This content is also available in:
![]() English
English ![]() Čeština
Čeština ![]() Magyar
Magyar ![]() Polski
Polski
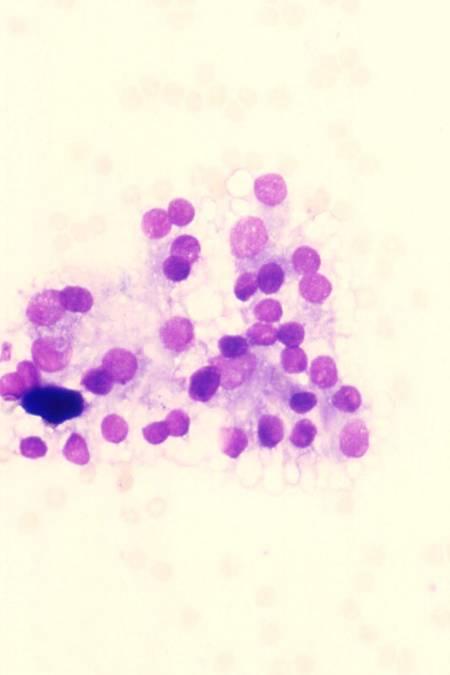
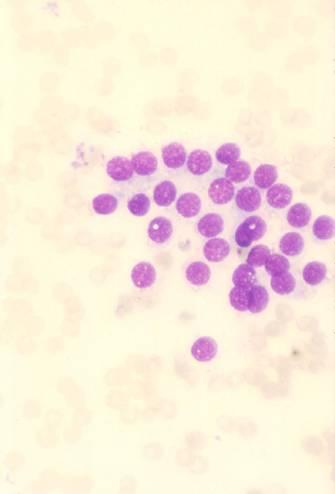
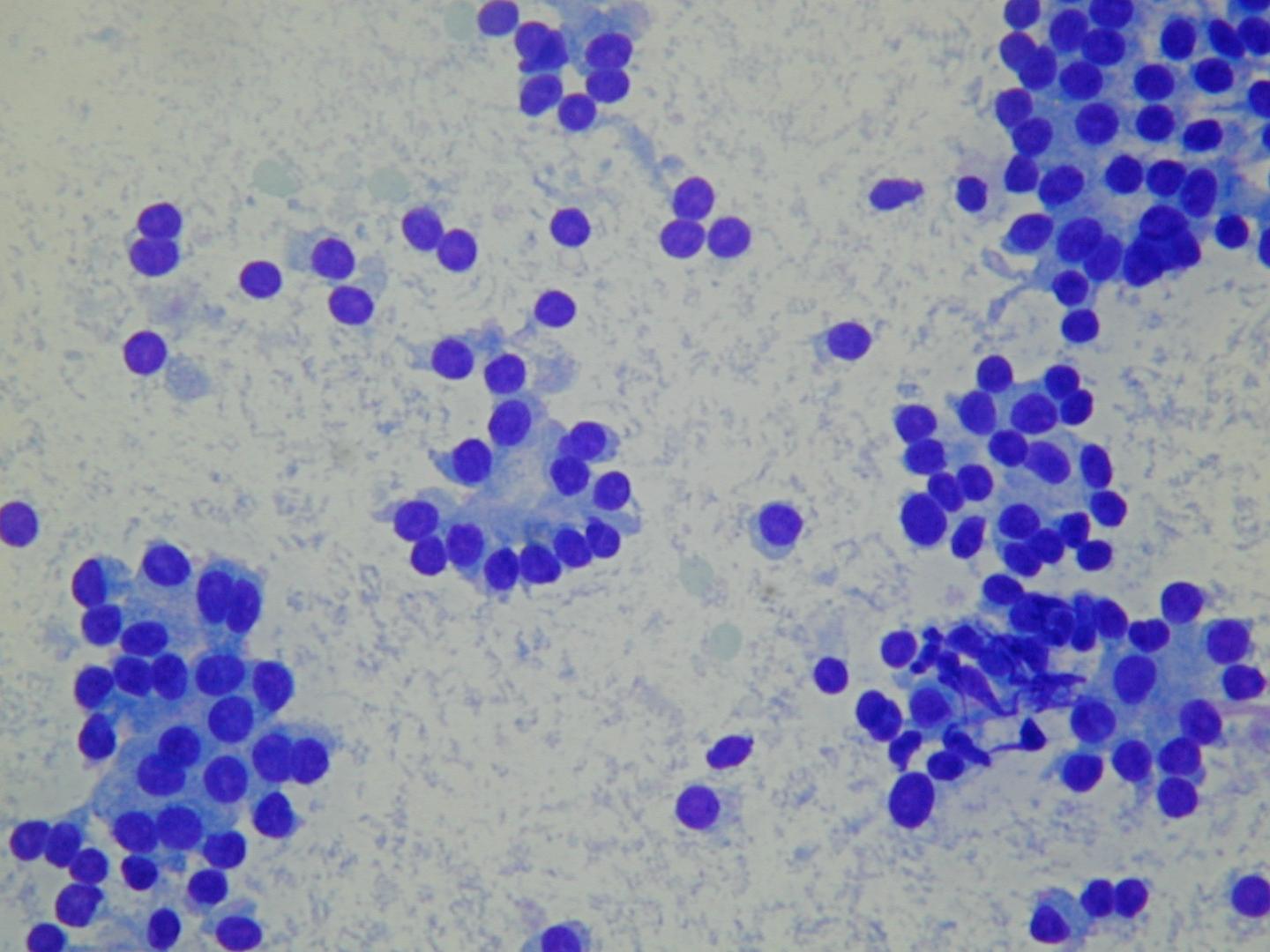
Características citológicas diagnósticas
- Baja o moderada celularidad
- Células cohesivas
- Patrón de predominio microfolicular
- Células foliculares uniformes, regularmente espaciadas.
