This content is also available in:
![]() English
English ![]() Español
Español ![]() Magyar
Magyar ![]() Polski
Polski
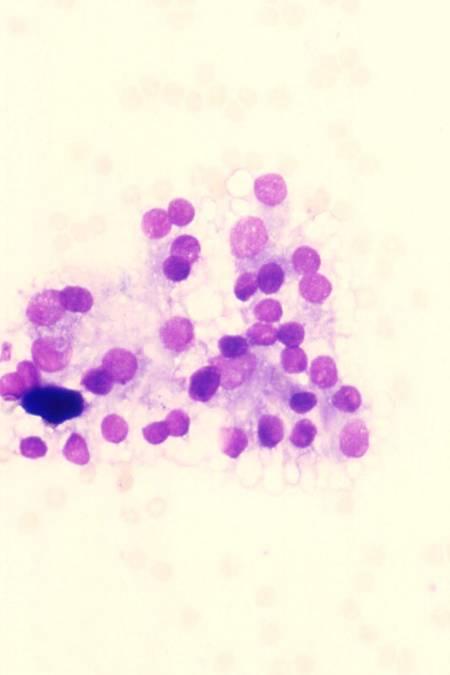
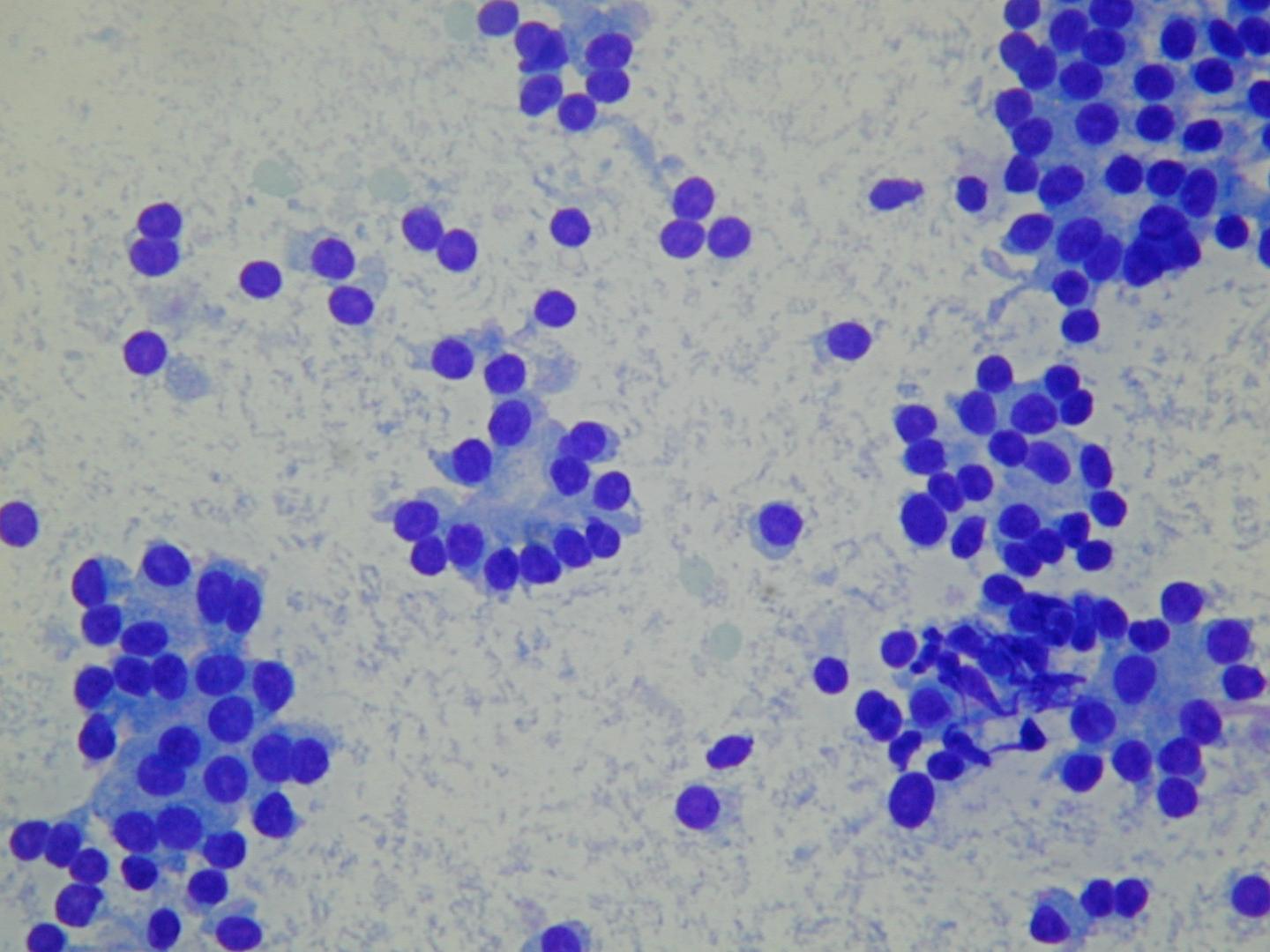
Cytologické diagnostické znaky
- nízká nebo st?ední bun??nost
- kohezivní bu?ky
- p?evážn? mikrofolikulární úprava
- uniformní, pravideln? uložené folikulární bu?ky
- okrouhlá jádra, jemn? granulární chromatin
- chudá nebo st?ední cytoplazma
- málo makrofág?
