This content is also available in:
![]() Italiano
Italiano ![]() Português
Português ![]() Deutsch
Deutsch
Processing cytology samples involves reception of the specimen and request form, preparation of slides for microscopic examination, staining, screening and reporting the slides. All these processes are subject to quality control and quality assurance measures.
Reception of specimen and request form
- Details on specimen and form are checked to make sure they match.
- Specimen and form must have at least three patient identifiers (out of name, surname, date of birth, NHS number, hospital number).
- Laboratory reference number assigned.
- Patient ID and sample reference number entered on the laboratory information management system (LIMS).
Preparation of slides for microscopic examination
- Liquid-based slides are prepared using the equipment and manufacturers instructions. The most frequently used methods are ThinPrep (Hologic) and SurePath, whose manuals should be available in the laboratory and adhered to.
- Links to all ThinPrep equipment and methods for collecting samples are given on the main website: http://www.thinprep.com/hcp/ifu/
- Links to BD SurePath http://www1.bd.com/anz/training/surepath
Staining using the Papanicolaou method
- Regressive Papanicoloau method is shown in Table 8.xx as used in automated staining machines.
- All slides are mounted, coverslipped and labelled.
- Staining characteristics of individual nuclei and counterstains are checked on a daily basis
The Papanicolaou staining method
After years of experimentation, Dr Papanicolaou developed a trichrome stain, which until this day, is still used (although slightly modified). The trichrome stain is a combination of one nuclear stain, haematoxylin and two counterstains, OG-6 and EA-50. OG-6 stains keratin while EA-50, (a double stain, eosin and azure) stains the cytoplasm of squamous epithelial cells, nucleoli and red blood cells.
For optimal staining, the cells on the slide must not be allowed to dry before fixation or during processing as this will lead to unwanted artefacts. Modification of the stain is frequent for each laboratory prefers their own colour balance: adjustments can be made by altering the length of time in haematoxylin and EA-50.
Simple variations such as the chemical content of the tap water, ambient temperature, pH of specimen and number of slides stained per batch, can affect the colour balance of the stain. It is the laboratories duty, through quality control checks, to maintain a consistent staining intensity to facilitate consistent cytological diagnoses.
Providing that the nuclear detail is clearly defined and the transparency of the cytoplasm is maintained, inter-laboratory variation of the colour balance is acceptable.
Progressive or regressive staining
In using the progressive method, the intensity of nuclear staining is controlled by the immersion of the slide into a blueing agent after the nucleus has been stained to the required intensity with haematoxylin. The blueing agent most commonly used is Scotts tap water (pH 8.02). Progressive staining tints the cytoplasm very lightly.
When using the regressive staining method, the nucleus is deliberately over-stained with a non-acidified haematoxylin. The excess stain is removed with dilute hydrochloric acid solution (acid water). The decolourising process is then stopped by immersing the slide in running tap water. Timing is crucial in the regressive method as de-staining may lead to a hyperchromatic nucleus becoming hypochromatic.
One last variable for the Papanicolaou stain not only depends on the staining method used but also the commercial source of the stains and the pH of the cell sample. In consequence the Papanicolaou stain cannot be considered to be an exact stoichiometric stain.
Both methods work as well as each other, and depending on the laboratory, either one of these methods could be used. The overall staining results and diagnostic capabilities are comparable.
Characteristics of Papanicolaou stainingIndividual nuclei
Counterstains (cytoplasm)
The stains should be equal in intensity There should be cytoplasmic translucency with a sharp contrast to the nuclear stain |
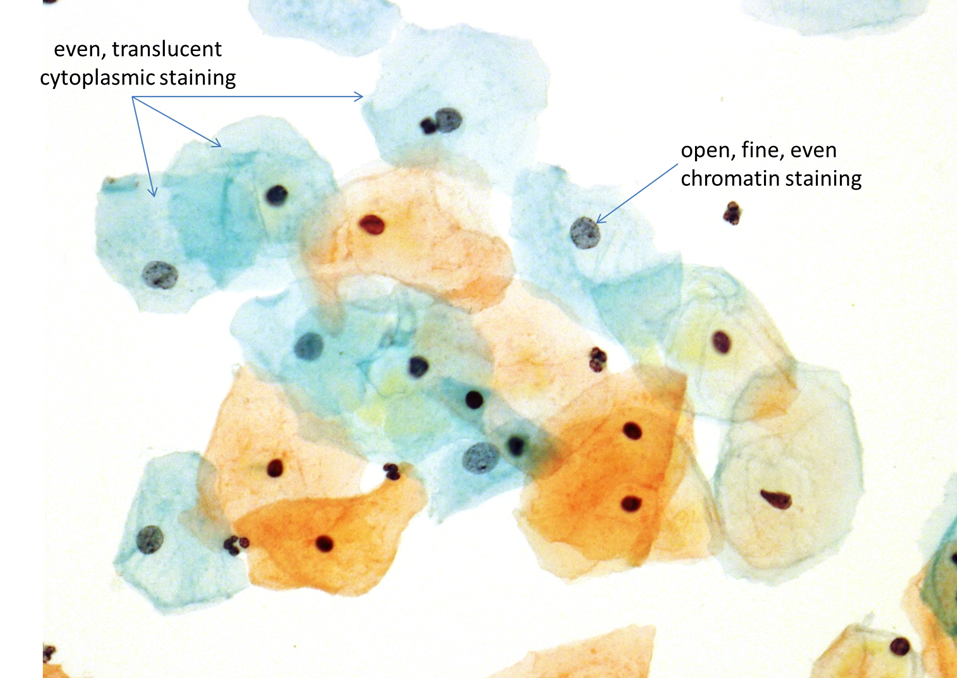
Table 8.1. Regressive Papanicolaou staining method (Automated staining machine)
|
Station |
Solution |
Time (minutes) |
|
1 |
95% Alcohol |
1:30 |
|
2 |
70% Alcohol |
1:30 |
|
3 |
Haematoxylin |
4:00 |
|
4 |
Acid water |
0:05 |
|
Wash 1 |
Water |
Wash |
|
Wash 2 |
Water |
Wash |
|
Wash 3 |
Water |
Wash |
|
Wash 4 |
Water |
Wash |
|
5 |
70% Alcohol |
2:00 |
|
6 |
95% Alcohol |
1:00 |
|
7 |
OG6 |
2:00 |
|
8 |
95% Alcohol |
0:10 |
|
9 |
95% Alcohol |
0:10 |
|
10 |
EA50 |
6:00 |
|
11 |
95% Alcohol |
0:15 |
|
12 |
95% Alcohol |
0:15 |
|
13 |
Absolute alcohol |
1:00 |
|
14 |
Absolute alcohol |
1:00 |
|
15 |
Absolute alcohol |
1:00 |
|
16 |
Xylene |
3:00 |
|
17 |
Xylene |
2:00 |
|
Exit |
Xylene |
1:00 |
Screening and reporting the cytology
- A cytotechnologist or cytology screener screens the slides.