- Núcleos redondos, cromatina finamente granular
- Citoplasma escaso o moderado
- Algunos macrófagos
- Núcleos desnudos
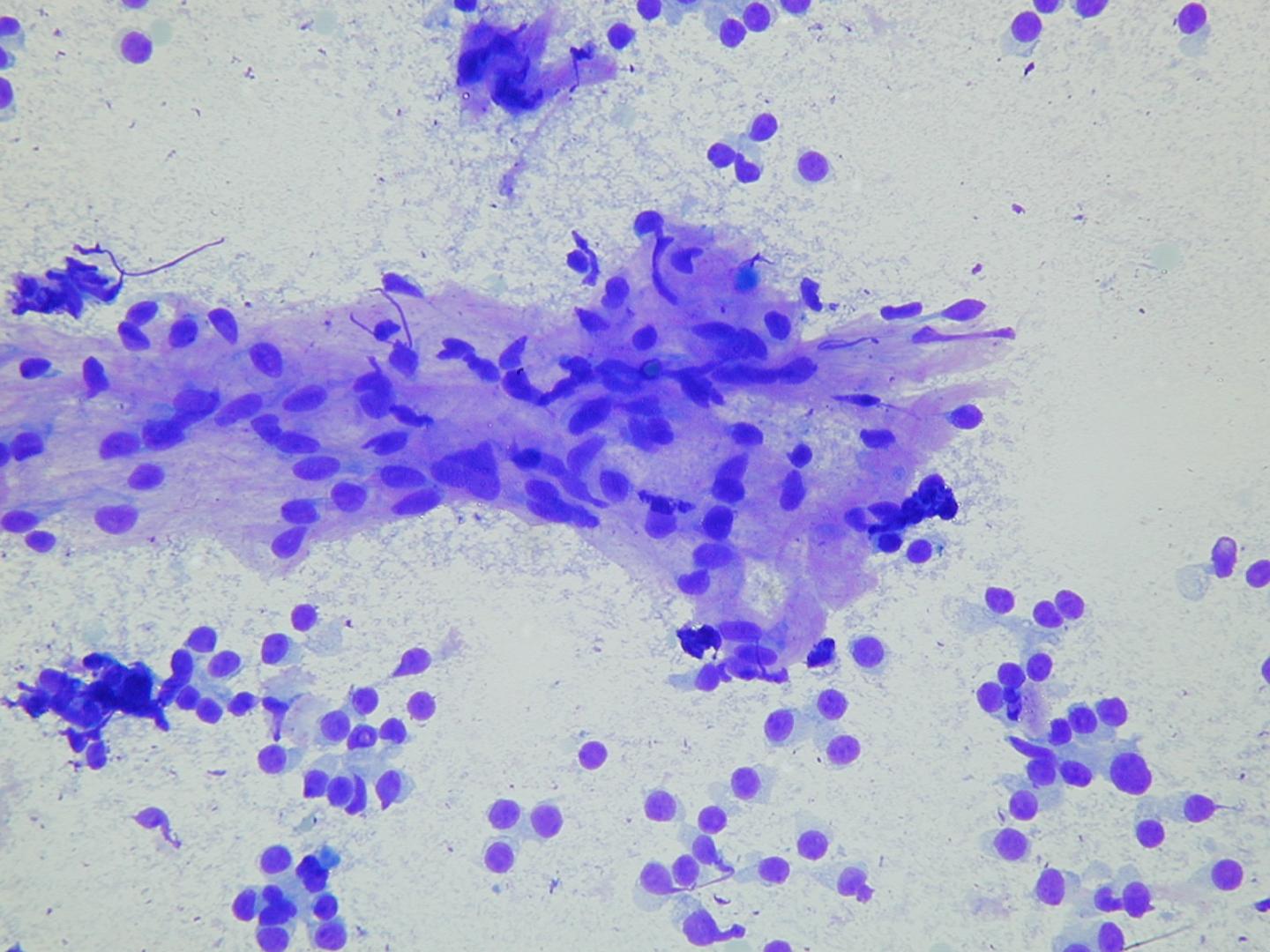
El coloide es usualmente abundante, aparece como gotas amorfas o como una película delgada translúcida con burbujas y fisuras lineares.