- nahá jádra
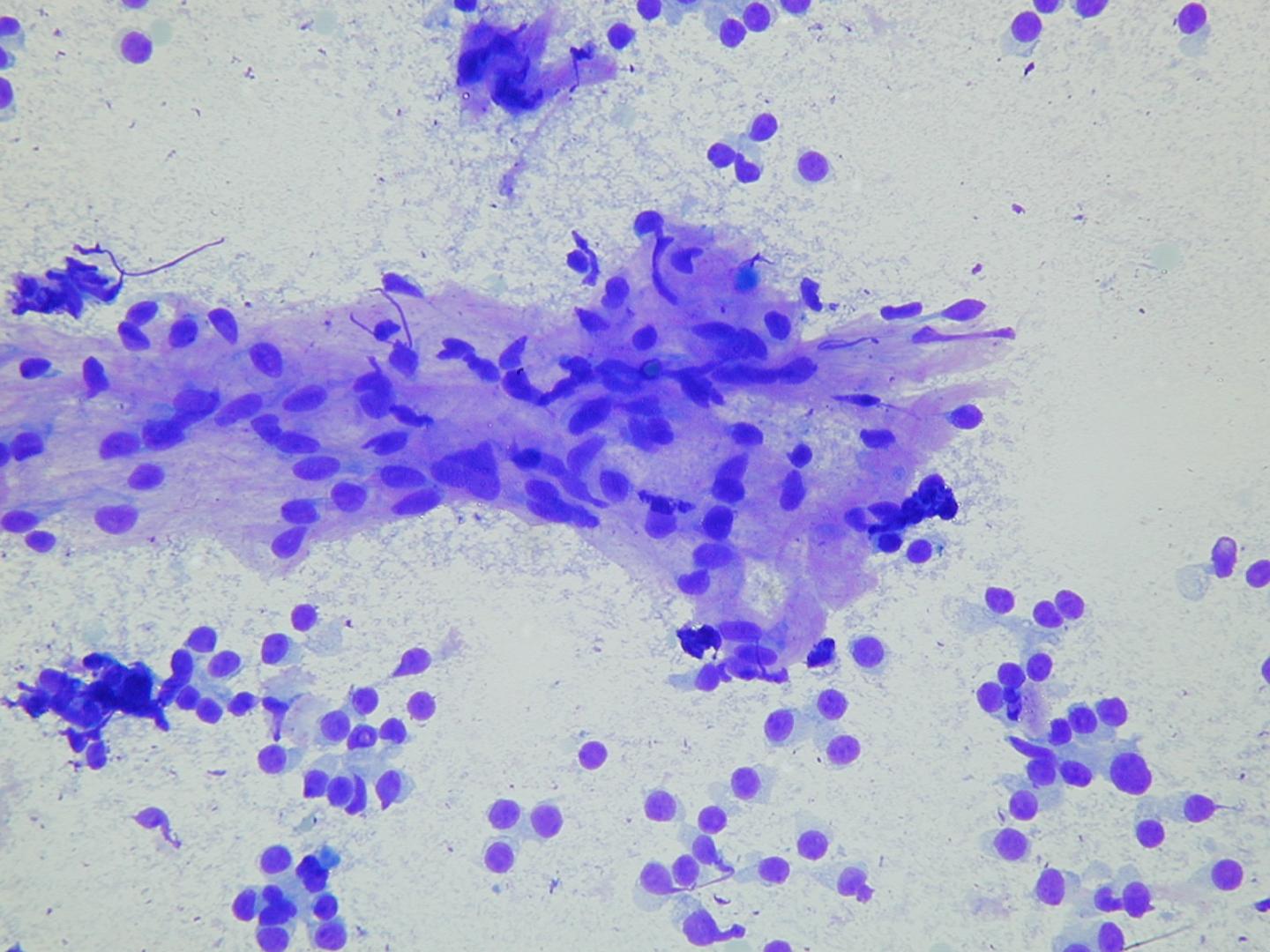
Koloid je obvykle hojný v podob? amorfních kapek nebo jako tenký pr?svitný film s bublinami a lineárními trhlinami.
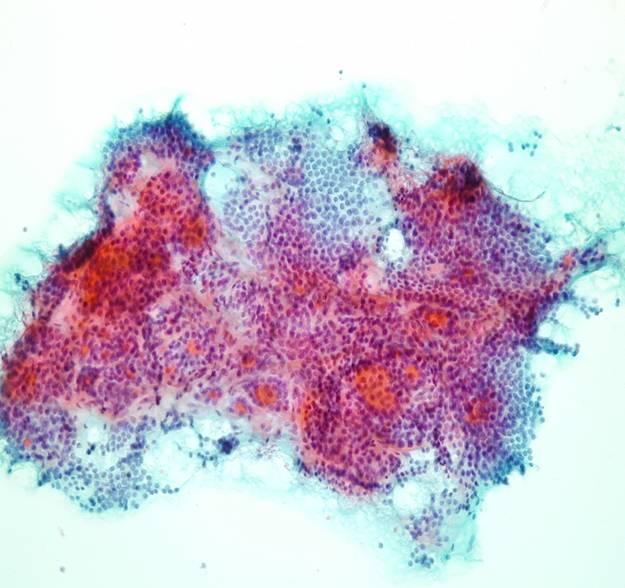
N?které benigní folikulární léze jsou hypercelulární a mohou dokonce obsahovat fokální cytologické atypie. P?