- Depending on local protocols, all slides assessed as negative or inadequate are rapidly reviewed and any found to be abnormal are referred to a senior cytotechnologist for assessment.
- Negative and inadequate results are signed out according to local protocols,
- All abnormal cytology slides are referred to a consultant pathologist, senior scientist or advanced biomedical scientist practitioner depending on local protocols for issuing a final report.
- A final report is signed, recorded, and either sent by post or electronically dispatched to the smear taker.
- Final reports include a recommendation for management, such as referral for colposcopic examination or repeat test if the sample is inadequate.
- HPV testing is carried out if required for ASC-US/low-grade triage or test of cure after treatment of CIN.
- The patient is informed of the result of the test.
- The clinician or clinic submitting the sample is responsible ensuring appropriate action is taken in event of abnormal result unless other agreed written protocols are in effect for referral to colposcopy and requesting repeat tests.
- A system of reminders for colposcopy appointments and repeat tests should be in place.
These procedures may vary between laboratories regions and countries but should follow European guidelines for quality assurance of cervical cancer screening (Wiener et al.)
Protocols for screening conventional and liquid-based cytology
A screening and reporting protocols with integrated quality control measures should be implemented by the laboratory manager in collaboration with departmental consultant pathologists.
In order to develop expertise, cytotechnologists should see a wide range of cases. Laboratories should process at least 15,000 cervical smears per year and each screener may be expected to screen 50 (conventional) or 80 (LBC) smears per day with breaks at regular intervals. The screener should have his/her own workstation and binocular microscope and should aim to achieve a minimum of 3000 cases screened per year.
The prepared slides should be screened for abnormal cells using a x10 objective and x10 eye piece, the same objective should be used to screen the whole slide. The screener should progress field by field across the slide until the whole area under the coverslip has been inspected. It is usual to start screening at one corner of the slide and work in a stepwise manner until the whole area under the coverslip has been examined.
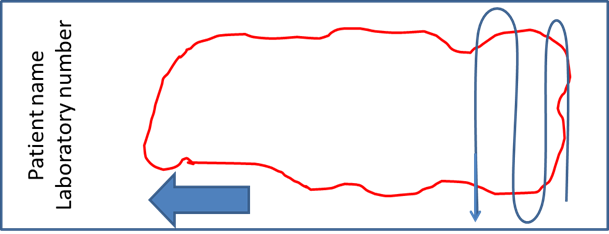
It has been estimated that a screener will have examined approximately 250-300 fields of view during the process of screening a single slide (using a x10 objective). The average time taken to complete this process for conventional cytology is 6-10 minutes (range 5 -20 minutes).
The duty of the screener is to mark cells of interest on the cervical smear. When marking or dotting a x4 objective should be used. The protocol for marking should be decided by the laboratory but coloured felt tip pens are normally used when screening LBC and white dotting ink is used when dotting a conventional smear. When inspecting areas or cells of special interest a x20 or x40 objective should be used.
The cytology request form and cervical screening history should be provided with each smear and should be reviewed by the cytologist before examining the smear.
Protocols for screening a ThinPrep slide
- Training must be available to cytologists converting from conventional smears to liquid-based cytology, whichever technology is used.
- ThinPrep uses a methanol-based fixative, which is different from the ethanol-based fixative of a conventional smear. Nuclear detail is well preserved in ThinPrep slides but the nuclear membrane is more distinct, which may affect the distinction between immature squamous metaplasia and HSIL.
- Screening ThinPrep slides may be done from side to side or up and down as preferred by the cytologist.
- No specific guidelines are available for rapid review or pre-view.
Protocols for screening a SurePath slide
- Training must be available to cytologists converting from conventional smears to liquid-based cytology, whichever technology is used.
- The fixative used in SurePath is ethanol-based and similar to that used in conventional cytology.
- Although the area of cells to screen in a SurePath preparation is smaller than that of a ThinPrep, the time taken to screen the slide should be no shorter: SurePath preparations are not monolayers and three-dimensional cell groups need to be focused at high-power scanning up and down the cell groups.
- Users of SurePath recommend a rapid screen of the whole slide followed by a slow screen taking careful note of three-dimensional cell groups. (personal communication N. Dudding]
- No specific guidelines are available for rapid review or pre-view.
Training for liquid-based cytology
|