This content is also available in:
![]() Português
Português ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
Whatever the setting, the confidence of the colposcopist or gynaecologist and their reliance on a cytology report depends on the sensitivity and PPV.
- Cytology slide review allows potential false positive features to be recognised before treatment is carried out.
- Equivocal cytology reports may be given more definitive reports on review allowing the correct treatment to be carried out.
- Definitive cytological features may be presented and confirmed at MDT meetings allowing treatment to be planned even when the lesion cannot be seen at colposcopy.
- False negative cytology may be presented and discussed during the historical review of slides reported before a diagnosis of cervical cancer.
- Review of equivocal cases and recognised pitfalls provides colposcopists and other professional groups with insight into difficult areas of cytology.
- High-risk HPV positivity may support a diagnosis of HSIL or CIN but does not confirm it; nor does high-risk HPV negativity refute it.
Figure 12.1. Potential pitfalls to be reviewed at MDT meeting
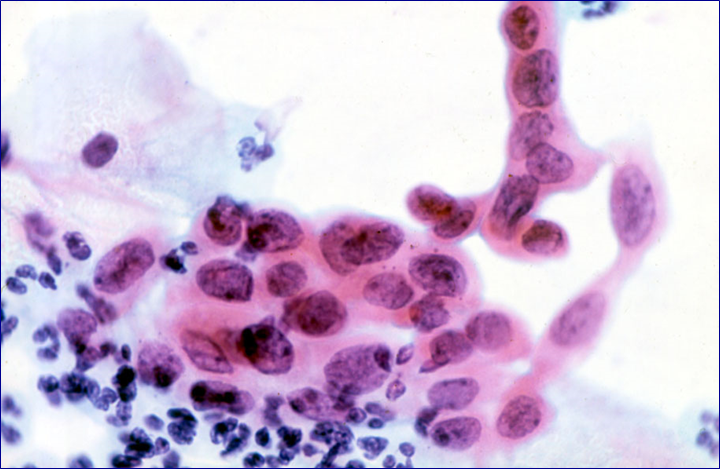
However, the diagnosis of CIN2 was doubted when this case was reviewed as a teaching case several years later and most likely represents immature metaplasia. It would now be resolved by p16/Ki67 staining (see below).
A decision to carry out a LLETZ was based on colposcopic appearances as well as the cytology report and is typical of cases requiring multidisciplinary discussion.
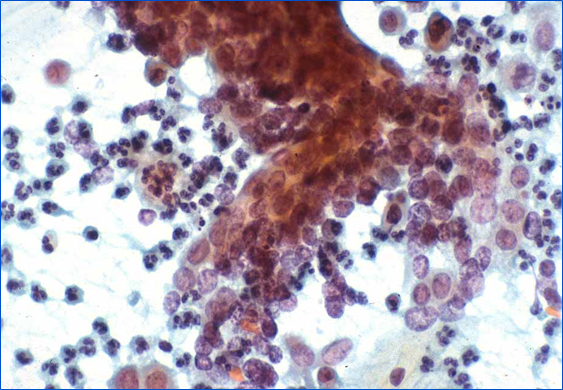
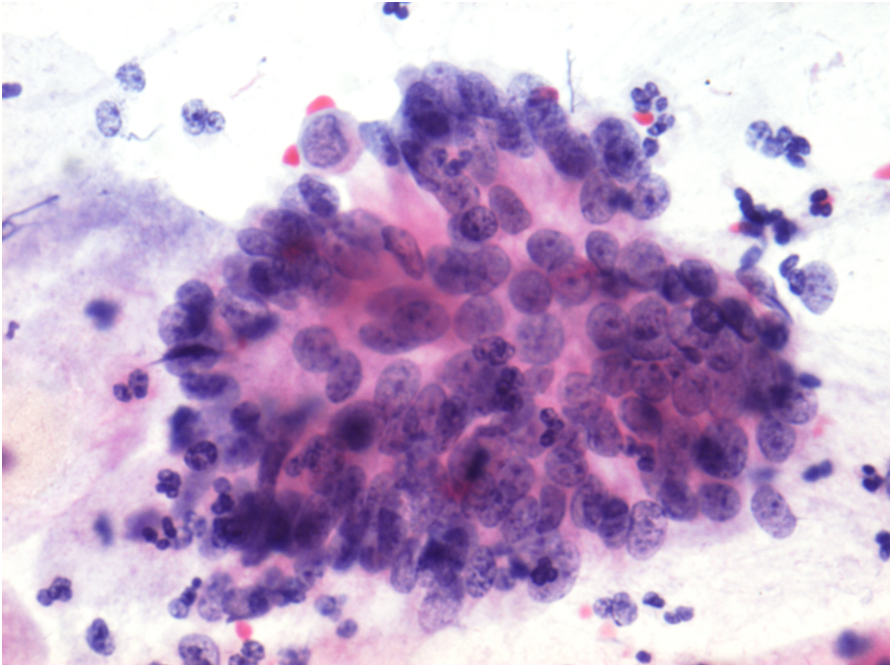
Hyperchromatic crowded cell groups
The diagnosis of HSIL in Figure 12.2 was confirmed as CIN3 but represents a difficult diagnosis warranting MDT discussion alongside full slide review and presentation of other findings.
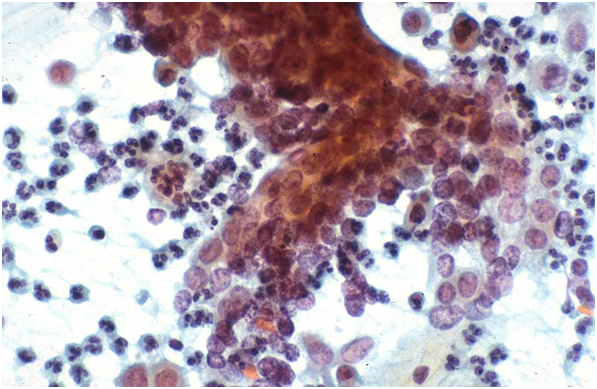
Alternatively, such changes could be seen when previous negative or atypical slides are reviewed from a patient who subsequently develops HSIL or cancer.
Hyperchromatic crowded cell groups are known to be at risk for a false negative diagnosis in conventional smears and liquid-based preparations (Demay 2000; Gupta et al. 2013).
This cell group could be misinterpreted as a cluster of endocervical cells – but close review shows severely dyskaryotic cells at the edge of the group of cells; similar cells are likely to be found on careful search of the rest of the slide.
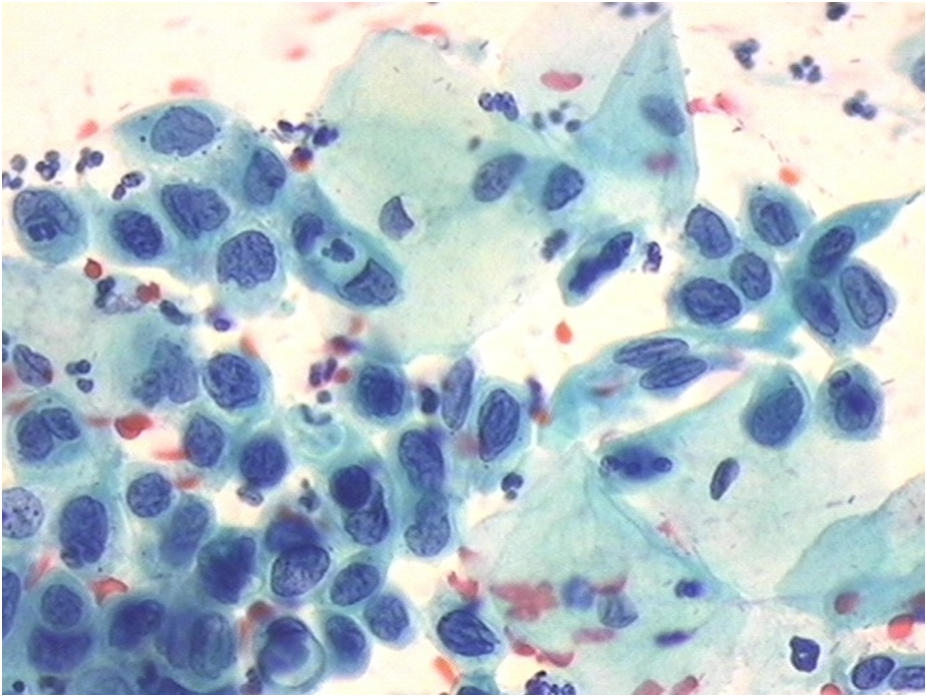
Definitive cytological diagnoses confirmed at MDT meeting
Classic appearances of HSIL and AIS respectively may have been well represented on the cytology slides even if not widespread, reported unequivocally and confirmed on review.
Colposcopy may be negative in such cases, particularly if the lesion is high in the endocervical canal: a biopsy may be inadequate or negative. Glandular abnormalities are known to be difficult to identify and sample at colposcopy.
Diagnostic LLETZ may be considered in such cases even if a punch biopsy does not identify the lesion.
Cytology review for MDT meetings
|