Sources of error
- Inadequate training and update of pathologists, particularly those with little interest in cervical cytology.
- Insufficient confidence to question screeners and cytotechnologists.
- Lack of experience of benign reactive changes leading to over-reporting of atypical or borderline changes.
- Excessive workloads, inadequate laboratory space and equipment may affect performance of any level of staff.
- QC and QA of final reports issued from the laboratory
Principles
- Regular communication between cytotechnologists and pathologists, using multiheaded microscopes, to discuss challenging cases before the reports are issued provides a day-to-day method of quality control.
- Quality assurance of final reports based on histological outcome requires standard terminology, accurate record keeping and access to colposcopy findings and histopathology results.
- As explained elsewhere, it is impossible to measure sensitivity without knowing the prevalence of high-grade abnormalities and cancer in the population screened as negative. Surrogate methods are used such as monitoring reporting rates and comparing them with regional and national standards (Wiener et al. 2007).
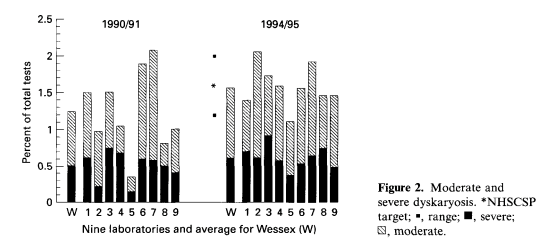
Reporting rates for high-grade cytology may be compared between pathologists for internal QA or, as a form of external QA between laboratories and regional or national standards.
Considerable variation in high-grade reporting rates in nine laboratories, with an overall population of 1 million people, moved close to the target NHSCSP range through inter-laboratory collaboration and comparison of reporting rates during a five-year period (Figure 11.4; Butland & Herbert 1996).
Reporting rates for low-grade and borderline / atypical cytology may provide information about reporting profiles, excessive use of borderline / atypical categories.
Inadequate reporting rates provide an indicator that may be useful for monitoring sample-takers as well as laboratory performance.
Positive predictive value of samples reported as high-grade dyskaryosis that are found to be CIN2+ at colposcopy provide a surrogate measure of specificity (reflecting false positives).
Achievable standards in terms of histological outcome: The NHS Cervical Screening Programme in England provides 5-95% percentiles as achievable standards for PPV, referral value (RV) and inadequate rates as measures of performance (Figure 11.5). Increases in RV reflect a change to HPV triage, with greater numbers of women with borderline change and low-grade dyskaryosis referred to colposcopy on first occurrence. PPV and RV both measure cytology laboratory performance in terms of histological outcome, giving a more objective measure of performance than reporting rates alone (HSCIC 2014).
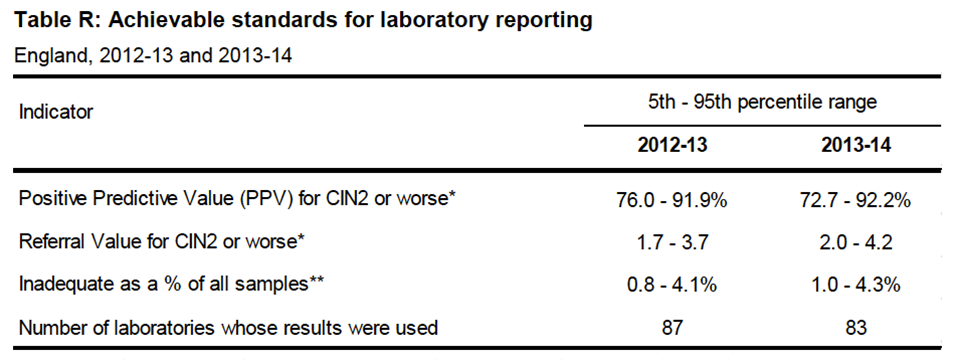
* Number of women referred to colposcopy to detect one case of CIN2+
?** % of samples from GP and community clinics
| Quality Assurance of cytology laboratory reportingHigh-grade, low-grade and inadequate reporting rates provide a measure of individual and laboratory performanceStandards based on histological outcome such as positive predictive value and referral value provide more objective measures of performance |