Algunas lesiones foliculares benignas son hipercelulares y pueden presentar atipia citológica focal. Pueden encontrarse ocasionales células alargadas, en forma de huso, representando elementos del estroma reactivo o células foliculares alteradas recubriendo áreas de degeneración quística. También pueden ocurrir cambios de células de Hurtle focales. Si los microfolículos son escasos y la atipia es focal, se debe realizar un diagnóstico de un nódulo benigno citológicamente, aun si la muestra es celular. Los pacientes con este diagnóstico tienen que tener un seguimiento a intervalos apropiados.
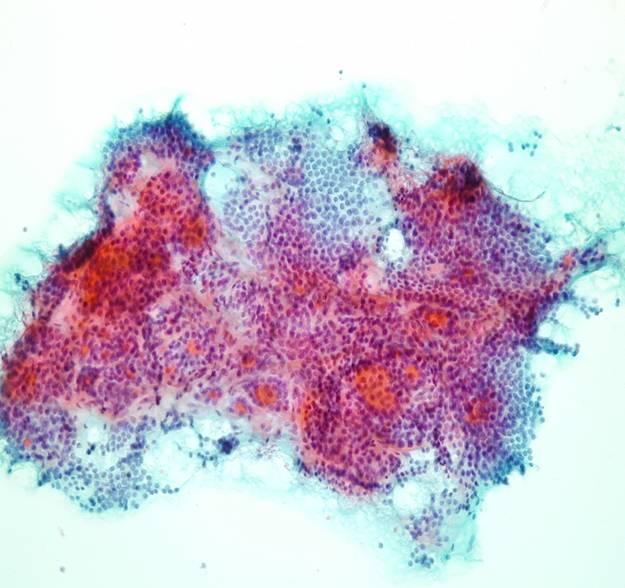
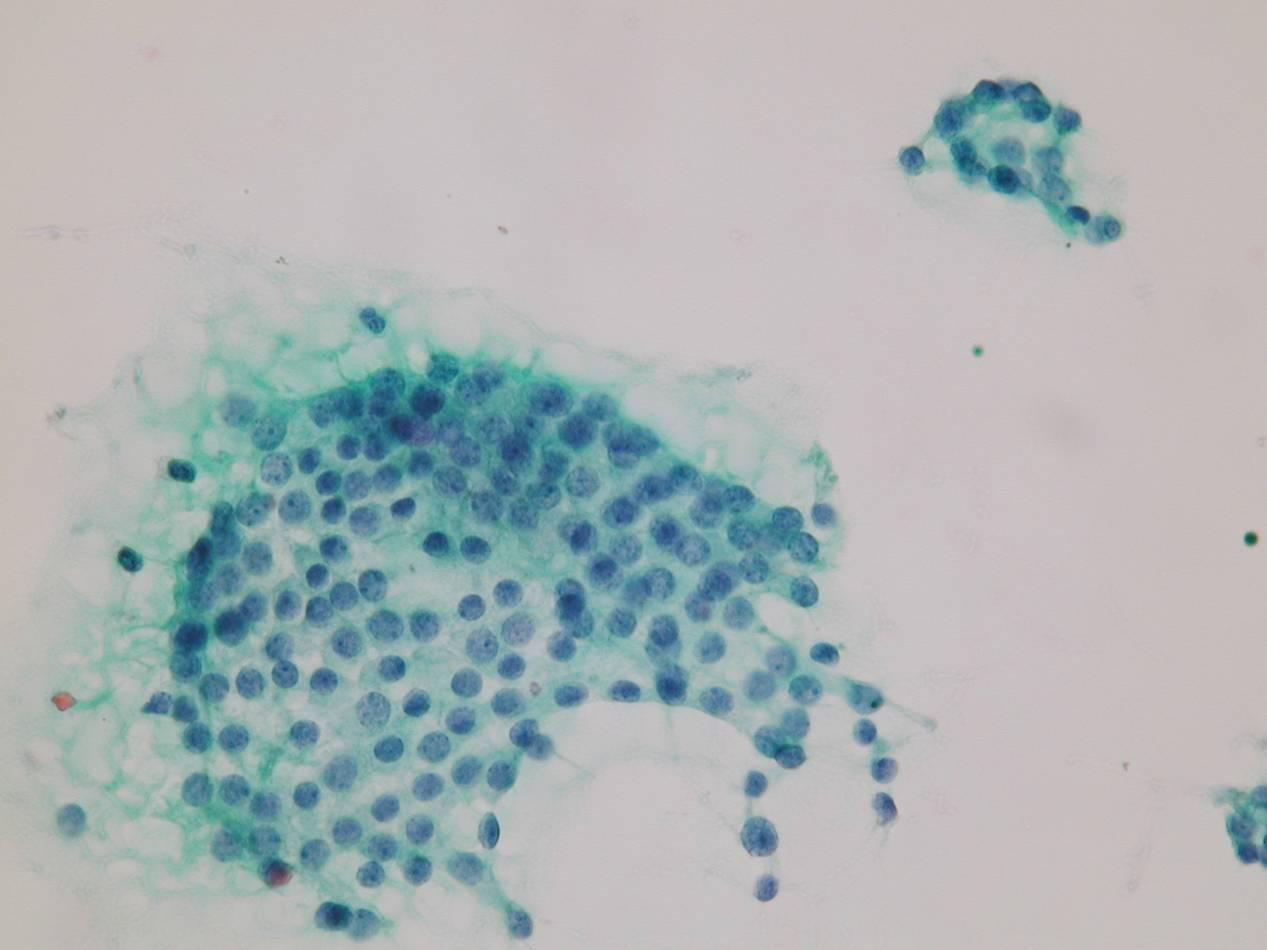
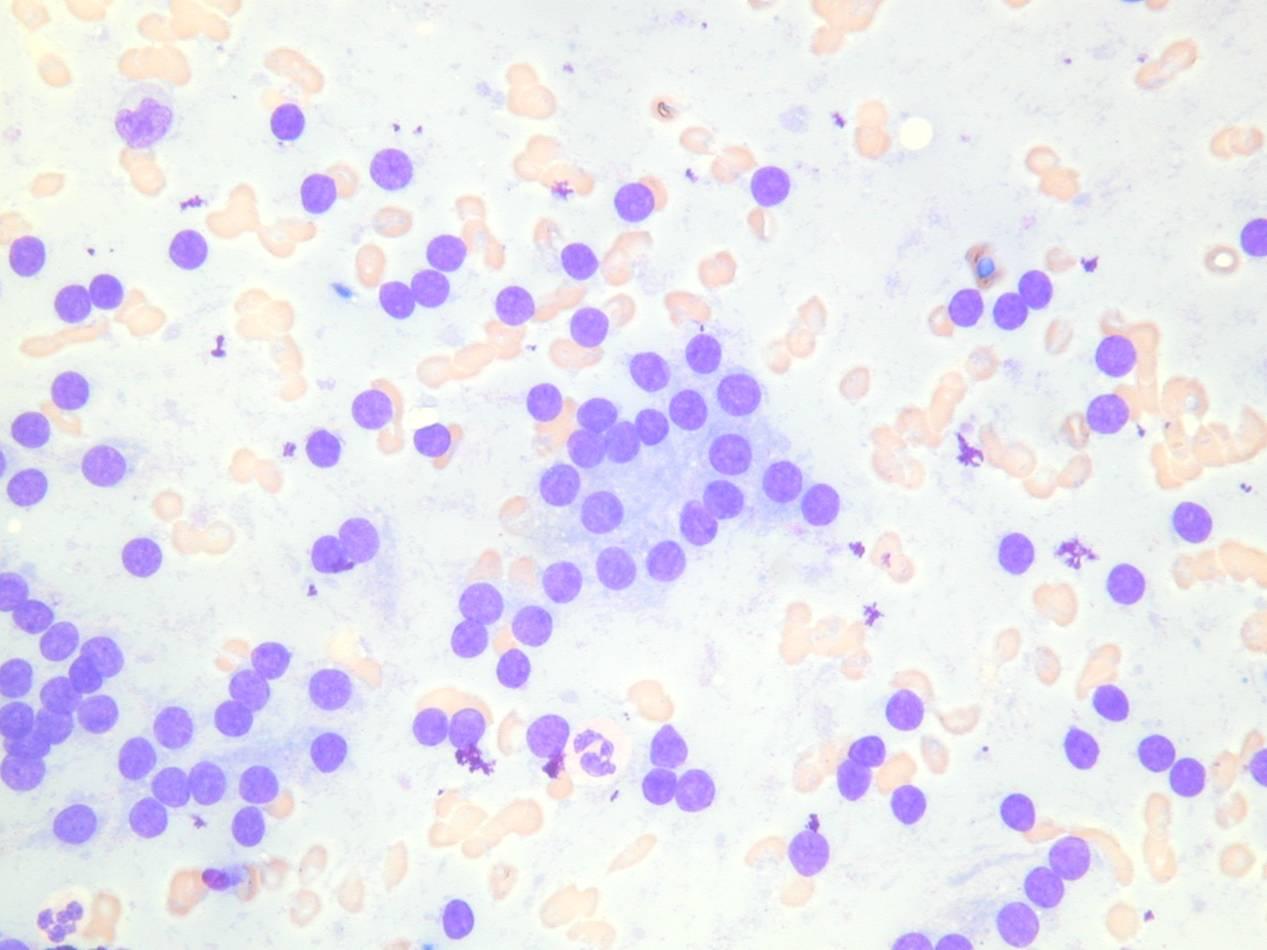
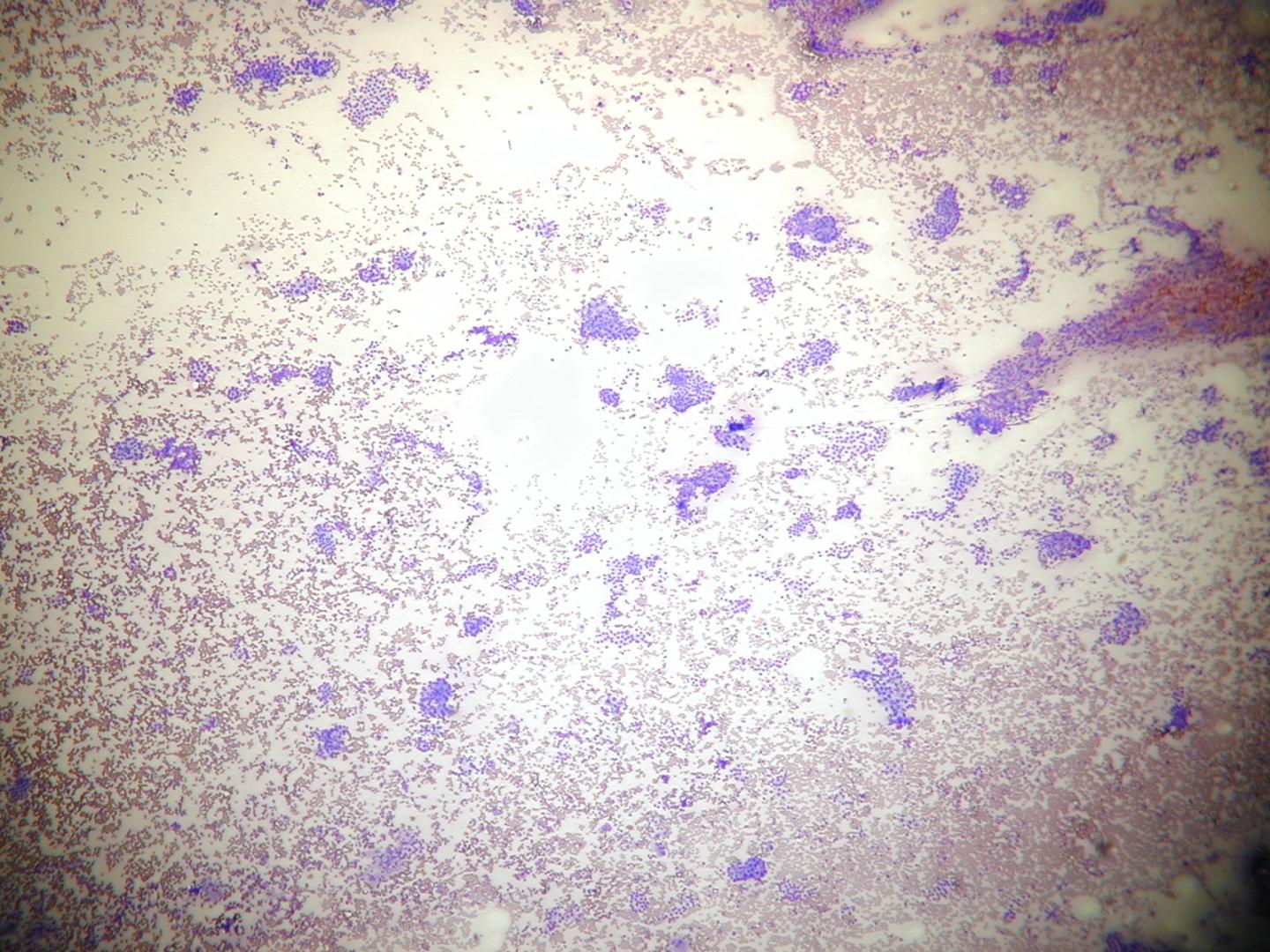
