This content is also available in:
![]() Português
Português ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
MDT meeting provide an opportunity to review biopsy diagnoses in the context of other findings and confirm or, if necessary, revise the reports before management is decided.
The accuracy of cervical punch biopsies depends on that of sampling, processing and interpretation of the samples. In a meta-analysis carried out in 2012, pooled sensitivity for CIN2+ on definitive histology was 92% and specificity 25%: sensitivity was lower and specificity higher for biopsies done immediately before excision (Underwood et al. 2012).
The NHSCSP invasive cervical cancer audit requires review of all biopsies and cytology samples reported within 10 years of diagnosis. A review of discrepancies found on review of 5159 histology specimens reported 6% of histology reports revised on retrospective review: 15% of CGIN and 12% of CIN3 were upgraded to cancer (Castanon et al. 2012).
Inter-observer variation of punch biopsies and LLETZ specimens was shown to be similar to LBC cytology (kappa values ranging from 0.44 to 0.49); agreement improved with increasing grades of CIN (Stoler et al. 2001).
CIN3 is the most robust histological diagnosis and an indication for treatment on diagnosis. However, CIN2 is intermediate in a spectrum that in reality consists of two entities: potentially reversible and genuinely precancerous lesions.
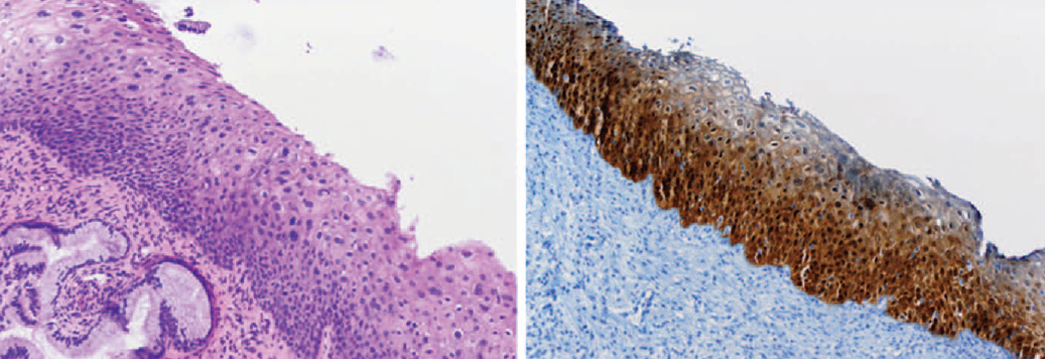
P16INKA4 staining improves the reliability of diagnosis of CIN2 as a high-grade precancerous lesion and is recommended in the LAST guidelines (Darragh et al. 2012). Ki67 staining carried out along with p16 is also recommended in this situation (Wentzensen et al. 2012).
Biopsies results in the MDT setting
|