Frankly invasive carcinoma is usually diagnosed in women with symptoms suggesting cancer but cytology may sometimes be taken as part of the investigation. Cytology is regarded as unreliable in clinical cancer because associated haemorrhage and inflammation tends to obscure the nuclear detail.
A recent study from the NHS Cervical Screening Programme has shown that cytology in symptomatic young women (20-29 years) with cancer may be more reliable than formerly thought (Landy et al. 2015). It should be noted that the majority of cancers at that age are likely to be early cancers (stage IA or IB) rather than advanced clinical cancers.
Microinvasive (stage IA) squamous cell carcinoma almost always develops in a background of extensive CIN3, which is the abnormality likely to be seen in cytology samples. Women with stage IA are likely to be asymptomatic and their cancers screen-detected by cytology.
Women with early invasive cancer (IB1) may also be asymptomatic and detected on cytology. Occult cancers are not clinically evident when the cytology sample is taken.
Although symptoms should always be investigated whatever the result of the cytology, an abnormal result may expedite diagnosis.
| Cervical cytology in women with invasive cancerCytology may be unreliable in clinically advanced cancersFrankly invasive carcinoma can only be suggested on cytology as morphological features overlap with HSILMicroinvasive carcinoma (stage IA) is a diagnosis that can only made on histologyMicroinvasive carcinoma usually develops in a background of widespread CIN3, which is the lesion seen as HSIL on cytology |
Cytology of invasive squamous cell carcinoma
Presentation
In a frankly invasive carcinoma, tumour diathesis and/or necrosis is likely to be a feature. (It is rare to find a malignancy with a completely clean background, but it can happen). Diathesis is the product of the breakdown of necrotic tissue, which forms a granular and proteinaceous precipitate with variable staining. As the tumour breaks down and ulcerates, it tends to haemorrhage so blood and its by-products are seen in malignant samples. Nuclear and cytoplasmic remnants as a result of necrosis, as well as inflammatory exudate, are a feature of the cytological background.
Tumour diathesis may be less obvious in liquid-based compared with conventional cytology; and most of the red blood cells and inflammatory cells will have been removed during processing.
The amount of material present in the sample obviously varies and this is due to the location of the tumour, its size, associated cytological contaminants (blood, inflammation, necrosis etc.) and the sampling technique.
Attention should be paid to the clinical presentation when suggesting invasive carcinoma on cytology.
Nucleus
Hyperchromasia is a constant feature of malignant squamous cells.
Chromatin distribution varies in cells within same groups, sheets or singly distributed cells. Some cells will show fine granular chromatin, some coarse granular chromatin and some will have opaque, marginated chromatin; its distribution will be irregular. Nuclear clearing and varying numbers of macro-nucleoli may be present – especially in poorly differentiated tumours.
The number of nuclei per cell can vary from a single nucleus to multiple nuclei.
Frequent mitoses and abnormal mitoses are a feature of invasive malignancy.
Cytoplasm
As described and illustrated below, the cytoplasm varies between being plentiful in keratinising and large cell non-keratinising squamous cell carcinoma and inconspicuous in small cell carcinoma. Thus the NC ratio varies between these types of carcinoma.
| Cytological features suggesting invasive squamous cell carcinomaTumour diathesis, haemorrhage and necrosisPleomorphic hyperchromatic nucleiIrregularly dispersed chromatin with nuclear clearingProminent irregular often multiple nucleoliKeratinisation of cells and keratinous debrisFrequent mitosis |
Keratinising squamous cell carcinoma
Presentation
Due to the exophytic nature of keratinising SCC, the tumour is usually directly sampled rather than shed or exfoliated so the presentation on the cytological preparation may be quite cleanThe majority of tumour cells will present singly and in sheets. In LBC preparations there will be a higher percentage of single cells due to the mechanical forces placed on the specimen during preparation. The cells will have size variation and bizarre/pleomorphic shapes. Free keratin, parakeratosis and hyperkeratosis may be seen as well as individually keratinising cells.
Nucleus
The nuclei are hyperchromatic with coarse granular chromatin, nuclear clearing and irregular chromatin distribution. It is rare to see macronuclei in keratinising cells but they may be seen in poorly differentiated cells in the same sample.
Cytoplasm
The cytoplasm is thick, dense and refractile. Importantly the density will vary between malignant cells. The staining will be variable but there should be a high number of orangeophilic malignant cells compared with basophilic or cyanophilic cells.
The NC ratio is variable from cell to cell and may be low because keratinising cytoplasm may be abundant.