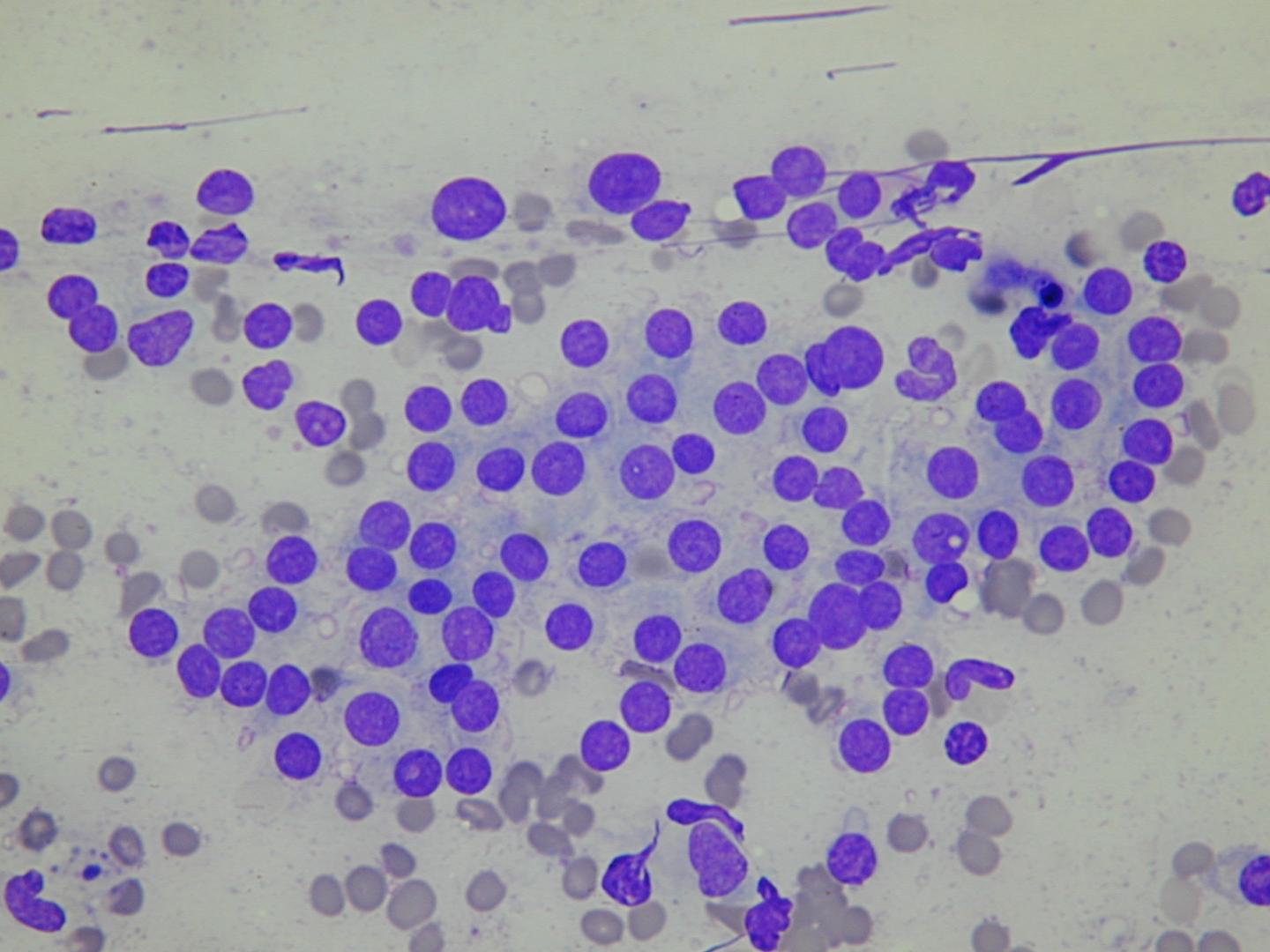
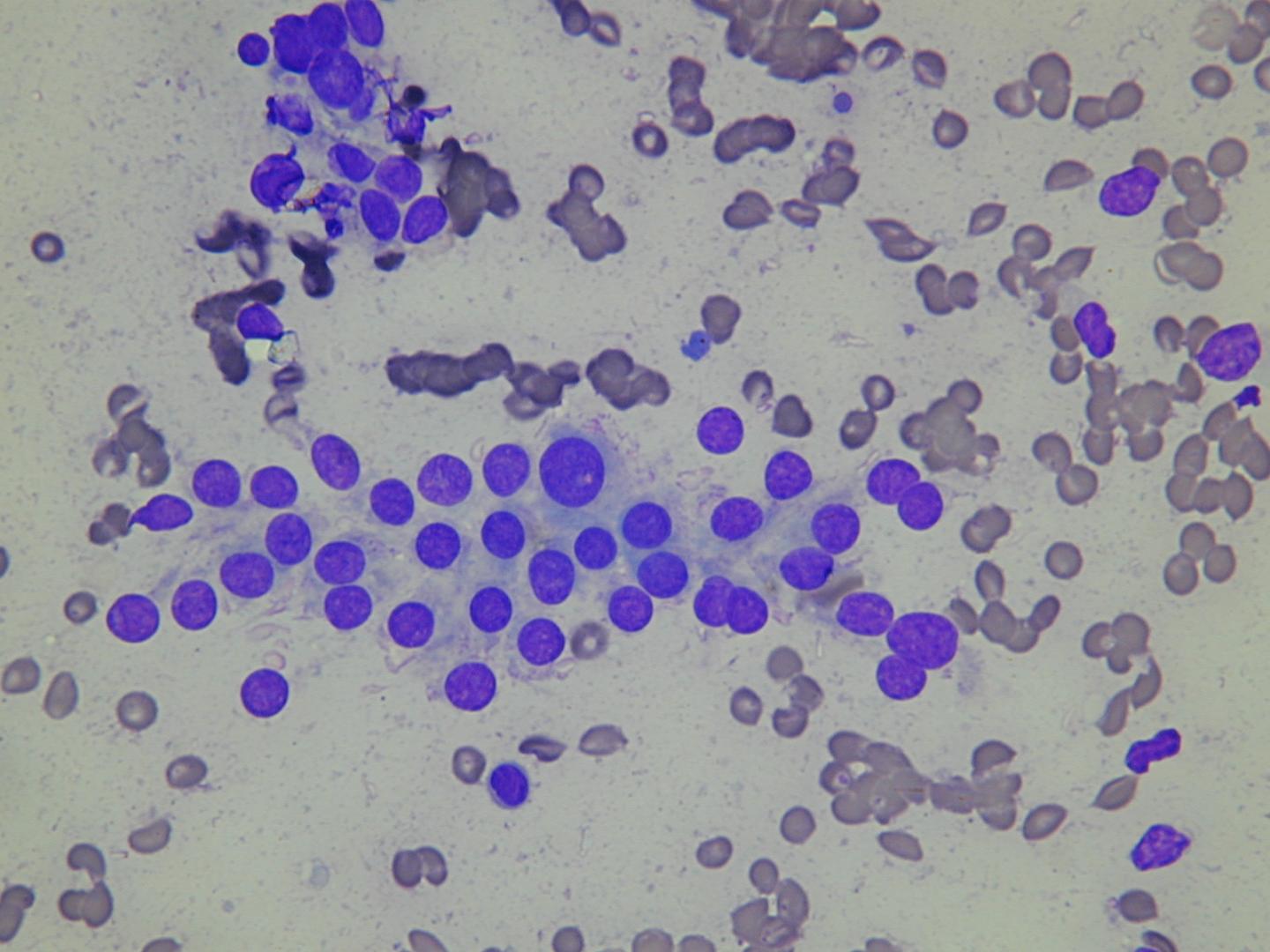
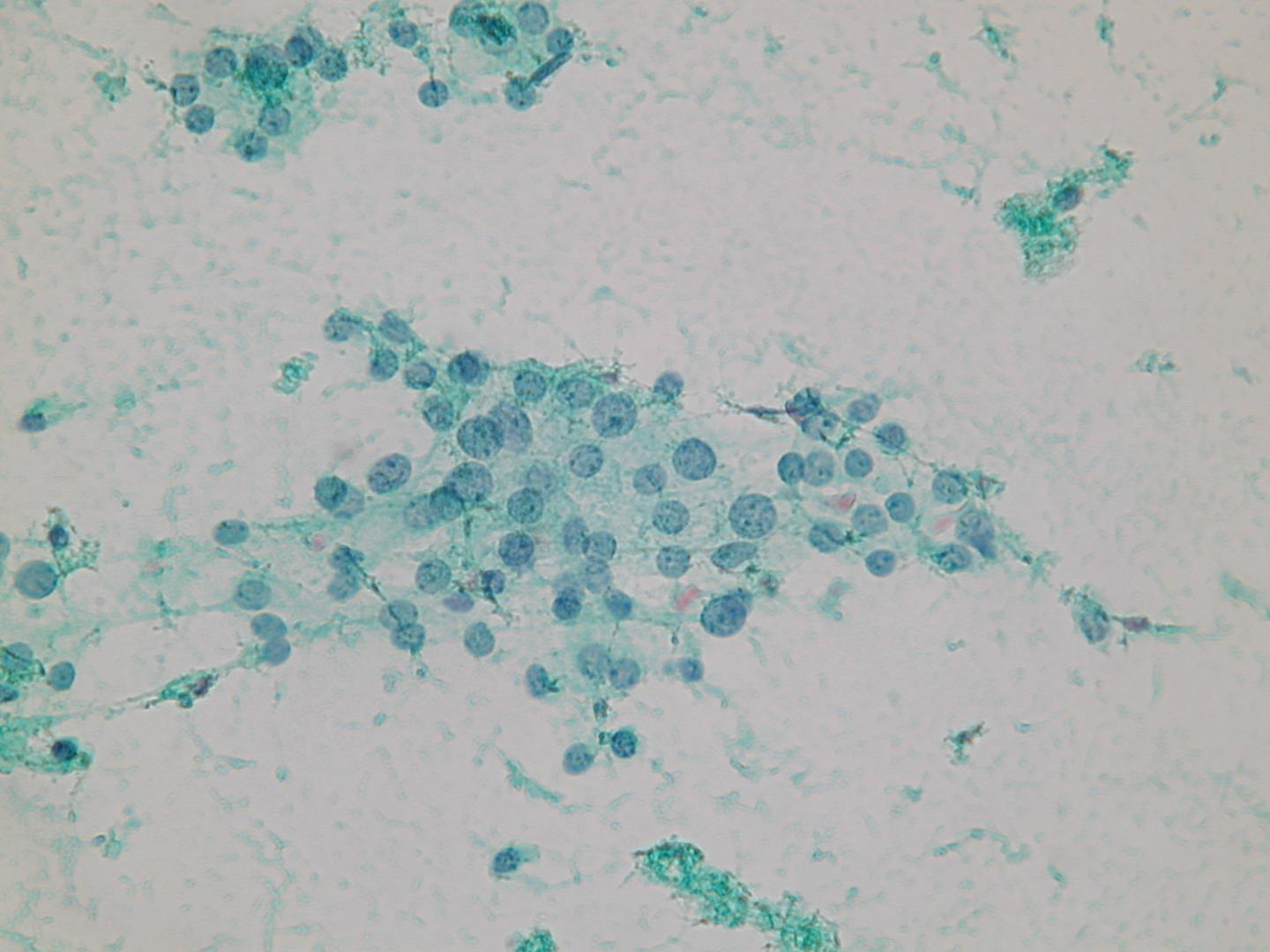
A microfollicular pattern:
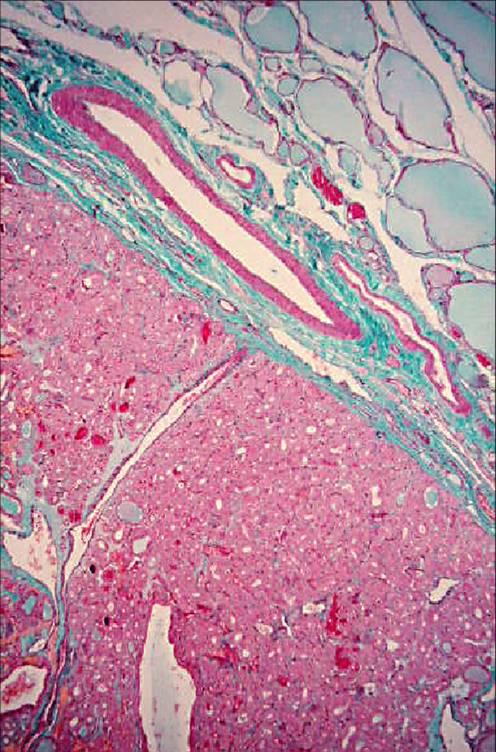
Adenoma follicular
Esta es una neoplasia benigna, que se presenta como un nódulo individual, usualmente no es mayor de 3cm de diámetro. Algunos