íležitostné se mohou objevit velké v?etenité bu?ky reprezentující bu? reaktivní stromální elementy nebo zm?n?né folikulární bu?ky vystýlající cystické dutiny. Fokální onkocytární transformace (Hürthleho bu?ky) se rovn?ž mohou objevit. Pokud je mikrofolikl? málo a atypie je fokální , m?la by diagnóza být benigní folikulární uzel i když je zrovna bun??nost vzorku vyšší.
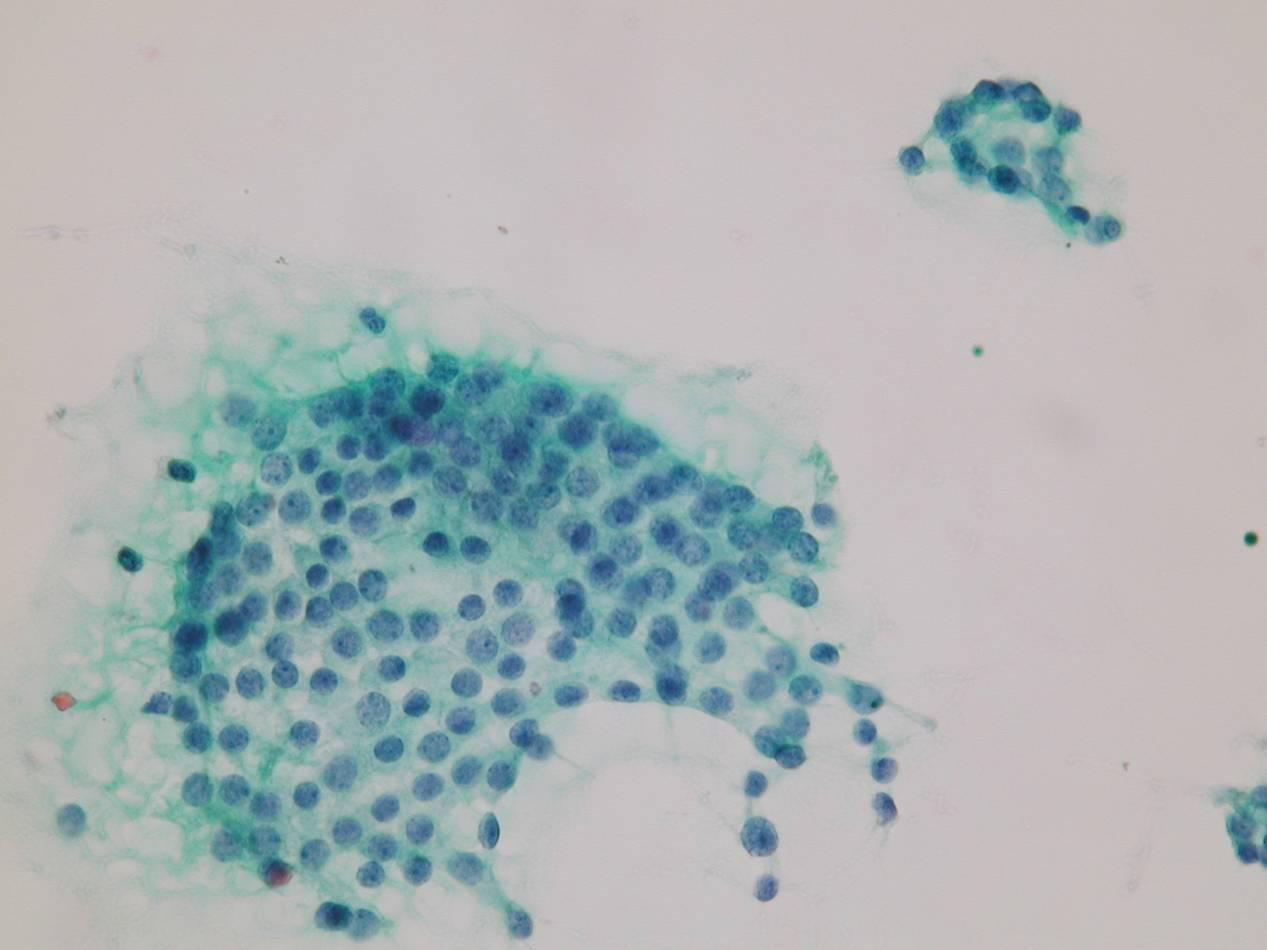
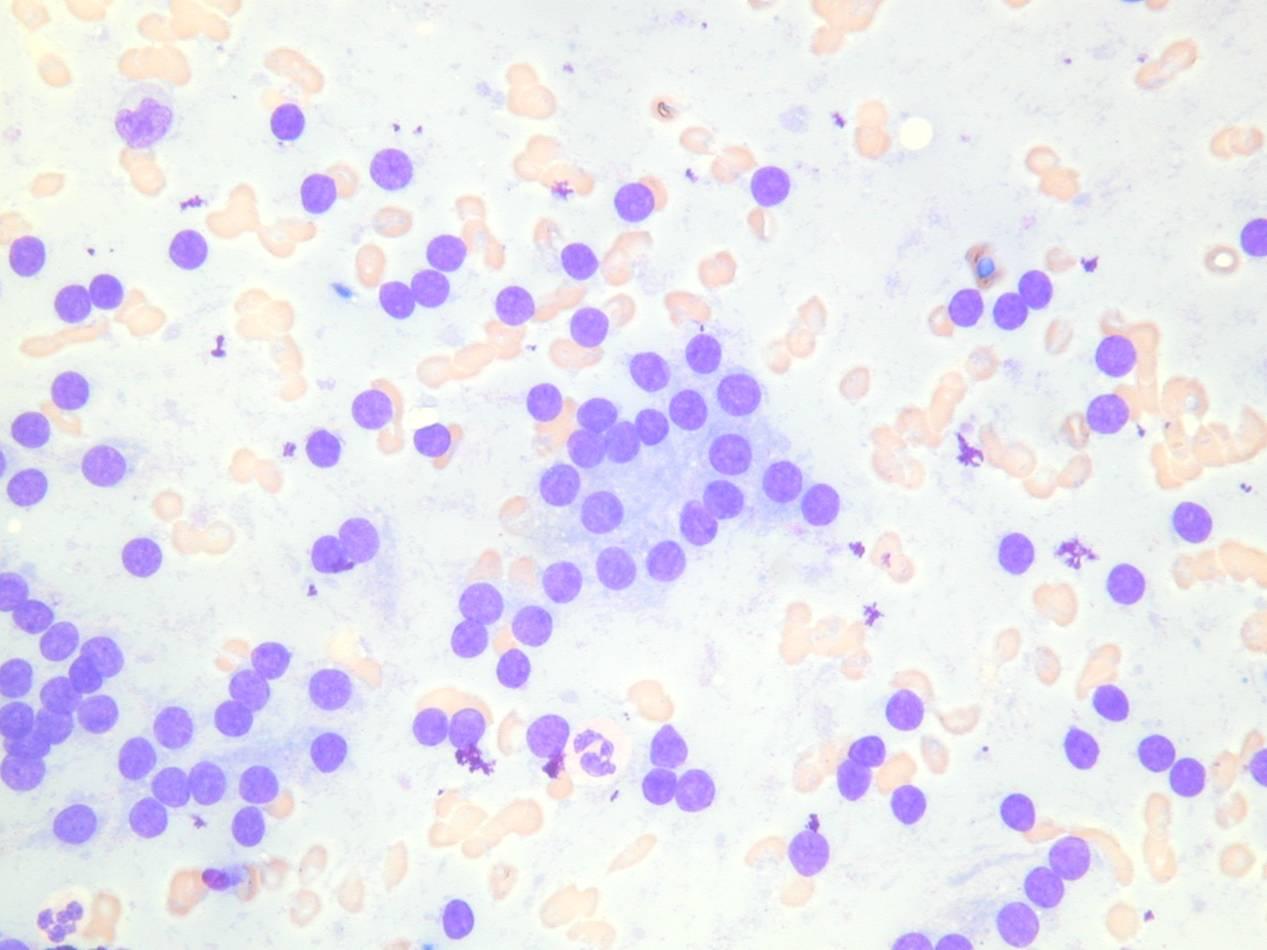
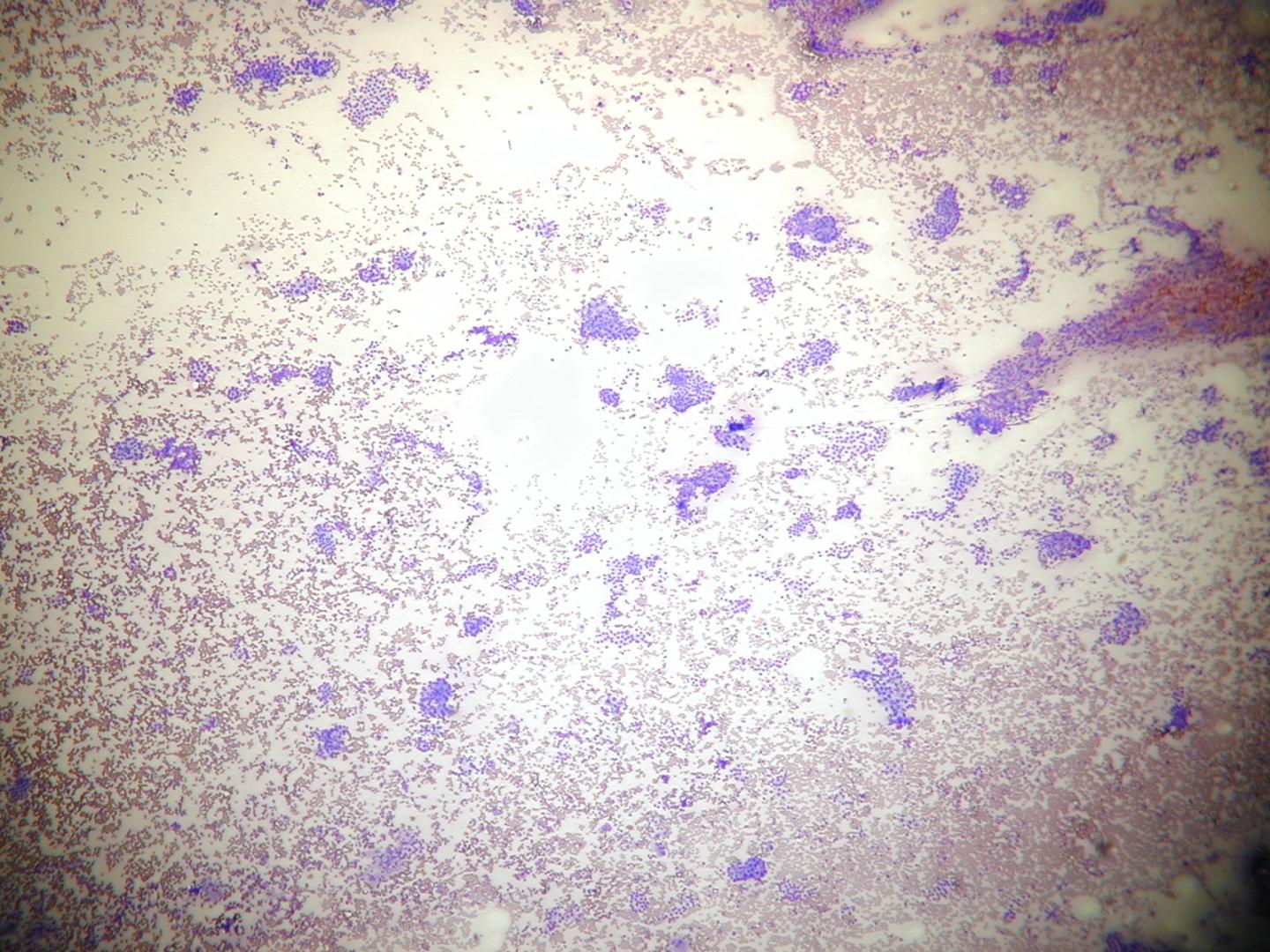
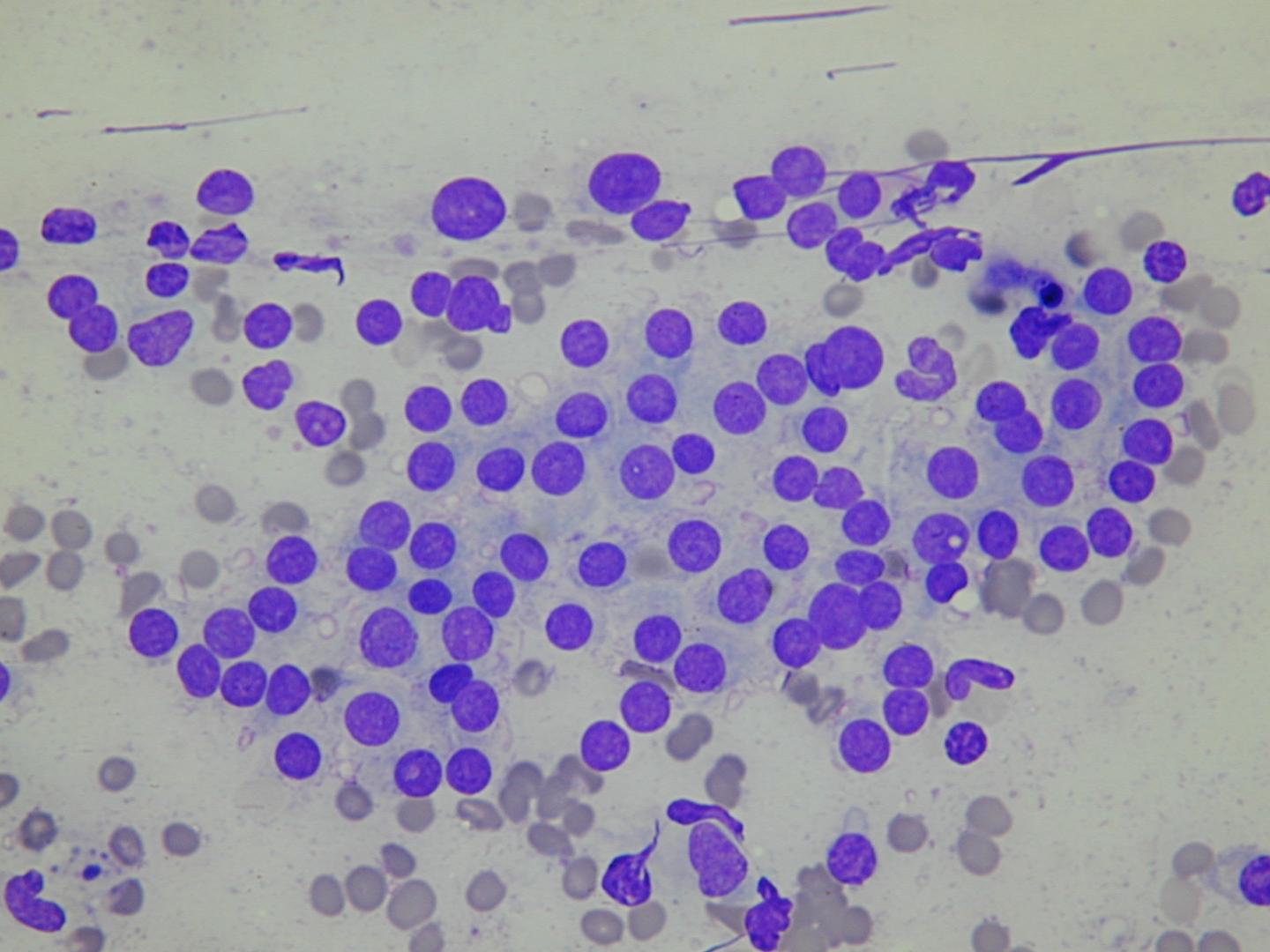
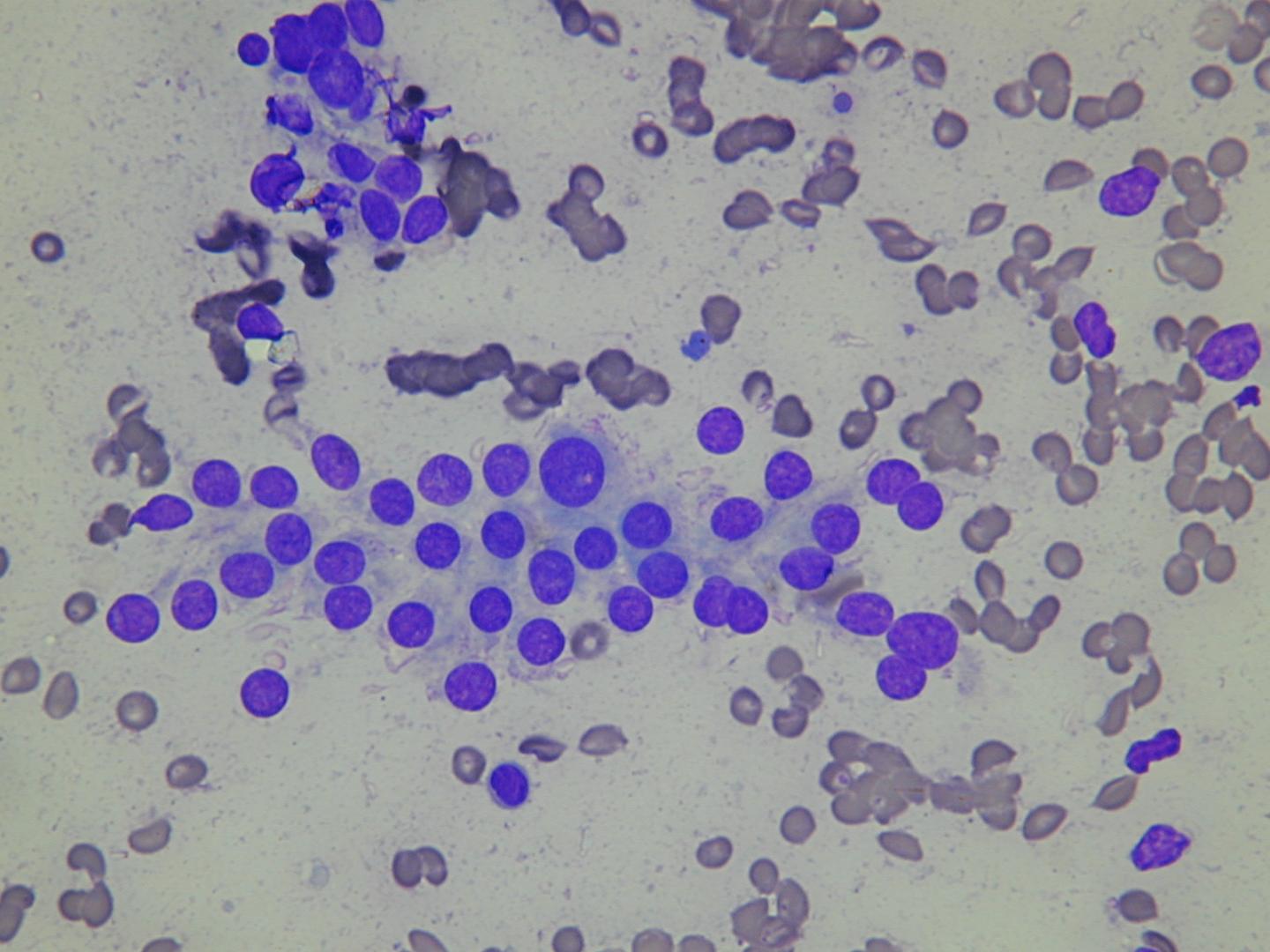
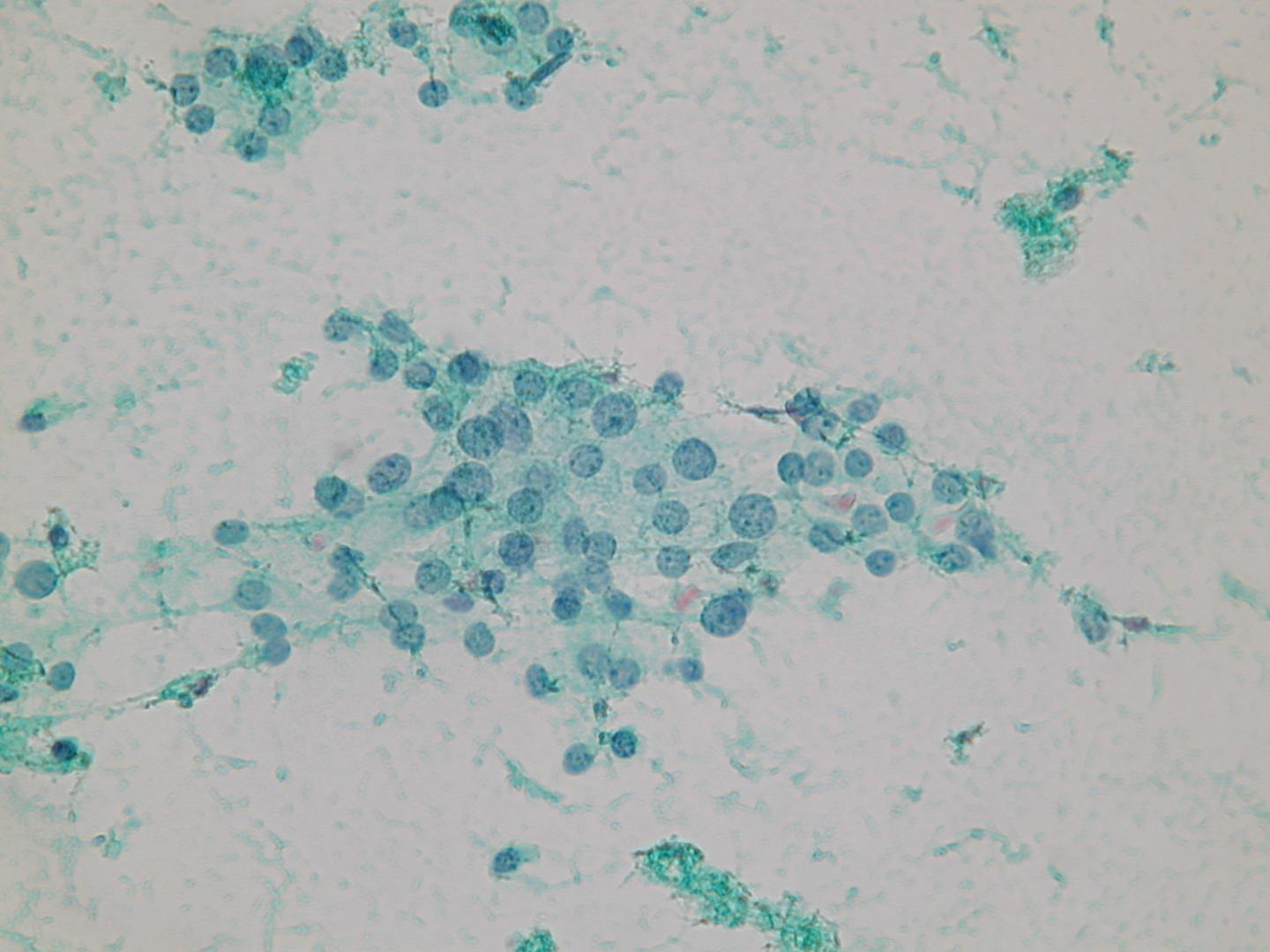
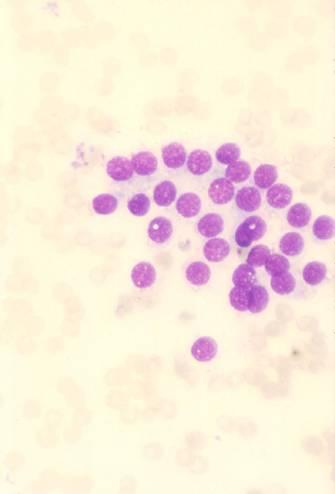
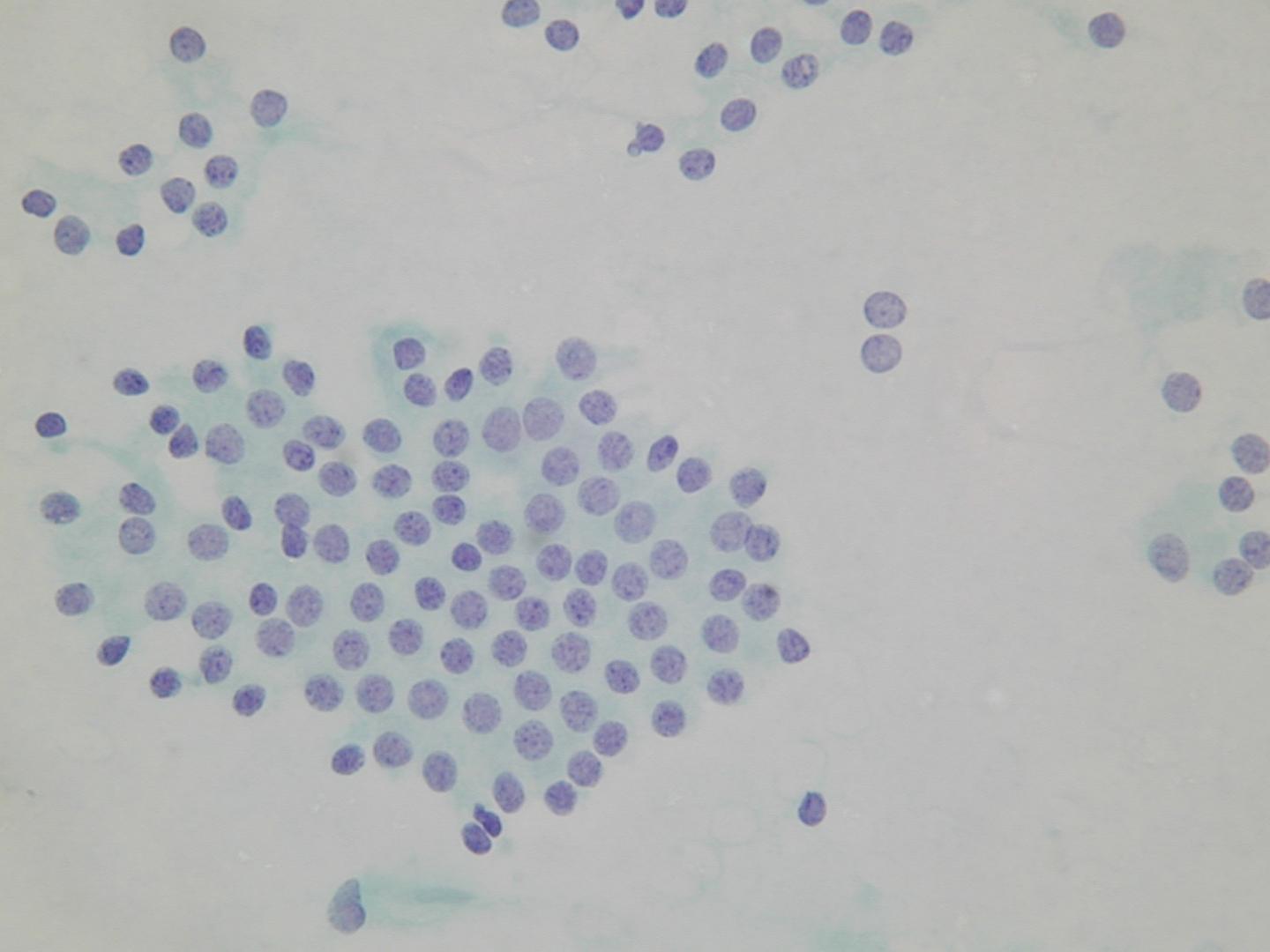
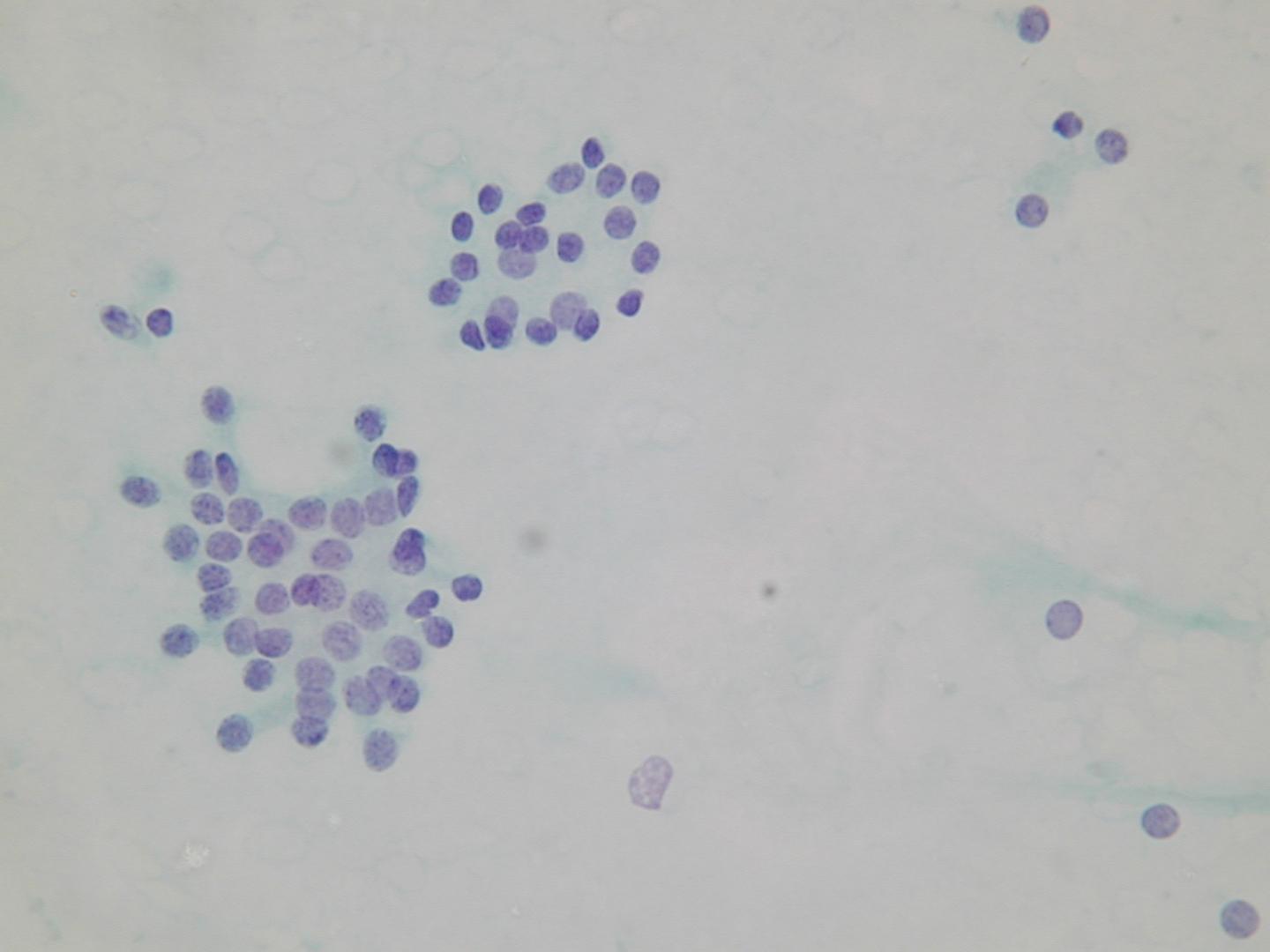
A microfollicular pattern:
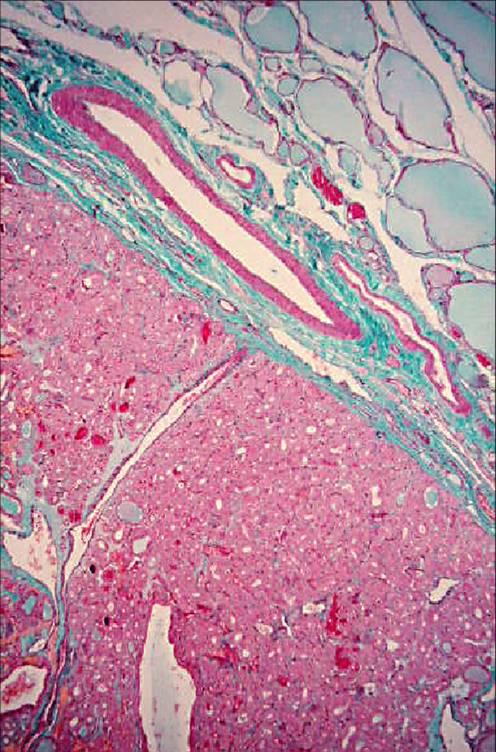
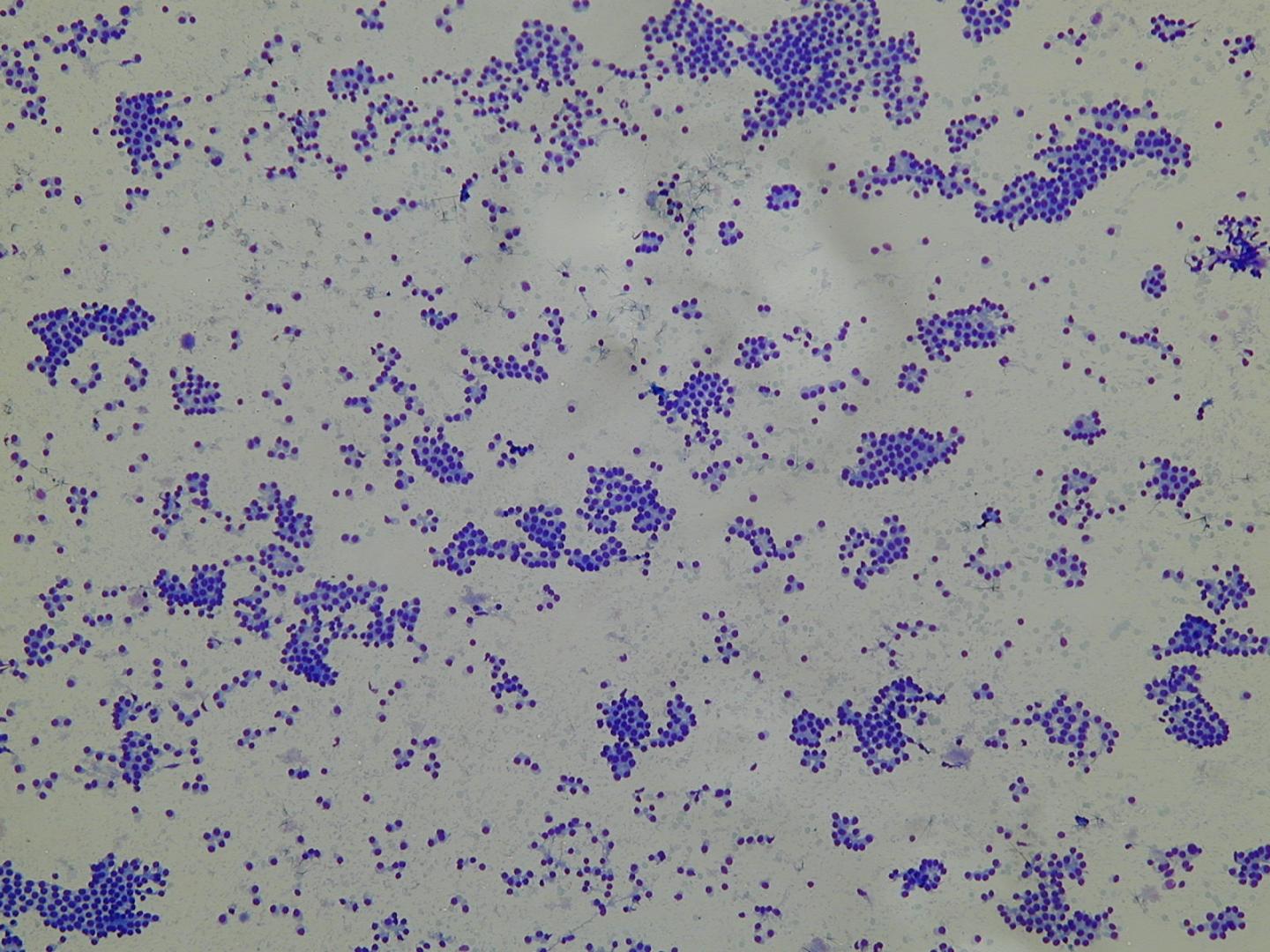
Folikulární adenom