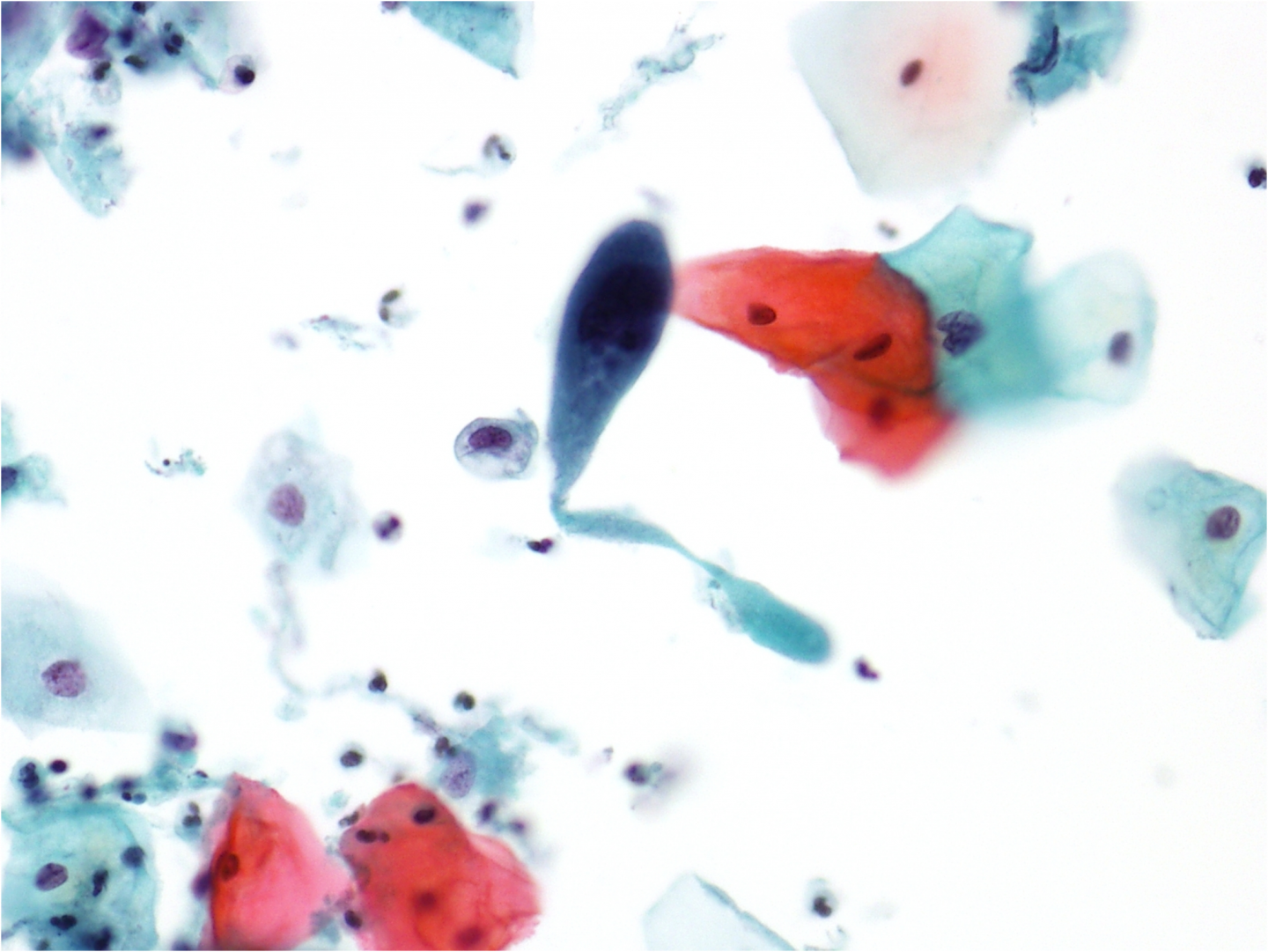
Figure 9c-19 (a-c). Keratinous background in squamous cell carcinoma
(a) Low-power view of an LBC sample showing tissue fragments, orangeophilic cells, clusters of polymorphs and necrotic debris
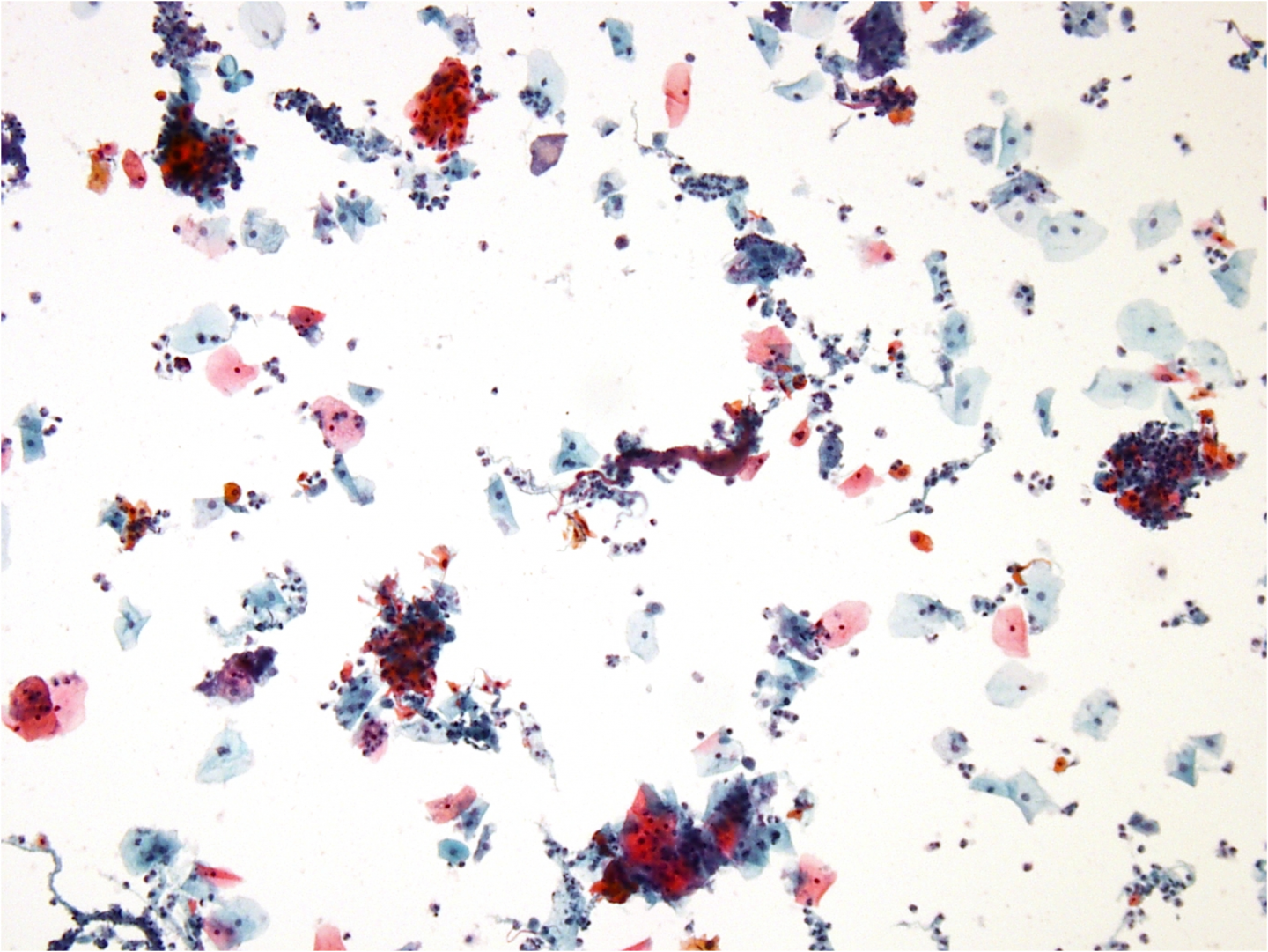
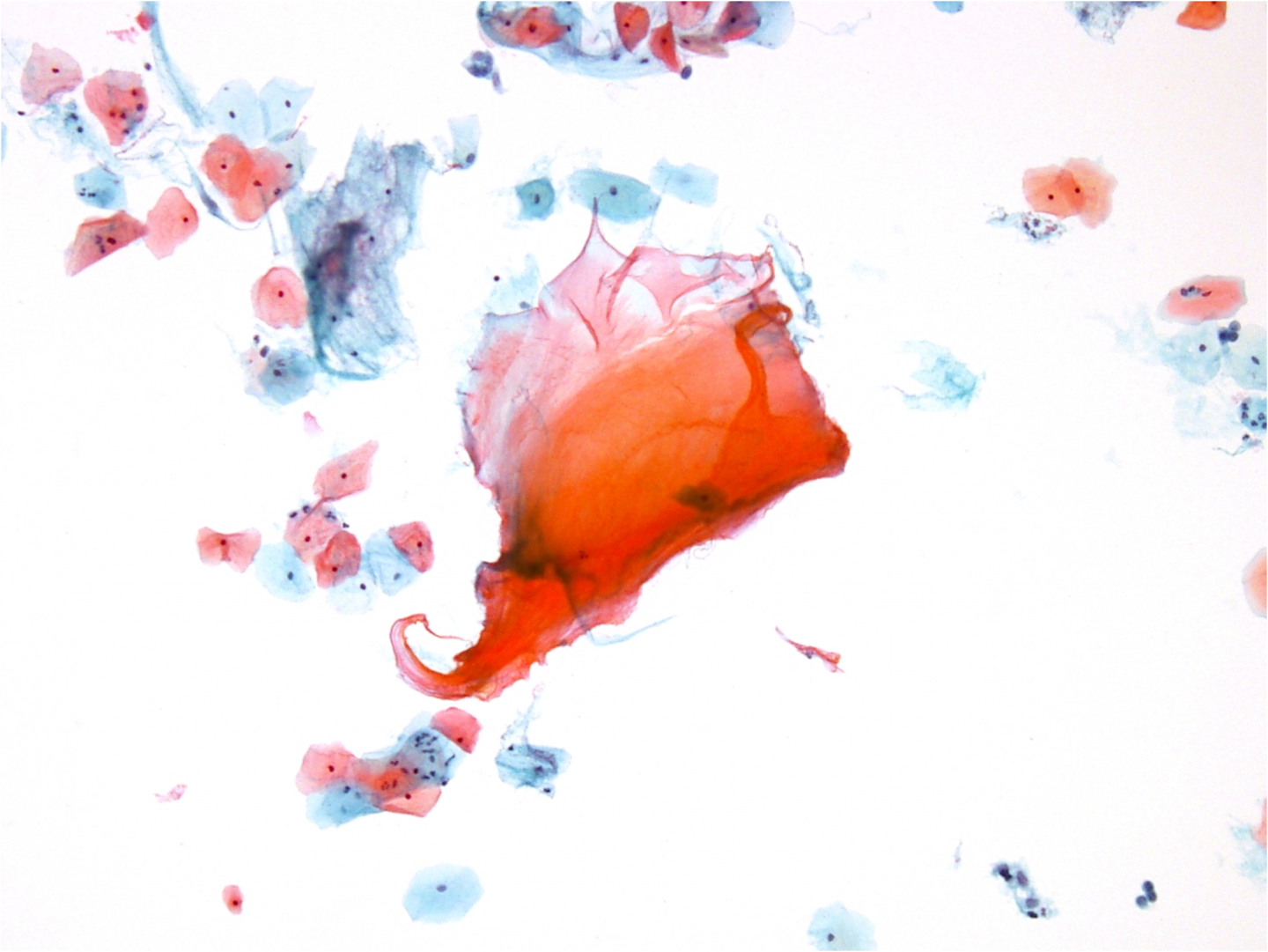
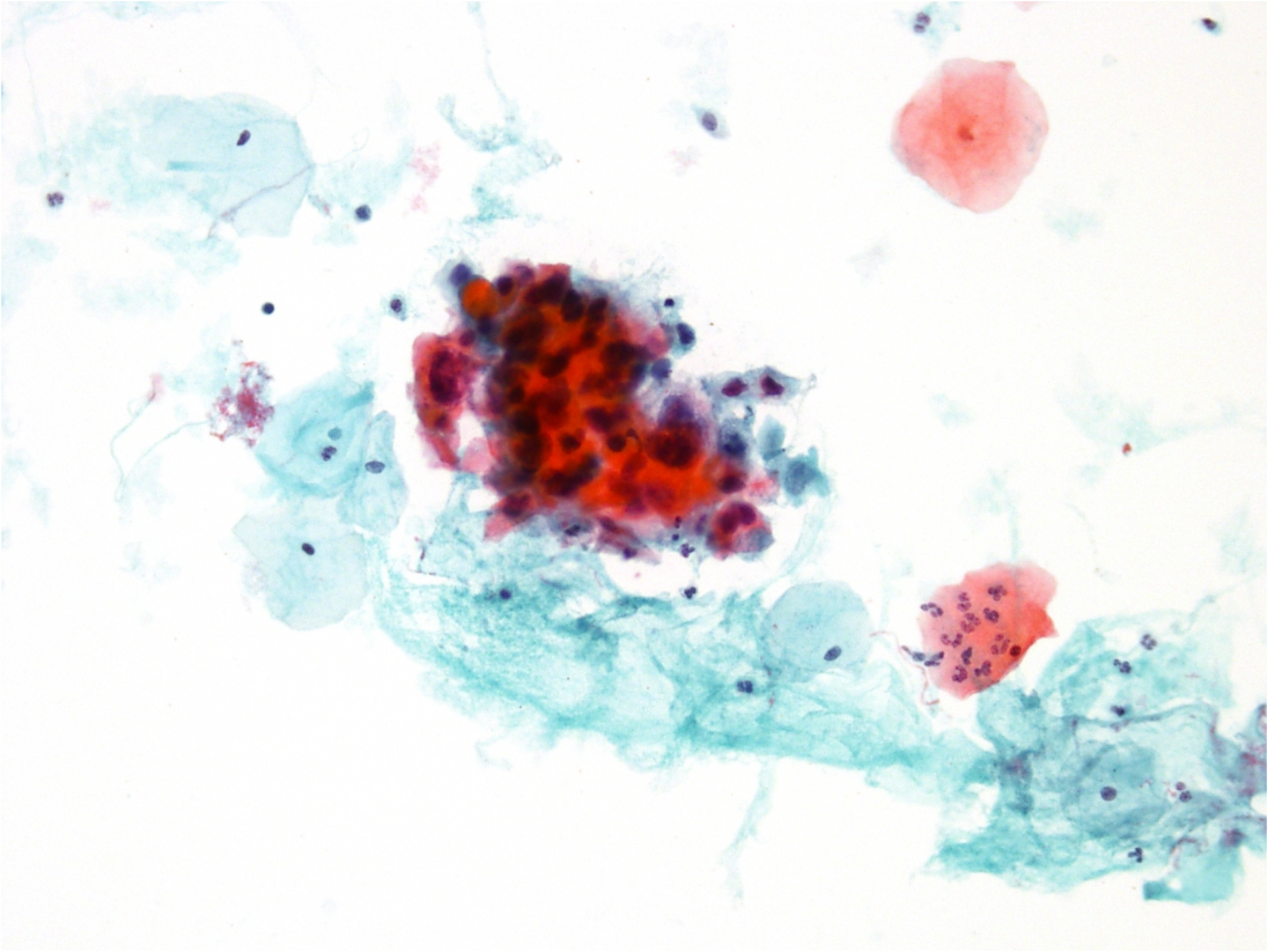
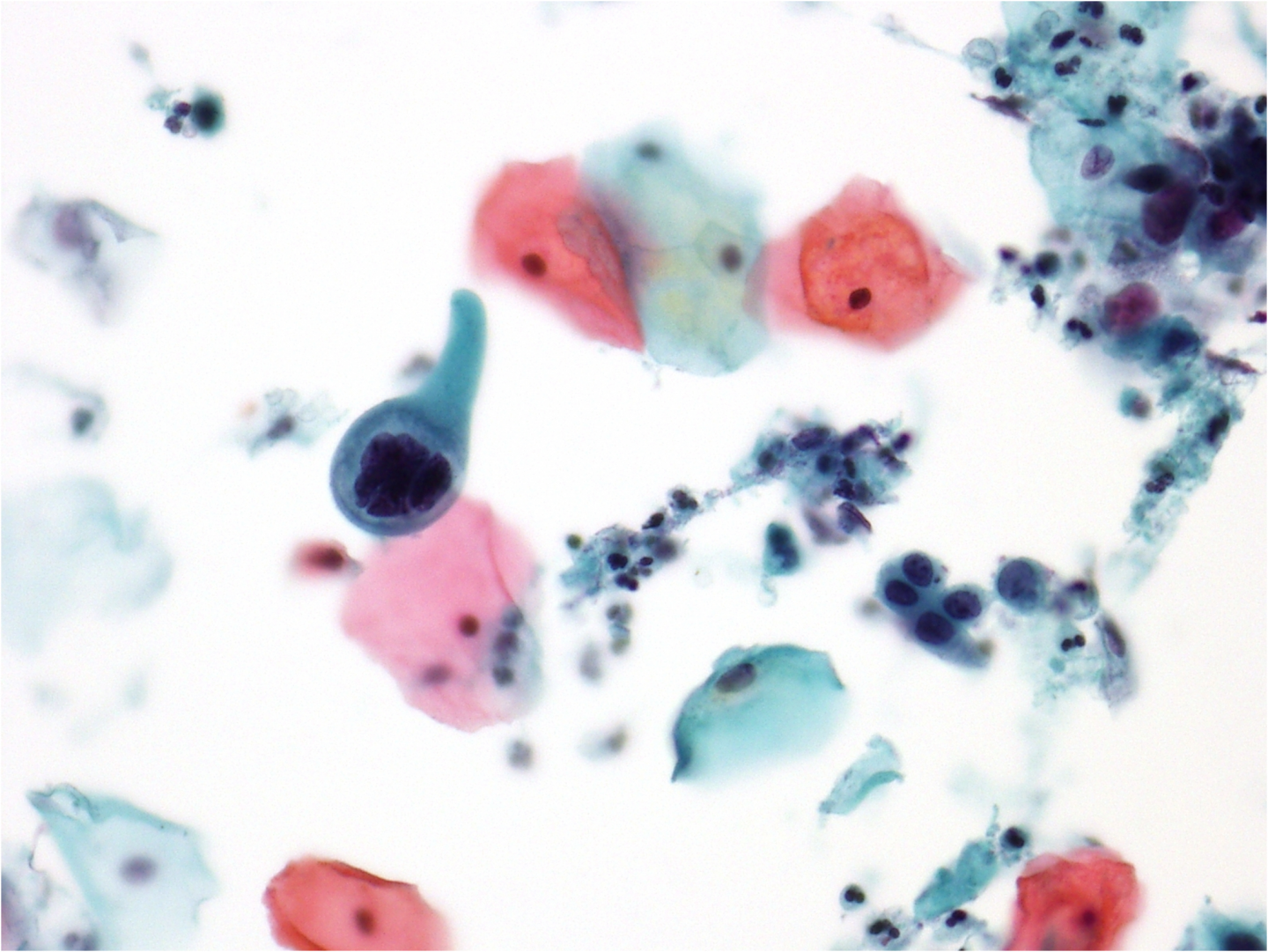