de estos pueden producir hormonas tiroideas y consecuentemente causar hipertiroidismo (adenomas funcionales o “calientes”). El patrón histológico puede variar: macrofolicular (compuesto de grandes folículos llenos con coloide), microfolicular (con folículos mas pequeños), trabecular (con células foliculares organizadas en cintas)
Clasificación (Sin significado pronóstico)
- Simple
- Microfolicular
- Trabecular
- Oxifílico
- Atípico
- Papilar
- Células en anillo de sello
| Nodular hyperplasia | Follicular neoplasia |
|---|---|
| multiple | solitary |
| poorly encapsulated | encapsulated |
| architectural heterogeneity | uniformity of the architecture |
| cytologic heterogeneity | cytologic homogeneity |
| comparable areas in adjacent gland | different from surrounding gland |
| no compression of surrounding gland | compression of surrounding gland |
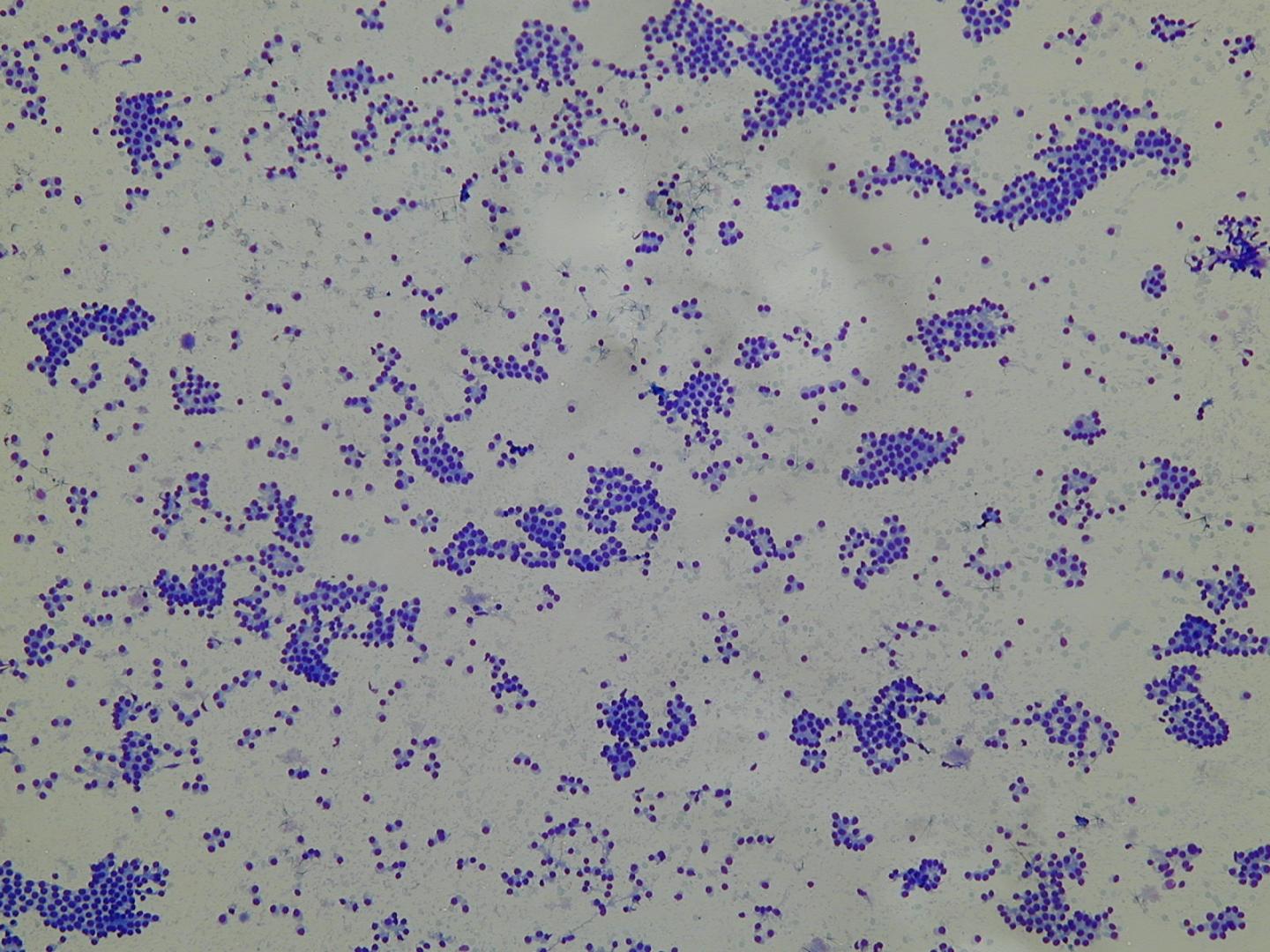
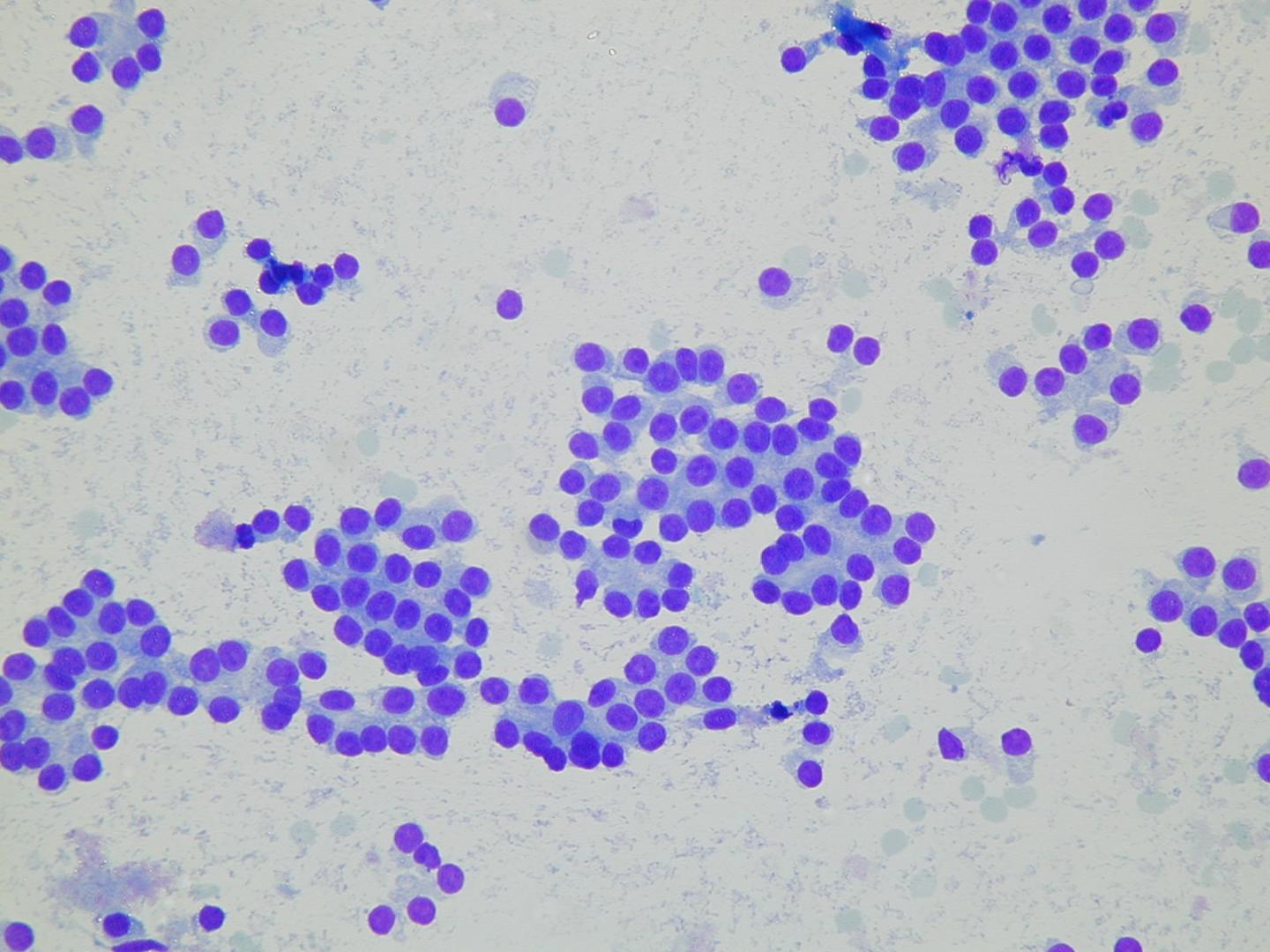
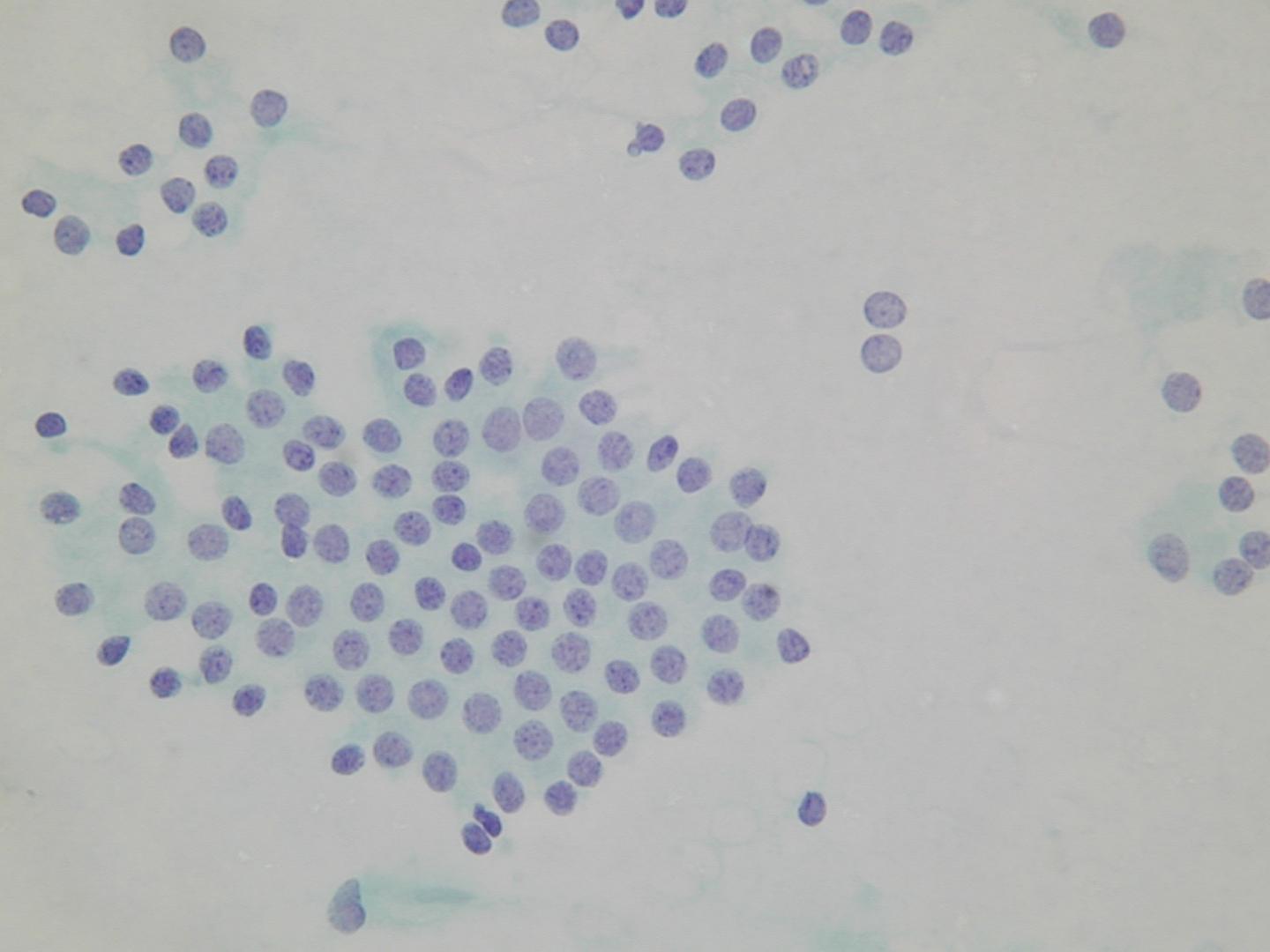
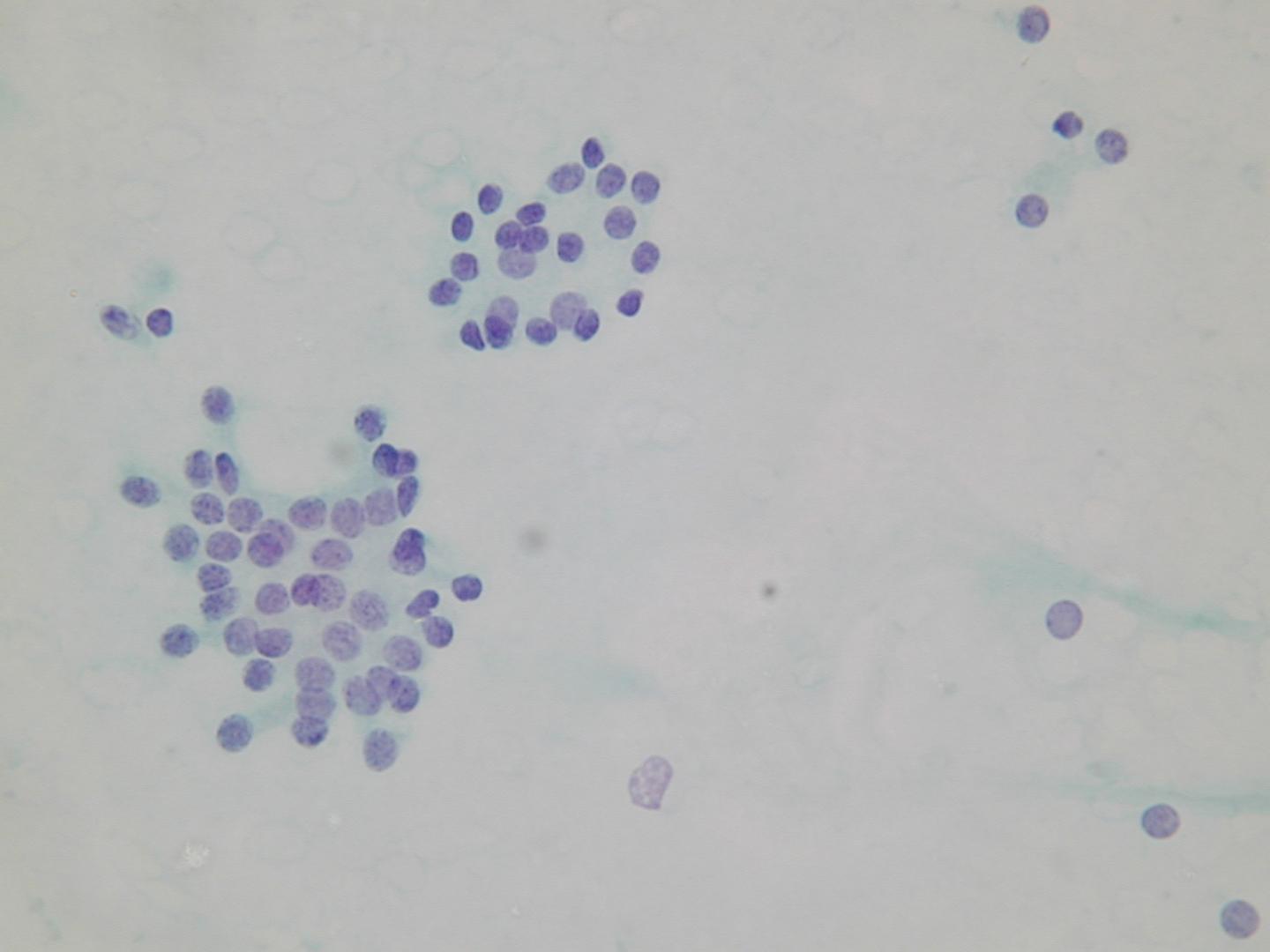
Microfollicular groups: