This content is also available in:
![]() Italiano
Italiano ![]() Português
Português ![]() Deutsch
Deutsch ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
Principles of screening
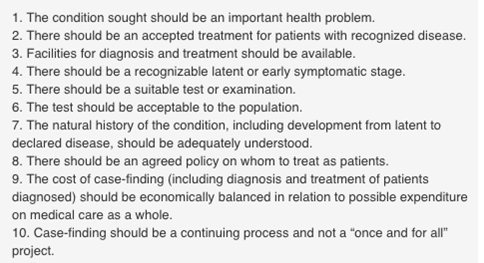
With reservations predicted by the authors at the time, cytological cervical screening has to a major extent fulfilled the criteria defined by Wilson & Jungner (1968) (Figure 5.1).
These principles have been revisited more recently by Andermann et al. (2008) in the knowledge of high-risk HPV being a necessary cause of cervical cancer and its precursors (Walboomers et al. 1999).
Cervical screening has been instrumental in the prevention of a condition that was (and in the absence of screening is) an important health problem.
Increasing knowledge about the natural history of the disease has raised problems (management of reversible vs. progressive lesions) and provided alternative solutions (vaccination and HPV testing) that are in the process of integration with cytological screening.
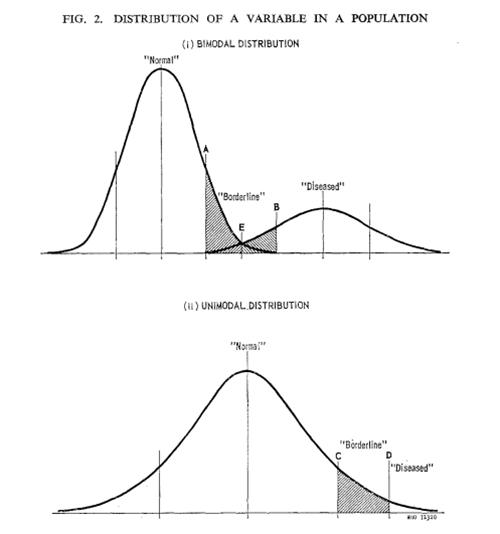
Wilson & Jungner recognised the snags of screening especially with respect to avoiding harm to those persons not in need of treatment. Their graph reproduced below (Figure 6.2) demonstrates the problem we now have in detecting a condition in what has been shown to have a bimodal distribution of high-grade pre-cancerous lesions developing in a background of far more prevalent and predominantly reversible human papillomavirus (HPV) infection.