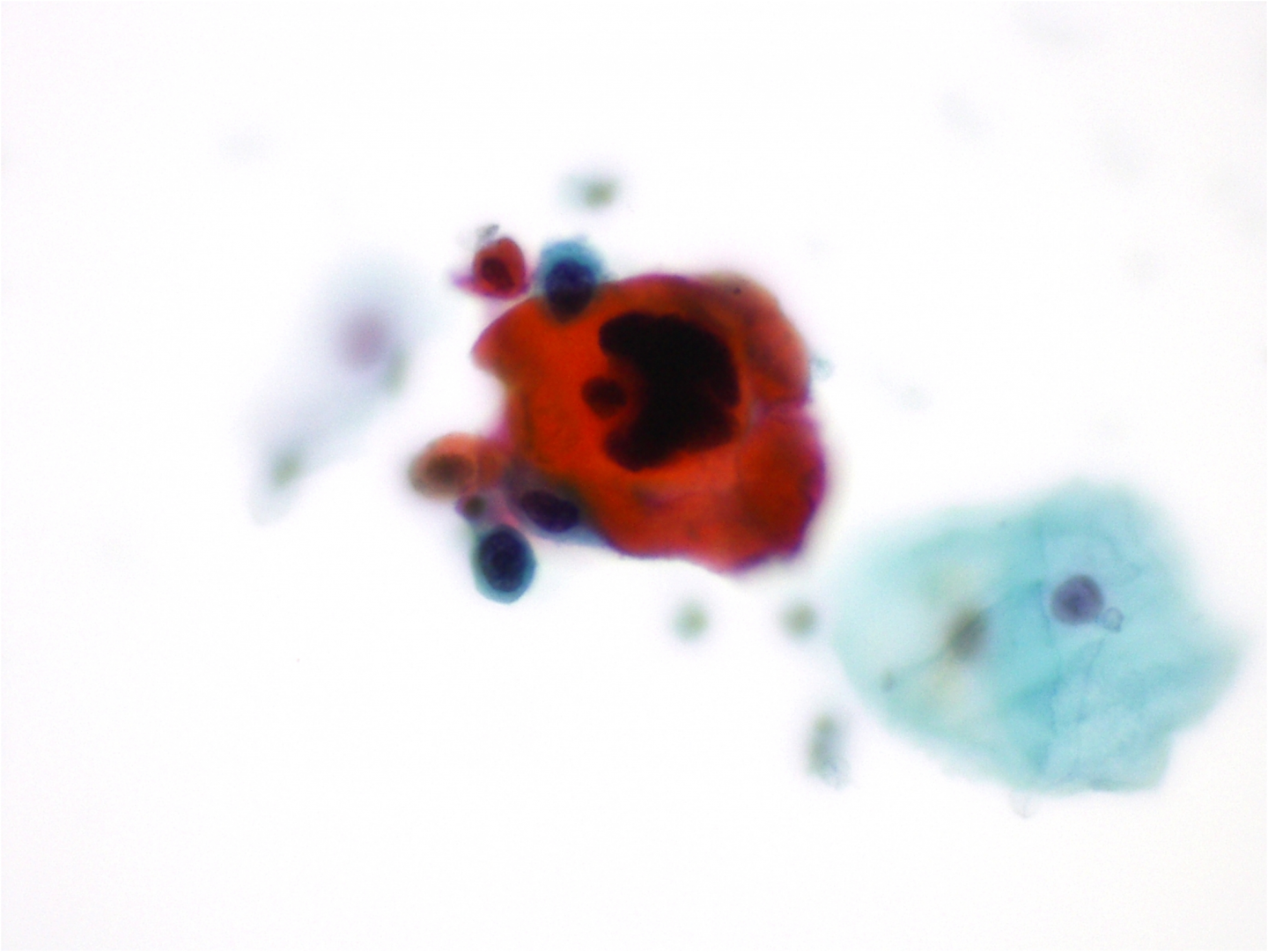
Figure 9c-20 (a-e) Cell types in keratinising squamous cell carcinoma
(a) Pleomorphic multiple nuclei in a malignant cell with copious basophilic cytoplasm
Squamous cell carcinoma without keratinisation
Presentation
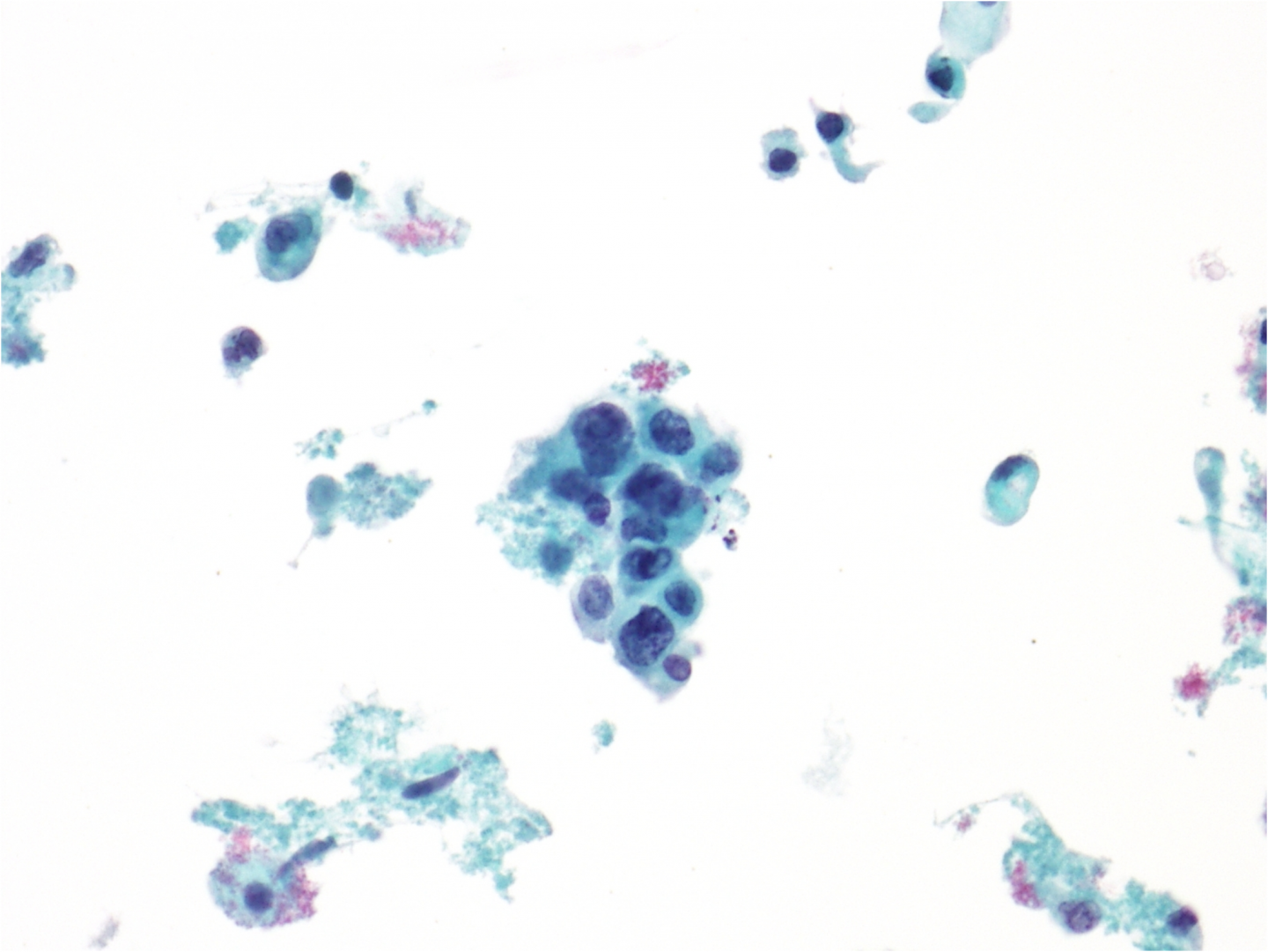
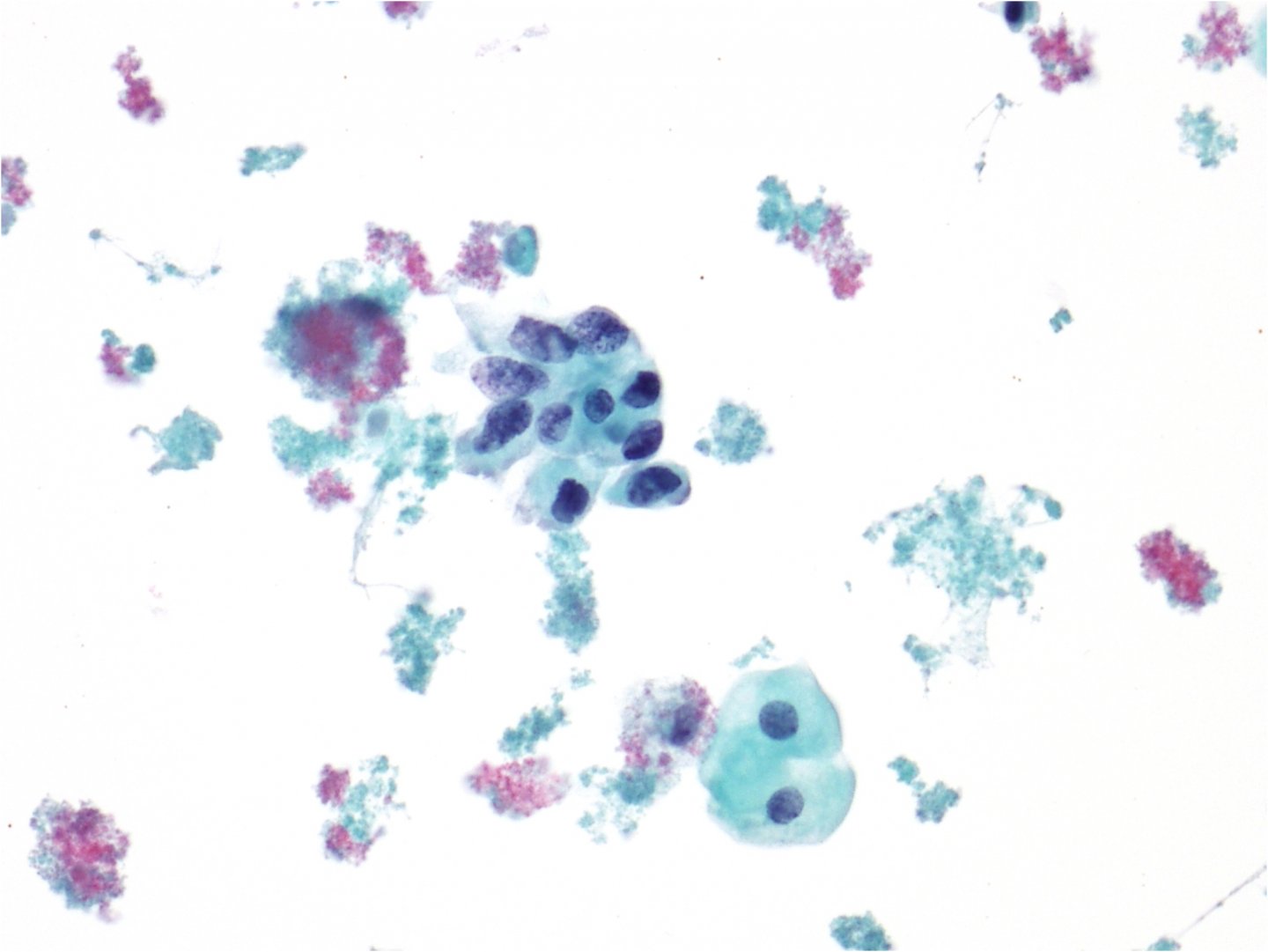
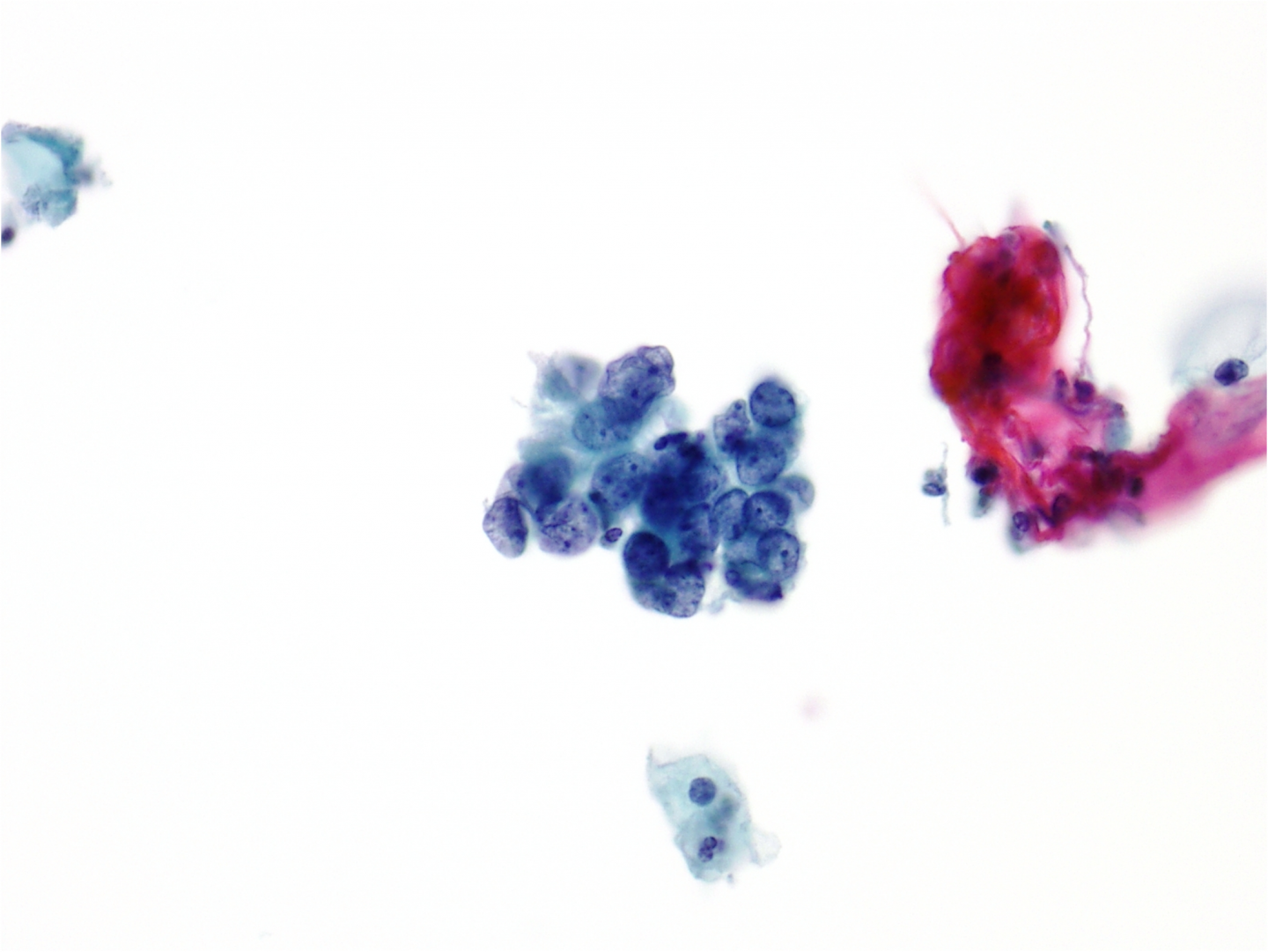
