This content is also available in:
![]() Italiano
Italiano ![]() Português
Português ![]() Deutsch
Deutsch ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
Uses of HPV testing alongside cytology
|
The principles of all these methods alongside cytology are similar:
- HPV is more sensitive than cytology for CIN2+
- Early detection of CIN2 is not an end in itself because almost half of CIN2 lesions would resolve naturally without treatment
- Detection of CIN2+ depends on sensitivity of colposcopy
- HPV specificity is considerably lower than cytology
- Most HPV-positive lesions represent transient infection
- Persistent HPV-positive lesions are at risk for progression
- HPV is not 100% sensitive for CIN2+, CIN3+ or cancer
HPV triage of ASC-US or LSIL cytology
Follow up of women with ASC-US or LSIL cytology can be done by repeat cytology, HPV testing or colposcopy.
ASCUS-LSIL triage study (ALTS)
The ASCUS-LSIL triage study (ALTS) randomised trial showed triage for high-risk HPV (hrHPV) using Hybrid Capture 2 (HC2) to be significantly more sensitive than repeat cytology in detecting CIN2+ (ALTS 2003a) but it was no more sensitive in detecting CIN3. The results suggested that around 40% of CIN2 lesions had regressed (Castle et al. 2009).
HPV triage was not recommended for LSIL, most of which was hrHPV+
HC2 versus APTIMA
A meta-analysis of the APTIMA HPV test, which tests RNA rather than DNA, showed similar sensitivity for CIN2+ and CIN3+ compared to HC2 for ASC-US and LSIL: all values were over 90% (Arbyn et al. 2013). Specificity ranged from 27.8% to 56.4% in the two arms of the APTIMA versus HC2 meta-analysis (Arbyn et al. 2013) and was higher for APTIMA.
|
UK sentinel site pilot study
The UK sentinel site pilot study of HPV triage of borderline and mild dyskaryosis (equivalent to ASC and LSIL) showed wide variation in HPV-positive rates, especially in borderline samples (39% to 73%), between laboratories (Kelly et al. 2011).
The main advantage lay in returning HPV-negative women and, depending on local protocols, HPV-positive women with no CIN at colposcopy to routine screening.
The positive predictive value of HPV-positivity for CIN2+ varied between 12% and 23% for CIN2+ and 4% and 12% for CIN3+ reflecting high false positive rates for HPV (Moss et al. 2004).
Summary of HPV ASC-US/LSIL triage
Challenges
|
Test of cure after treatment of CIN
The risk of recurrent CIN or cancer after treatment
- Women may be at increased risk of cancer for up to 20 years after treatment of CIN3 (Strander et al. 2007).
- A four-fold increased risk of cancer has been reported after treatment of any grade of CIN and three negative cytology tests (Rebolj et al. 2012).
- Among 15 studies with 2-year follow up, the risk of recurrent CIN varied between 4% and 18% (average 8%) in 15 studies (Flannelly et al. 2001).
These studies indicate the need for a test of cure that is more sensitive than cytology to reduce the need long-term follow up of all women after treatment.
|
HPV testing for test of cure needs to be highly sensitive since it aims to detect the small percentage of cases that recur after treatment in women at higher risk of cancer |
Protocols for test of cure
Protocols for test of cure after treatment of CIN usually recommend colposcopy if the cytology is either abnormal (ASC-US+) or negative and HPV+. The protocol in the NHSCSP for England can be accessed on http://www.cancerscreening.nhs.uk/cervical/hpv-triage-test-flowchart-201407.pdf
HPV testing has been shown by meta-analysis to be more sensitive (93% vs. 72%) and no less specific (81% vs. 84%) than cytology in this setting (Arbyn et al. 2012). Nevertheless, cytology is recommended along with HPV testing of negative samples (Zielinski et al. 2004).
Results of test of cure in the UK
Outcome may depend on which of several approved HPV tests is used, since they vary in rates of positivity. HPV positivity at 6 months in a multicentre Scottish study varied between 17% and 27% (Cubie & Cuschieri 2013). In one of the UK sentinel site projects, HPV positivity in cytologically negative samples was 14% with HC2 and 28% with Cobas 4800 (Innamaa et al. 2014).
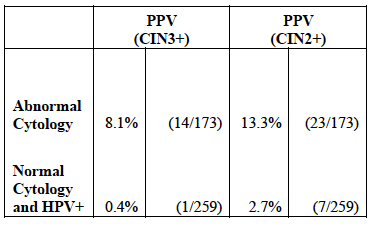
The results of test of cure in the NHSCSP sentinel sites report relatively little CIN2+ detected at colposcopy in HPV positive/cytology negative women: Moss et al. (2011) report 2.7% of CIN2+ in 12.1% of 3203 who were HPV-positive/cytology negative compared with 13.3% in 6.2% with abnormal cytology (Table 7-1).
Results of test of cure in the Netherlands
There has only been one study for as long as 10 years (Kocken et al. 2011): the results of this three-centre Dutch study of 435 women showed higher long-term detection of CIN3+ in 20% of women who were HPV+ at 6 months compared with 23% with ASC-US+; both groups had more CIN3+ than women who tested negative.
- Further tests were carried out at 12 and 24 months.
- The overall CIN2+ recurrence rate was 18% of which half (9%) was CIN3+ (including two squamous cell carcinomas).
- About half of recurrences occurred within the first 5 years after treatment including all the CIN3+ cases.
Risk of CIN3+ within 10 years according to results at 6 months (Kocken et al.):
29% of HPV-positive women (i.e. 6%)
13% of women with ASC-US+ cytology (i.e. 3%)
22.5% of women positive for either or both (i.e. 7%)
2.1% of HPV-negative women (i.e. 2%)
2.8% of cytology-negative women (i.e. 2%)
1.4% of double-negative women (i.e. 1%)
- Risk of CIN2+ recurrence after negative co-testing at 24 months or three negative cytology tests was similar to the risk of CIN2+ in the general population.
- As a result of this study the authors recommended co-testing at 6 and 24 months – or three cytology tests at 6, 12 and 24 months if HPV testing is not available.
Advantages of HPV test of cure
Challenges of HPV test of cure
|
HPV tests to resolve uncertainty
HPV tests are sometimes carried out to resolve uncertainty at the request of the gynaecologist at colposcopy.
A study in Manchester (Bowring et al. 2013) recorded the following groups:
- Persistent CIN1 (n=422)
- Recurrent low-grade after treatment of high-grade CIN (n=260)
- Low-grade vaginal vault cytology after hysterectomy (n=20)
- Women with a cervix difficult to access (n=44)
- Mismatch between high-grade cytology and colposcopy (n=9)
About half of the first group were HPV+ and one-third of the second group. Overall in the study, CIN2+ rates were 0.7% in HPV-negative compared with 8% in HPV+ women.
HPV testing to resolve uncertainty (e.g. persistent CIN1)
|