Clinical features
- Generally in adolescents
- The least aggressive of the malignant germ cell tumours in children
- Found in the ovary and pineal region
- Testicular tumours are rare at this age
- Rarely as a component of a teratoma
- 15% bilateral (in patients with gonadal dysgenesis)
- Serum elevation of lactic dehydrogenase and isoenzyme-1
Fig 66 – Germinoma – High cellular smear composed of large single cells with abundant cytoplasm admixed with lymphocytes. Tigroid background (Giemsa)
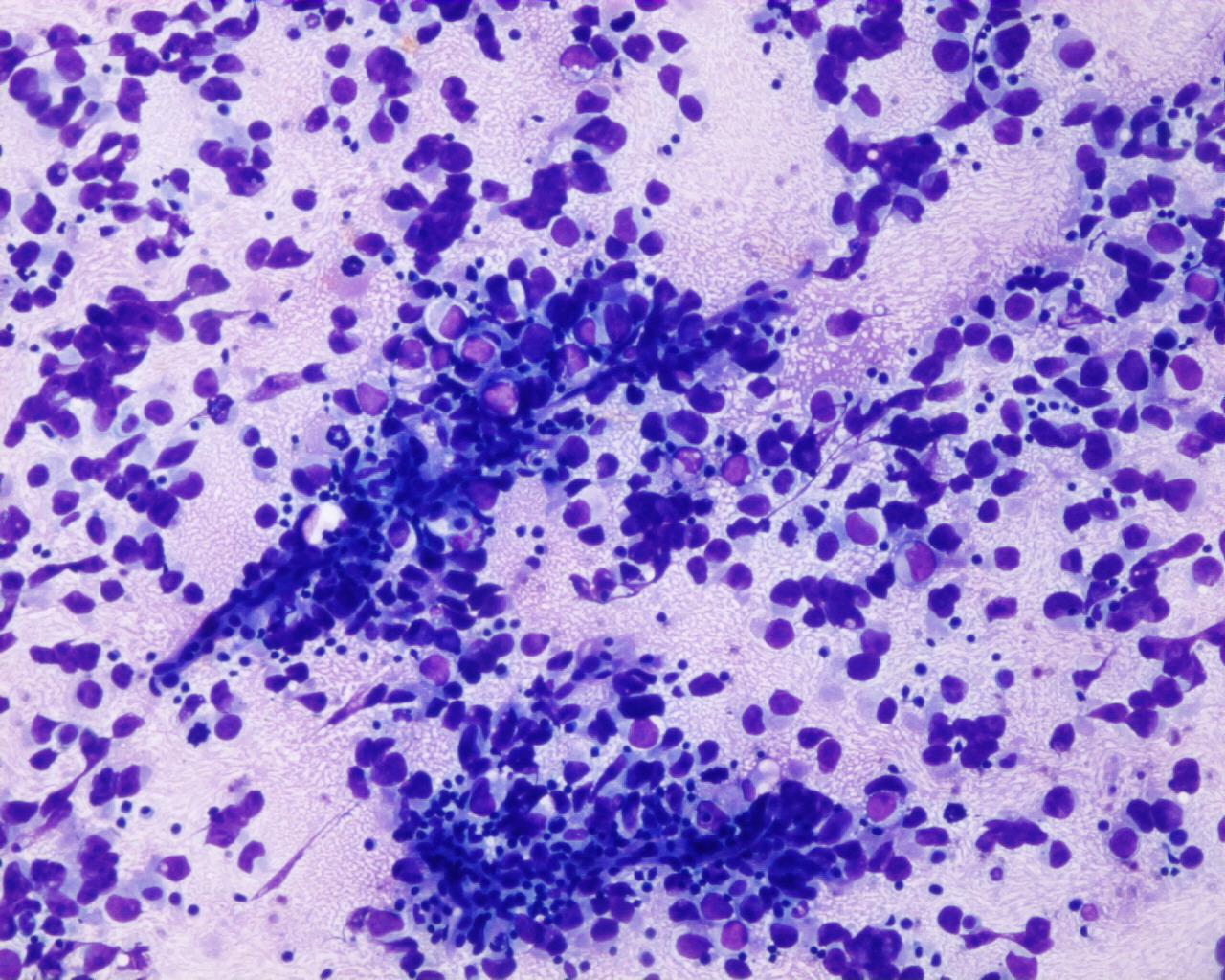
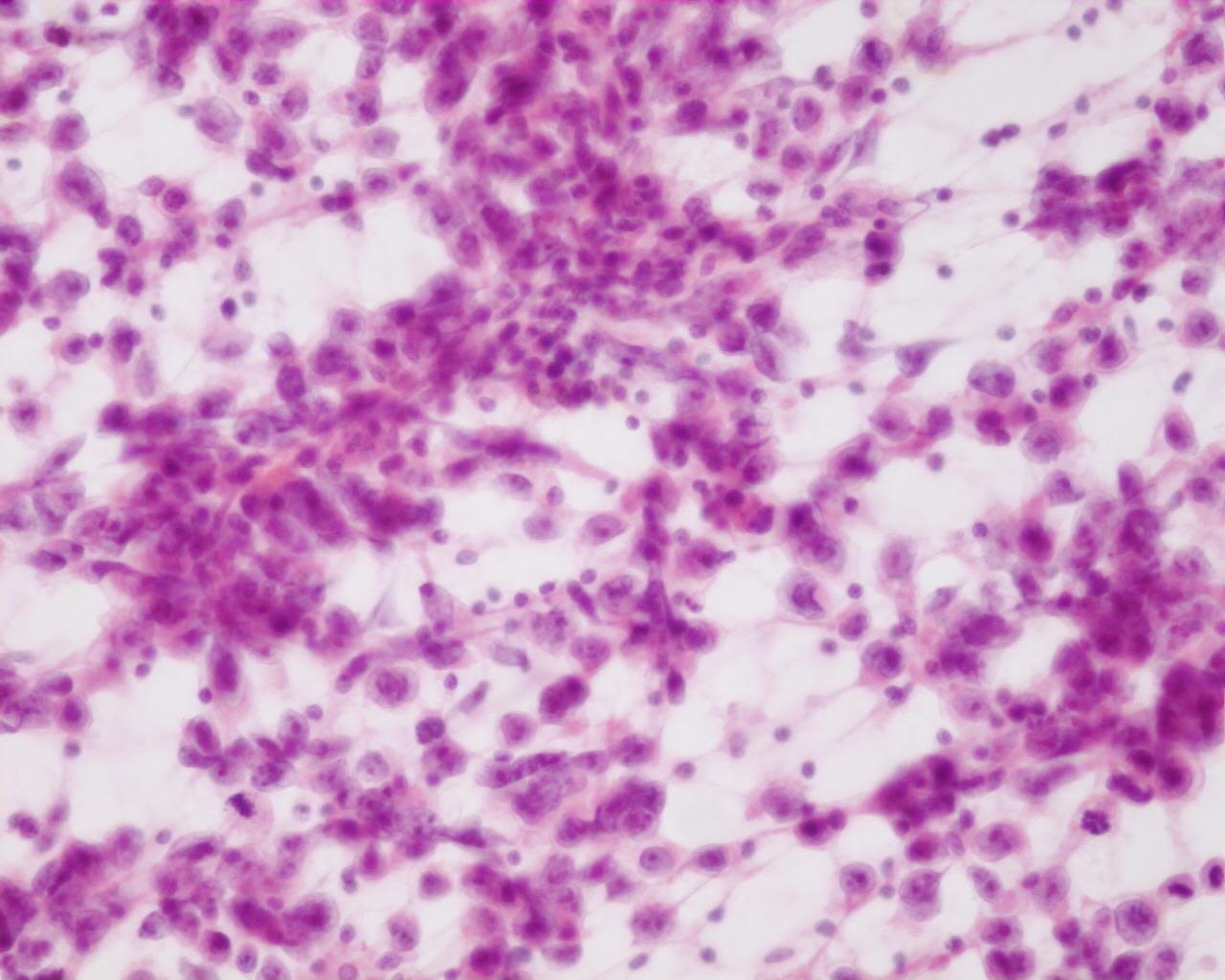
- Moderately to highly cellular smears
- Poorly cohesive cells
- Stripped nuclei
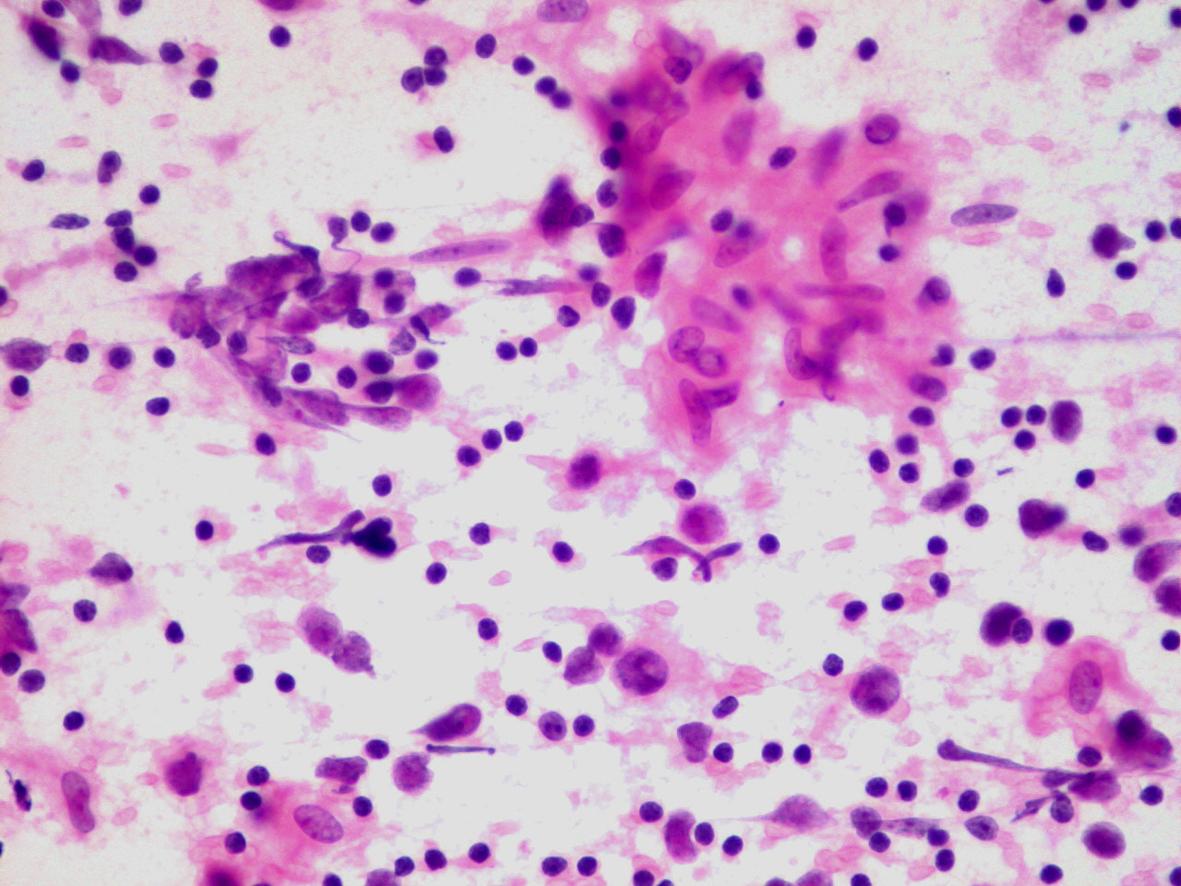
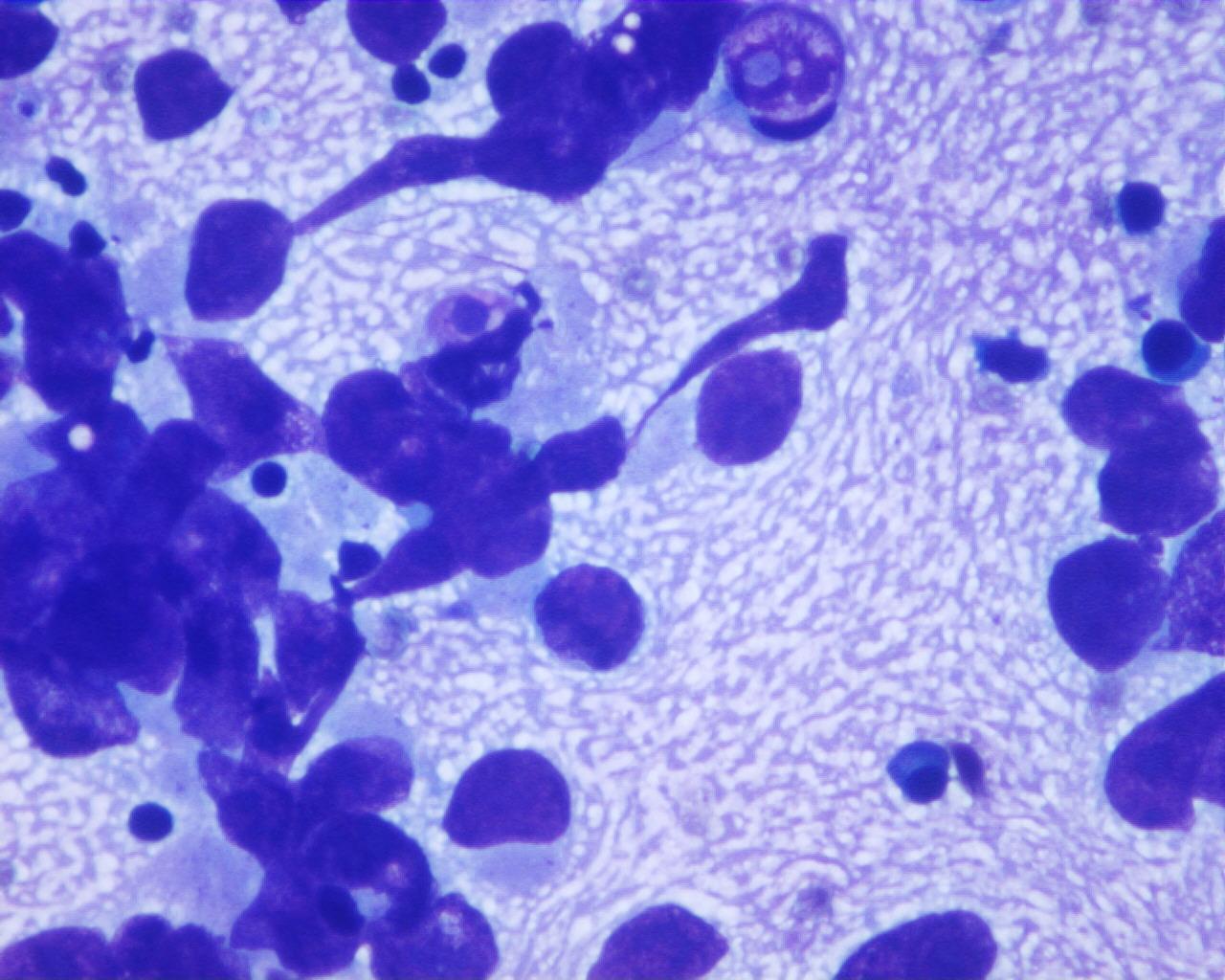
- Large single cells with single central vesicular nuclei and prominent nucleoli
- Fragile cytoplasm (glycogen)
- Tigroid background (Giemsa stain); absent in the atypical forms
- Epithelioid cells, occasionally granulomas
- Multinucleated histiocytic cells
- Lymphocytes (rare in the atypical forms)
- Necrosis is not characteristic
Histochemical stains
- PAS positive; PAS-diastase negative
Immunocytochemistry) (see Table 1)
- Placental alkaline phosphatase (PLAP): positive
- Vimentin: positive
- CD117: positive
- OCT4: positive
- Cytokeratin: generally negative (some authors have reported that 15% of cases are positive)
- EMA: negative
- Alpha-fetoprotein: negative
Differential diagnosis
- Large cell lymphoma
- Lymphoglandular bodies
- More irregular nuclei
- Lacks glycogen
- CD45: positive
- PLAP: negative
- Embryonal carcinoma
- Carcinoma pattern (acinar, tubular, papillary or solid)
- Prominent cellular polymorphism
- Nuclei with coarse chromatin and multiple nucleoli
- Necrosis
- Absence of lymphocytes
- Absence of tigroid background
- CD30: positive
- Cytokeratin: positive
- CD117: negative
Main points
- Five-year survival for pure forms is 80-90%
- Metastasizes to the opposite ovary, retroperitoneal nodes and peritoneal cavity
- Generally occurs as pure forms
- Association with choriocarcinoma, yolk sac tumour or embryonal carcinoma worsens the prognosis