This content is also available in:
![]() Italiano
Italiano ![]() Português
Português ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
Atypical squamous cells of undetermined significance (ASC-US)
- ASC-US (or borderline changes in squamous cells) border on LSIL and can largely be resolved by HPV triage.
- HPV negativity would usually exclude minor changes in mature or intermediate squamous cells without koilocytosis (the only diagnostic feature of HPV infection).
- Minor nuclear enlargement and hyperchromasia is frequent in peri-menopausal women but may end up being reported as ASC-US.
- Minor changes of HPV, confirmed on high-risk HPV triage, should be managed by investigation if they persist as for LSIL.
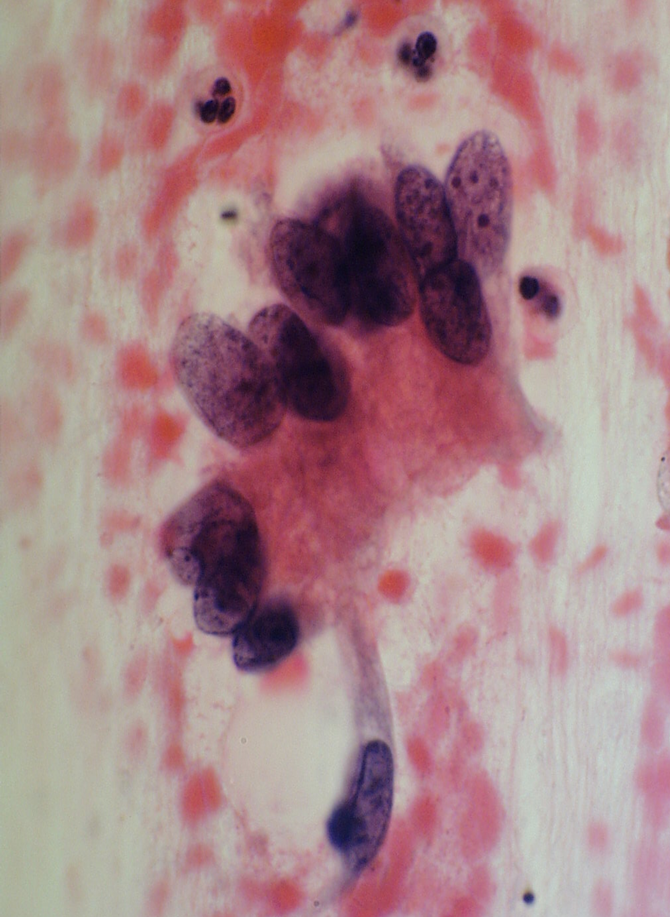
Figure 10.9 Examples of ASC-US bordering on normality and LSIL
How to avoid unnecessary ASC-US reports
|
Atypical squamous cells, cannot exclude HSIL (ASC-H)
- The whole slide should be examined carefully to look for recognizable HSIL to avoid unnecessary ASC-H reports.
- ASC-H is reported when features of HSIL are uncertain after consideration of all the conditions discussed above as potential false negatives and false positives.
- It is easy to see how Figures 10.1 (b), 10.2 (a-b) and 10.3 (a-c) could have been reported as ASC-H if these cells were representative of the most abnormal cells on the slide. Indeed, some of them were reported as ASC-H, which may avoid false negative reports in difficult cases.
- Equally, in some examples of immature squamous metaplasia, tubal metaplasia and lower uterine segment sampling it may be difficult in practice to avoid an ASC-US or ASC-H report as in Figures 10.5 (c-d), 10.6 (b), 10.8 (b) and 10.9 (b).
- Colposcopy and slide review of cytology and histology can avoid unnecessary treatment in potential false positive cytology cases.
- Monitoring HSIL rates for laboratories and individuals can be used as a method of quality control.
Atypical glandular cells (AGC)
AGC presents a two-fold problem in the context of false negatives and false positives:
- Distinguishing benign or metaplastic processes from neoplastic glandular cells as in Figure 10.11 (a-b).
- Distinguishing reactive glandular cells from HSIL as in Figure 10.5 (c).
Classical features of AIS must be distinguished from reactive endocervical cells, tubal metaplasia and TEM by attention to the chromatin pattern, palisading arrangement of cells and absence of stromal cells or cilia.
Clinico-pathological correlation and slide review before treatment is the key to avoiding over- or under-treatment of difficult glandular abnormalities.
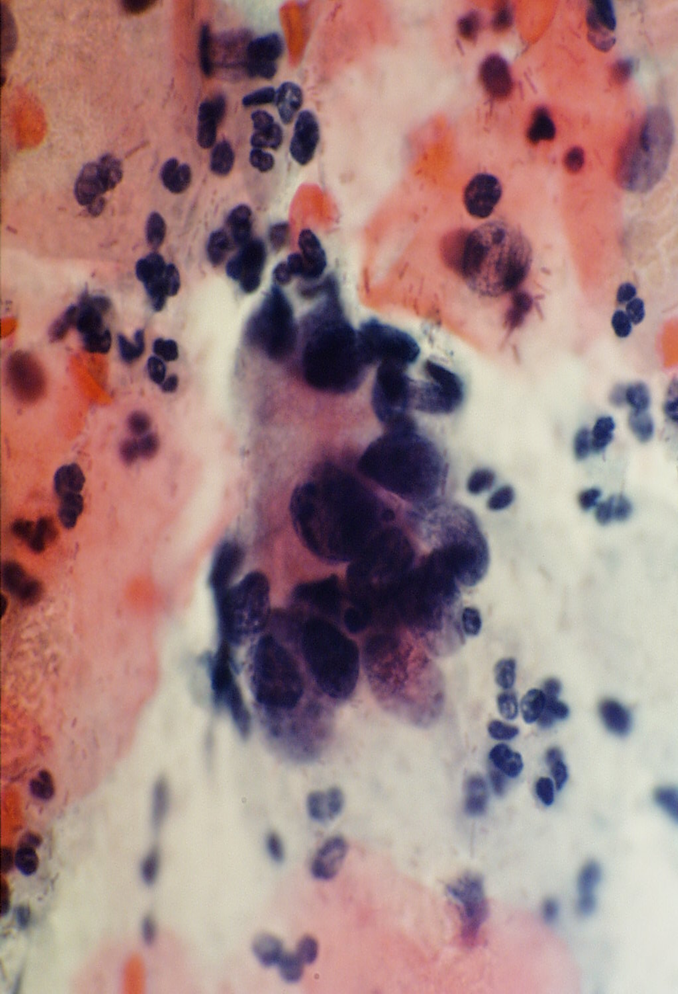
Figure 10.11 Atypical glandular cells favour neoplasia

How to avoid unnecessary ASC-H and AGL reports
|
Learning points from Chapter 10
|