This content is also available in:
![]() Italiano
Italiano ![]() Português
Português ![]() Deutsch
Deutsch
The effect of screening on incidence and mortality of carcinoma of the uterine cervix is difficult to establish because there was no randomised trial before it was started. In some countries screening has been in place for more than 50 years although it may have been poorly organised in the past, or more recently organised on the background of opportunistic screening in countries where the risk of cancer and its precursors was changing.
Effect of prevalence of high-risk HPV on cervical cancer rates
|
Organised screening programmes
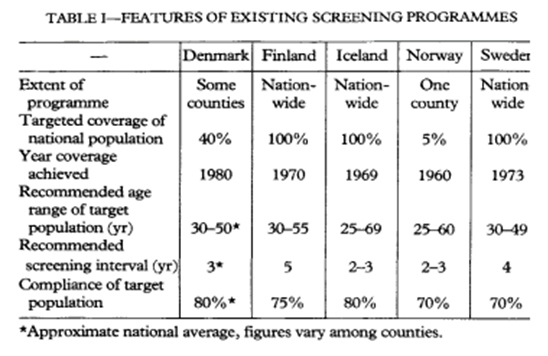
Nordic countries (Denmark, Finland, Iceland, Norway and Sweden)
The results were complicated by various factors (Figure 6.1):
- Problems with cancer registration in early years
- Spontaneous screening being carried out in addition to organised screening in all Nordic countries with the exception of Iceland
- Different age ranges and screening intervals
- Compliance with the programme in the five countries
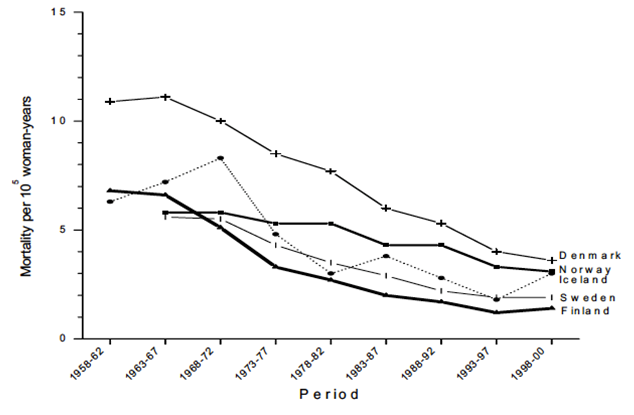
Furthermore, mortality may have already been falling in older women who had not been screened, and was rising in women aged 20-29 in Finland, Norway and Sweden, which will be considered in more detail later in this chapter.
Once screening became organised in all these countries, mortality fell to current levels below 5 per 100,000 women (Figure 6.2).
The effect of organised screening in UK
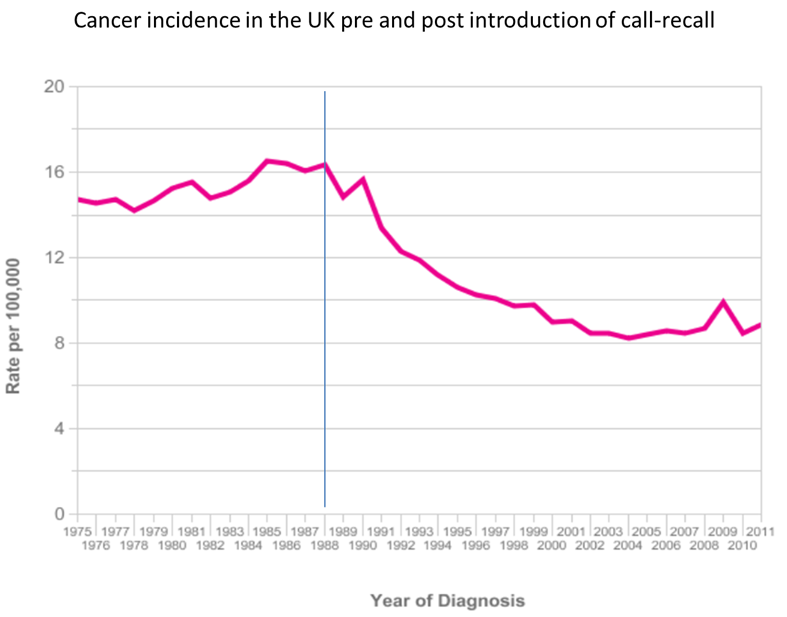
Incidence and mortality in the UK as a whole showed little change during the 1970s and 1980s when there were approximately 4000 cases and 2000 deaths per year – with a slight increase towards the end of the 1980s (Figure 6.3).
However, this apparent lack of effect of screening during the 1970s and 1980s was not constant across the UK: successful screening in Aberdeen, Scotland was comparable to that of Finland and Iceland providing a shining example to be followed nationally (Figure 6.4; Macgregor et al. 1985).
The NHS Cervical Screening Programme was launched in 1988: computerized call and recall for all women aged 20-64 years had a dramatic effect during the following decade (Figure 6.3).