Presentation may vary between well-differentiated and poorly differentiated carcinomas. Well-differentiated non-keratinising carcinomas may show cohesive cell groups with well-defined cell borders similar to those seen in HSIL. In poorly differentiated carcinomas the cell borders are indistinct and the cytoplasm delicate and fragile. It may be very difficult to distinguish a poorly differentiated non-keratinising carcinoma from adenocarcinoma. Macronucleoli may or may not be present.
Tumour diathesis and a host response (inflammation) are common in non-keratinising squamous cell carcinomas. Depending on sampling technique there may be abundant material on the preparation. Due to the vascular nature of the tumours bleeding often occurs when sampling so the sample may be blood stained.
Nucleus
The nuclei are hyperchromatic with variation in size and shape. When shed in groups or sheets, the nuclei will be crowded and overlapping with loss of polarity.
Chromatin is usually coarse, granular and unevenly distributed throughout the nuclei – but it may appear evenly distributed in some cases.
Nucleoli are usually prominent. Macronucleoli may be a feature: they are unevenly distributed within the nuclei and will vary in number between nuclei.
Cytoplasm
The cytoplasm is lightly basophilic in well-differentiated non-keratinising carcinomas and may be inconspicuous and colourless in a poorly differentiated carcinoma.
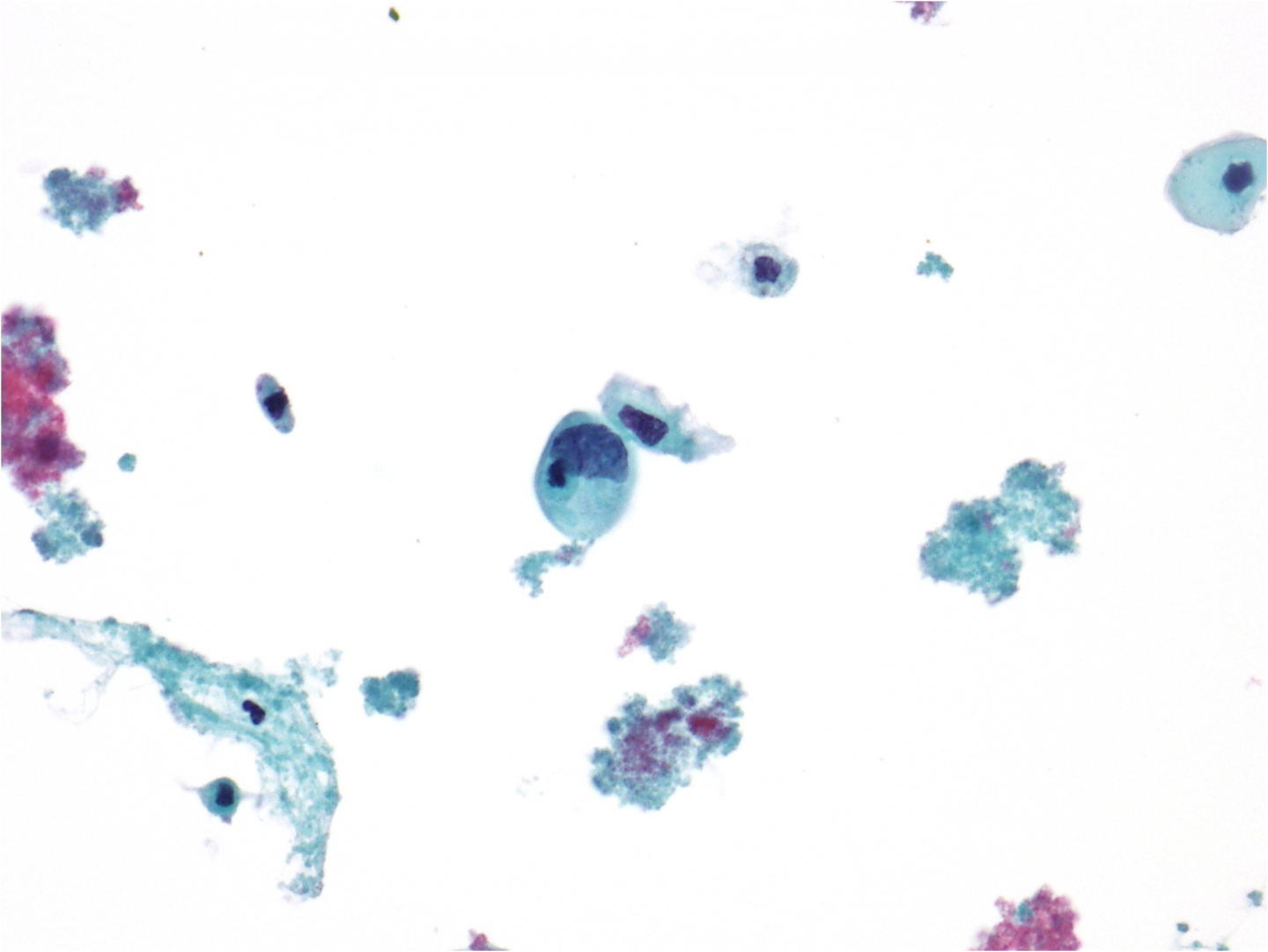
Figure 9c-21 (a-d). Non-keratinising squamous cell carcinoma
(a) Tumour diathesis seen alongside severely dyskaryotic cells with prominent nucleoli in an LBC preparation.
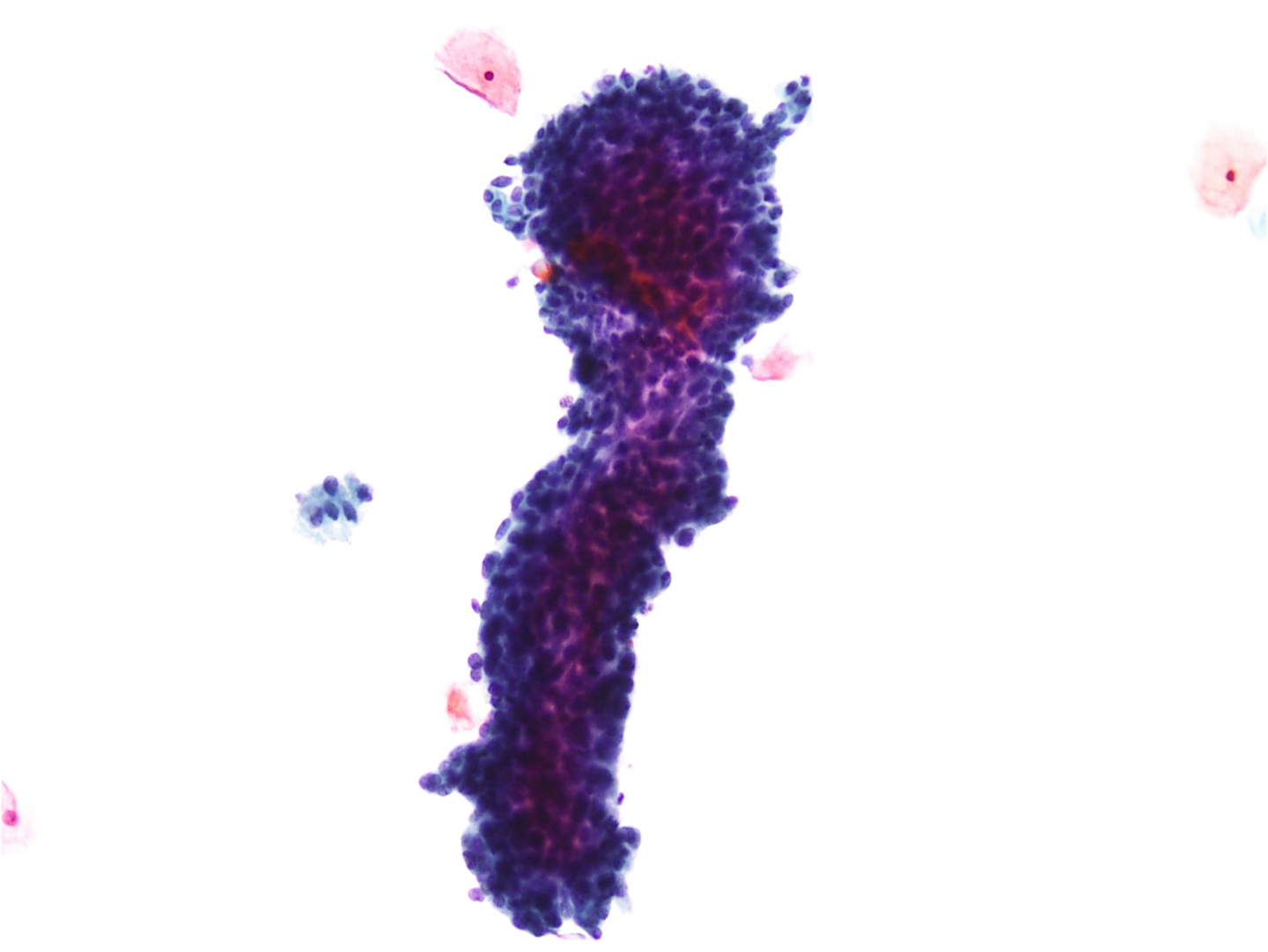
Small cell (neuroendocrine) carcinoma
Presentation
The term small cell carcinoma refers to highly aggressive carcinomas with neuroendocrine differentiation. These carcinomas are rare (<2% of invasive cervical cancers) and are similar to small cell carcinomas of the lung. They are rarely diagnosed on cytology (Ciesla et al. 2001). Cytologically, these tumours present with dispersed hyperchromatic small to medium sized cells with scant cytoplasm and a high NC ratio. Loose and cohesive clusters with nuclear moulding may be seen. Tumour diathesis is usually present. The cells within the groups/clusters are crowded and show no architectural integrity. Blood is often associated with this tumour.
Nucleus
The nuclei are small, round to oval and relatively uniform in size. They are hyperchromatic but the degree of hyperchromasia varies between cells. The chromatin is finely granular and irregularly dispersed with prominent chromocentres but inconspicuous nucleoli. Nuclear moulding is seen in cell clusters. Mitoses may be frequent.
The nuclei are larger (twice the size of a normal intermediate cell nucleus) than described in the small cell type of HSIL.
Cytoplasm
The cytoplasm is scant, delicate with indistinct margins.