This content is also available in:
![]() Italiano
Italiano ![]() Português
Português ![]() Deutsch
Deutsch ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
Guidelines for taking cellular samples
Guidelines are available for taking samples for conventional cytology or liquid-based cytology, which are equally effective as long as the guidelines are adhered to (NHSCSP 2006); Arbyn et al. 2007).
Clinical conditions required for taking a sample
Cytology samples should be taken at mid-cycle: menstrual samples may obscured by blood and endometrial cells shed during the few days before or after menstruation may lead to cytological changes being misinterpreted.
Accurate information about the age and date of birth of the patient, date of last menstrual period, symptoms if present and previous screening history should be provided on the request form and may be relevant to the interpretation of cytological changes and the cytologists recommendation for follow up. For example, endometrial cells in a cytological sample only likely to be significant in women over 40 years of age but not otherwise.
|
Procedures for taking the sample
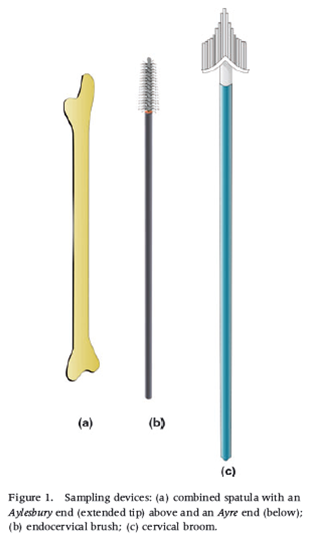
When taking a sample for conventional cytology the clinician or nurse will use an extended tip spatula or one or other end of the Ayre spatula depending on the age and parity of the patient, with or without a brush. The broom is used for liquid-based cytology (Figure 8.1).
Devices for collecting cervical cellular samples
- Aylesbury spatula (modified Ayres spatula) for sampling the cervix and transformation zone
- Endocervical brush to sample the endocervix.
- Cervical broom (LBC)
Once the sampling equipment is prepared, the clinician or nurse can prepare the patient for the procedure.
- A speculum is inserted into the vagina: the cervix must be clearly visualised using a direct light source and the cervical os should be located.
- The sampling device(s) used should be selected according to the shape and size of the cervix and the location of the squamocolumnar junction.
- The mucus plug is wiped away gently to make sure the spatula/brush is in direct contact with the epithelial surface; otherwise insufficient cells may be collected and the sample obscured by mucus and inflammatory cells.
- An Aylesbury spatula or the extended tip of the Ayre spatula is suitable for sampling the cervix of a young or nulliparous woman (Figure 8.3).
- The rounded end is used for a parous woman. A brush may be needed as well as a spatula to sample the cervix of a post-menopausal woman where the squamocolumnar junction lies within the endocervical canal (Figure 8.4 a and b).
- The broom device should be rotated 360 degrees five times to remove cells from the region of the transformation zone, squamocolumnar junction and endocervical canal. A broom may be used for a conventional smear (Figure 8.4 or liquid-based cytology (Figure 8.4.c and 8.6).
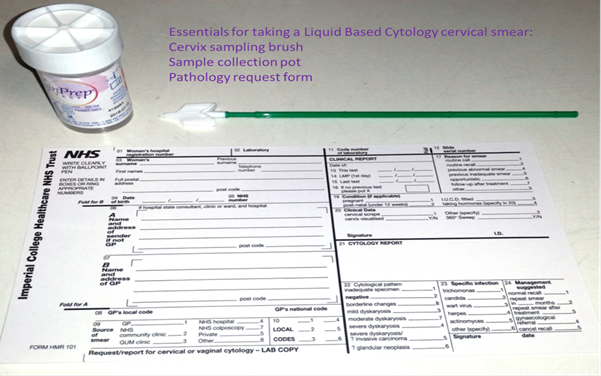
- The material on the spatula or brush must be transferred immediately to a glass slide for conventional cytology or to the liquid-based cytology vial for LBC cytology which has been previously labelled with the patients name and date of birth.
- As long as it can be done quickly enough before the cells of the first sample air dry, spatula and brush samples my be spread on the same slide (Figure 8.4 d.)
- For conventional cytology, the glass slide must be fixed immediately with an appropriate fixative (95% alcohol) and the slides transported to the cytology laboratory in a container for processing together with the corresponding cytology request form (Figure 8.5).
- Samples taken for LBC should be processed strictly in accordance with the manufacturers instructions. After sampling the cervix, the tip of the sampling device should be broken off into the transport medium in the container provided which should then be transported to the laboratory for processing if the Surepath method is being used. However if the ThinPrep method is being used it is of the upmost importance that the tip of the sampling device is not included in the container (Figure 8.6).
|
The spatula, brush or broom should be rotated 3600 more than once to ensure adequate sampling of the transformation zone If this is not adhered to there is the risk that the abnormal cells present on the cervix will not be sampled and therefore not end up on the slide. |
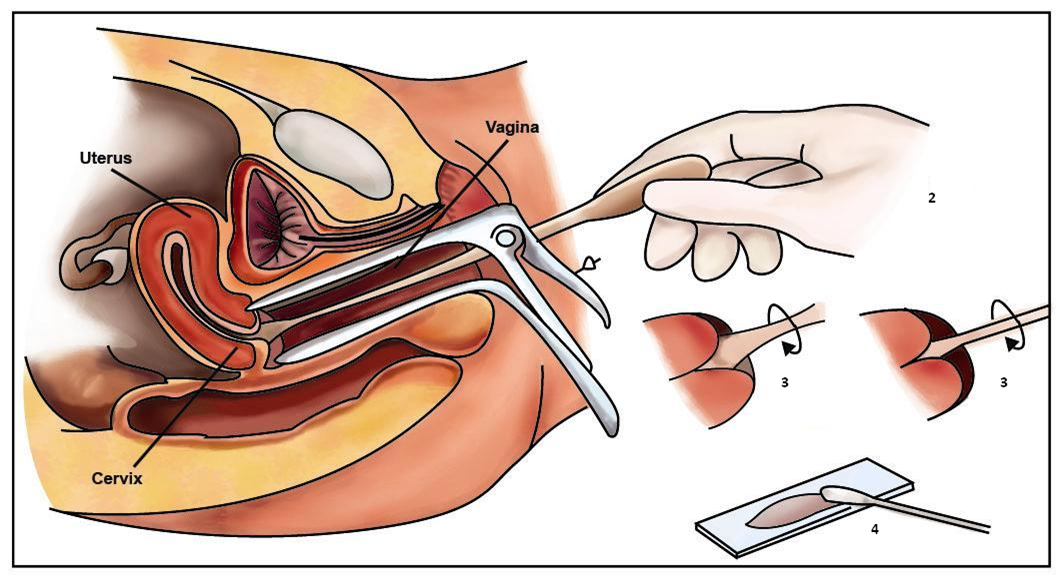
Figure 8.4. Using a spatula, brush or broom for taking and preparing a sample for a conventional smear (Figures 2, 4 and 5 from Arbyn et al. 2007)
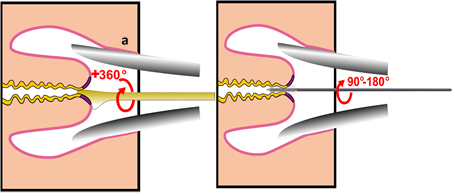
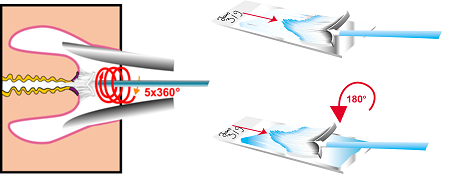
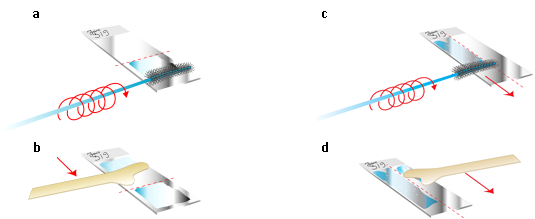
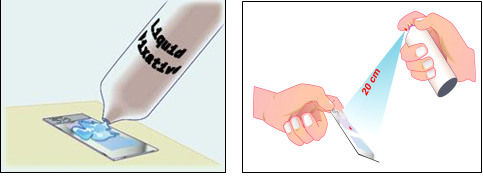
Figure 8.6. Rinsing the broom in commercial fixative using the manufacturers instructions for ThinPrep


Fixation of conventional smears
Adequate fixation is an essential step in the preparation of cervical smears. It ensures that the cells are well stained and clearly displayed for microscopic analysis and preserved for immediate and future review.
Fixation can be achieved by complete saturation or immersion of the slide in one of the many alcohol-based fixatives listed below for 15-20 minutes, after which the slide can be removed from the fixative and transported to the laboratory for staining. Alternatively, fixation can also be achieved by using a spray fixative (Figure 8.5).
Spray fixative consists of an alcohol base and carbowax that provides a thin protective waxy coat over the slide. The carbowax must be removed by immersion in alcohol before staining.
Recommended fixatives for conventional cytology:
95% ethanol (for optimal fixation)
80% isopropanol
95% denatured alcohol (90 parts 95% ethanol, five parts absolute methanol and five parts absolute isopropanol)
Reagent grade alcohol (absolute methanol, 80%isopropanol, 90% acetone)
Fixation must be immediate. The smear must not be allowed to air dry before fixation.
A satisfactory fixative for cytological specimens has to meet several requirements:
- It should penetrate the cell rapidly so that detailed cell morphology is maintained.
- Cell shrinkage should be minimal and uniform so that morphological distortions do not occur.
- It should allow permeability of dyes across the cell boundaries and appropriate for the staining method used.
- It should facilitate cell adhesion to the glass microscope slide.
- It should be bactericidal, non-toxic and permanent.
The advantages of liquid-based cytology (LBC)
|
Accuracy of LBC versus conventional cytology
Early studies suggested higher sensitivity of liquid-based cytology compared with conventional cytology in terms of detection of LSIL or worse although results varied between centres (Lee et al. 1997).
A meta-analysis a decade later showed no evidence of improved sensitivity or specificity but also reported considerable heterogeneity among studies (Arbyn et al. 2008). The National Institute for Clinical Excellence recommended LBC to be used in the NHS Cervical Screening Programme based on a Health Technology Assessment (Karnon et al. 2004).
|
The National Institute for Clinical Excellence (NICE) concluded that LBC was at least as sensitive and may be better than conventional cytology (2003) and had the other major advantages listed above. |
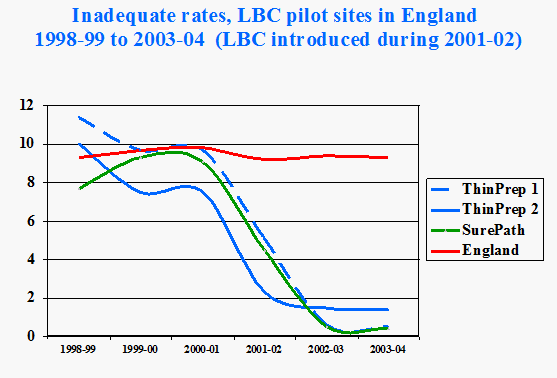
The main reason for introducing LBC in England was the striking fall seen in rates of inadequate tests from almost 10% to less than 2% (Figure 8.5), which was not seen in studies elsewhere in the world (Davey et al. 2006).
LBC virtually eliminates samples obscured by exudate, blood or air-drying artefact (Siebers et al. 2012) previously included in the satisfactory but limited by category.
Criteria for deciding the adequacy of a cytological sample will be dealt with elsewhere.