Folikulární adenom je benigní nádor- obvykle solitární uzel do pr?m?ru 3cm. N?které mohou produkovat thyroidální hormony a vyvolat hyperthyroidismus (funk?ní – horké adenomy). Histologický obraz je variabilní: makrofolikulární (sestává z velkých folikl? vypln?ných koloidem), mikrofolikulární (s malými folikuly), trabekulární s folikulárními bu?kami upravenými do pruh?).
Klasificace (nemá prognostický význam)
- prostý
- mikrofolikulární
- trabekularární
- oxyfilní
- atypický
- papilární
- z prsténcových bun?k
| Nodular hyperplasia | Follicular neoplasia |
|---|---|
| multiple | solitary |
| poorly encapsulated | encapsulated |
| architectural heterogeneity | uniformity of the architecture |
| cytologic heterogeneity | cytologic homogeneity |
| comparable areas in adjacent gland | different from surrounding gland |
| no compression of surrounding gland | compression of surrounding gland |
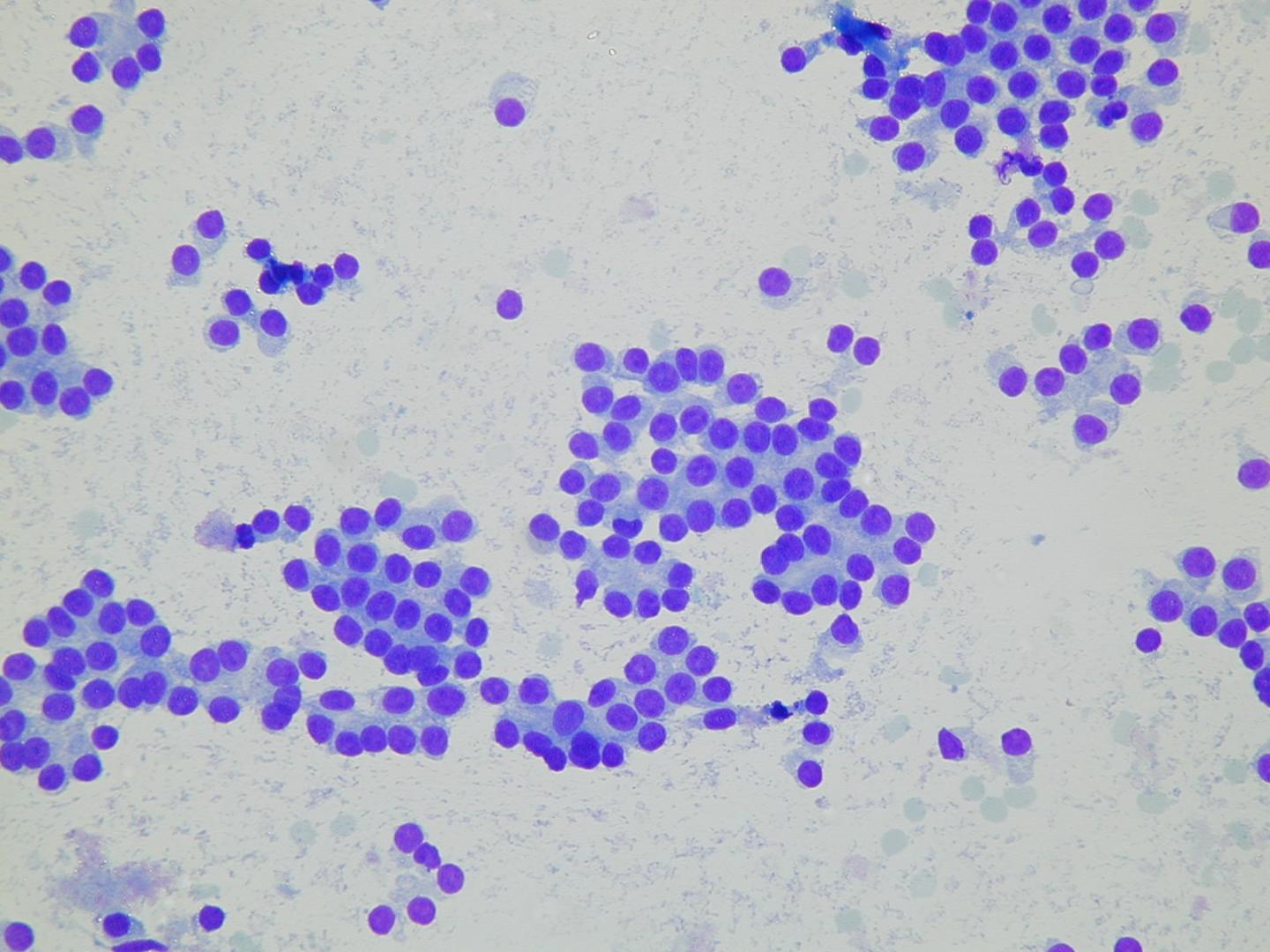
Microfollicular groups: