Clinical features
- Mesenchymal neoplasm
- Low malignant potential
- Typically diagnosed in the first three months of life, and 90% diagnosed in the first year
- Diagnosis should not be done over three years of age
- Male predominance
- Represents 2 to 3% of paediatric renal tumours
- Represents 56% of renal tumours in the first three months of life
- Congenital (may be a cause of premature delivery, non-immune foetal hydrops and polyhydramnios)
- Low-risk tumours (SIOP-2001-revised working classification of renal tumours of childhood)
- Locally invasive.
- Most cases have an excellent prognosis ( 5% of relapses), most due to incomplete excisions
- Three morphologic subtypes can be characterized in histology: classical (22%), cellular (40-60%) and mixed (20%).
Fig1- Congenital Mesoblastic Nephroma- cohesive fragments o fibroblastic/myofibroblastic cells in a clear background (H&E)
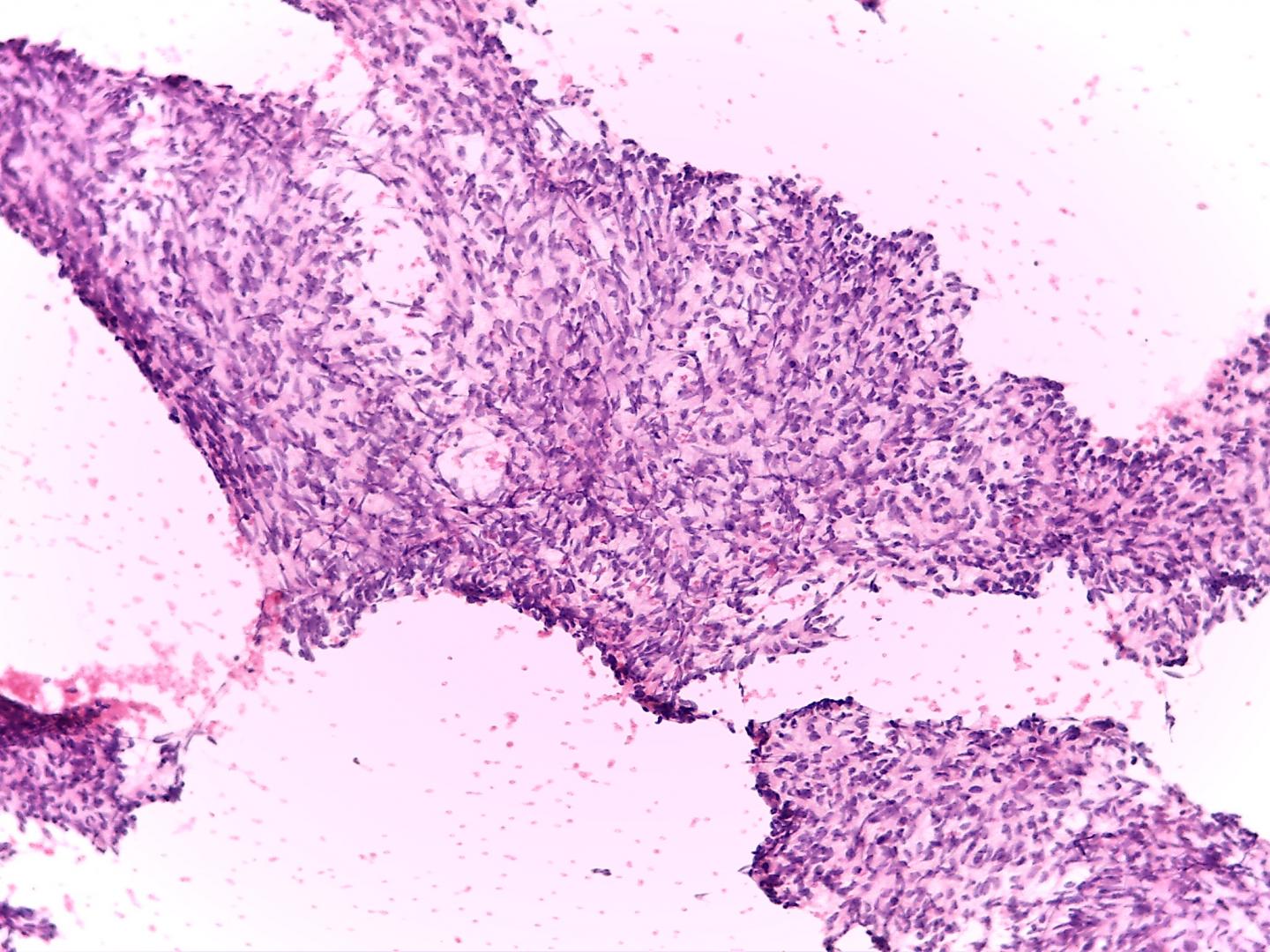
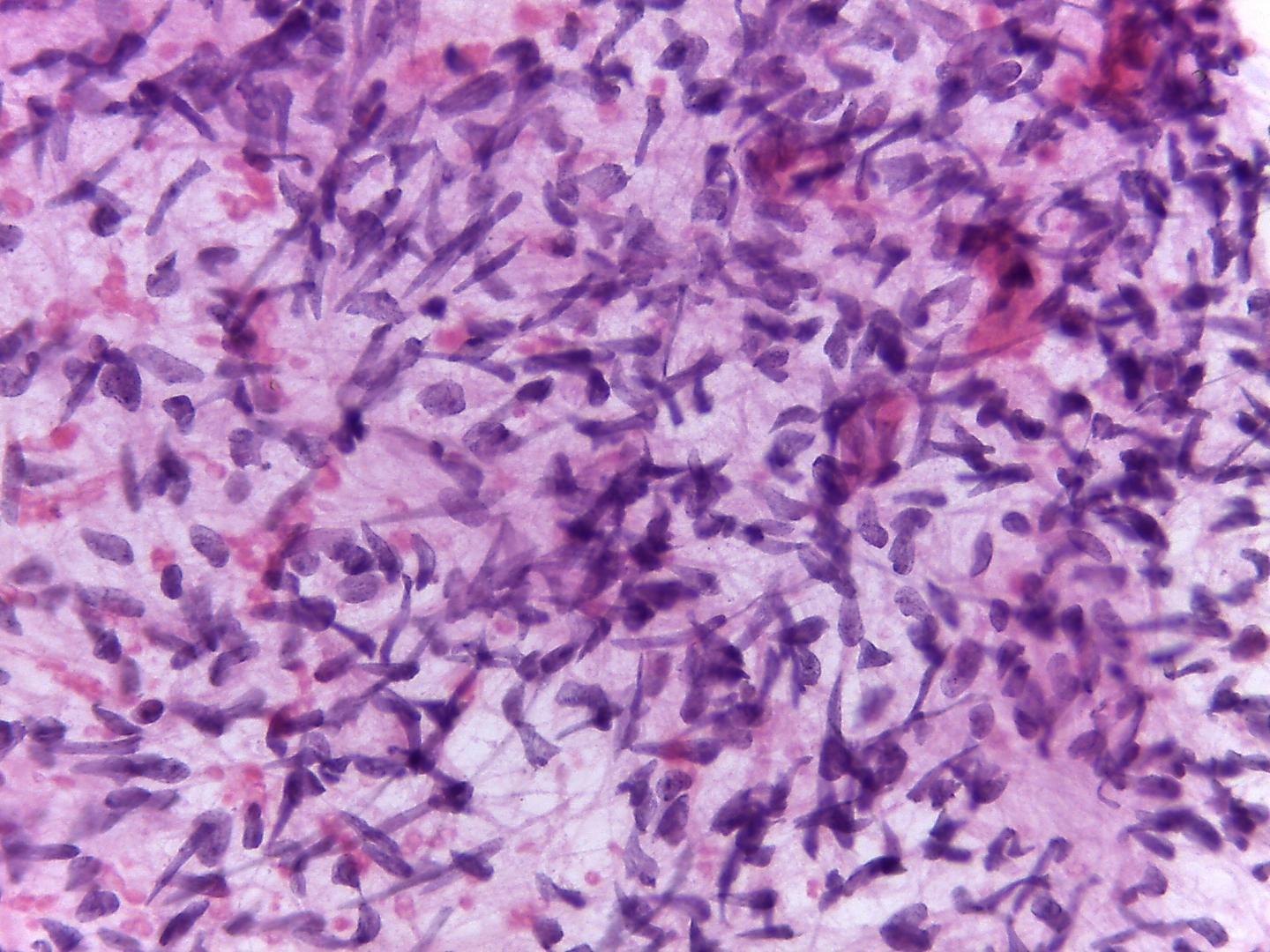
- Variable cellularity
- Naked nuclei and spindle/oval cells singly or in cohesive fragments-( Fig 1,Fig2)
- Fibroblastic/myofibroblastic bland nuclei
- Clear background; mucous-like material or necrosis in the background has been reported
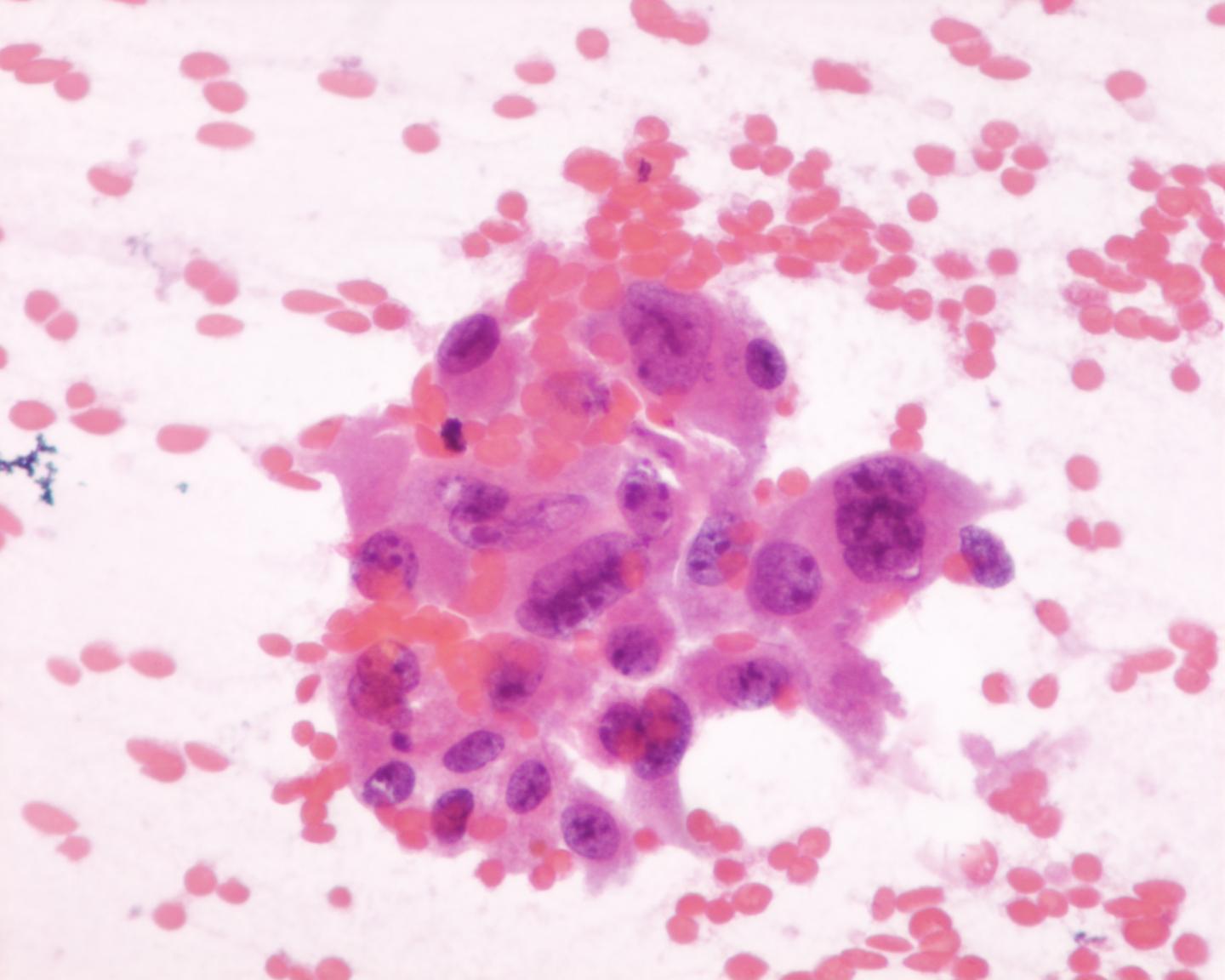
Attention is required regarding entrapped renal tubules of periphery, or even deeper situated in the tumour, which can acquire primitive appearance-(embryonal metaplasia-Fig 3). Entrapped tubules are EMA positive and CD56 (NCAM) negative. These antibodies are helpful in the distinction between mature and immature tubular epithelium from a Wilms´ tumour.
Immunocytochemistry
- Vimentin: positive
- Smooth muscle actin: positive
- WT1:Positive (only cytoplasm)
- Desmin: Positive
- CD56 (NCAM):Negative
- CD10: Negative
Genetic studies
- Polysomy of chromosomes 8,11,17 and 20 (only in the cellular variant)#
- t (12; 15)(p13;q26)- ETV6/NTRK3 fusion gene (only in the cellular variant)#
- Trisomy 11 –related to progression of classic to cellular type
These aspects are shared with infantile fibrosarcoma
Differential diagnosis
- Stromal: predominantly Wilms’ tumour
- Wilms´ pure morphologic cases are rare; multiple samples can solve the problem
- Clear cell sarcoma
- Background with metachromatic mucoid-like material rich in glycoproteins, seen in Giemsa-stained slides
- Nuclei with vesicular chromatin
- Nuclear grooves
- CD56 (NCAM): positive
- WT1: Negative
- Rhabdoid tumour of the kidney
- Pale nuclei
- Nucleoli are more prominent
- Eosinophilic para nuclear cytoplasmic inclusions
- Cytokeratin: positive (dot)
- WT1: Negative
- INI1 : loss of expression
Main points
- Low-grade fibroblastic sarcoma of the kidney
- Genetic studies have concluded that mesoblastic nephroma of classic and cellular types are different entities. Molecular similarities between the cellular type of mesoblastic nephroma and infantile fibrosarcoma have led to the belief that these two entities are the same, in different locations. Both share the same chromosome translocation t(12;15)(p13,q25)
- Rare cases of local recurrence are generally due to incomplete excision
- Generally cured by surgical excision
- Excellent prognosis (95% of cases do not relapse)