This content is also available in:
![]() English
English ![]() Italiano
Italiano ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
Falsos positivos em potencial
Apesar das implicações clínicas de falsos positivos parecerem menos significativas que dos falsos negativos, causam ansiedade desnecessária às pacientes e tratamentos excisionais desnecessários.
This is now known to increase the risk of premature rupture of membranes in pregnancy.
Although the risks are associated with large excisions rather than LLETZ (Castanon et al. 2014), it is clearly important to avoid false positive cytological reports.
|
A pista para se evitar falsos positivos é a familiaridade com processos reativos e metaplásicos do colo uterino na ausência de neoplasia |
É evidente que para escrutinadores que são expostos a toda gama de amostras regularmente – mas igualmente importante para patologistas que precisam ser familiarizados com as várias alterações benignas que são frequentemente e corretamente encaminhadas pelo citotecnologista como negativo.
É também importante no contexto de rastreamento primário da infecção pelo HPV quando será necessário emitir laudos negativos confiáveis, já que as amostras são todas de pacientes positivas para HPV de alto risco.
Falsos positivos em potencial são causados pelos seguintes itens:
- Alterações inflamatórias reacionais (por exemplo vaginite atrófica, cervicite folicular, endocervicite e reparo)
- Metaplasia (e.g. metaplasia escamosa imatura, metaplasia tubária, metaplasia tuboendometrial)
- Células endometriais – especialmente do segmento uterino inferior
- Células inflamatórias (e.g. linfócitos e histiócitos)
Alterações inflamatórias reacionais que podem mimetizar neoplasia
- Alterações associadas à atrofia são frequentemente associadas com processo inflamatório leve, que são geralmente subclínicos e não requerem tratamento. O padrão da vaginite atrófica é uniforme tanto na citologia convencional quanto no meio líquido; alterações bruscas de grupos de células com hipercromasia ou cromatina irregular devem ser identificadas e relatadas, se presentes.
- Qualquer forma de cervicite em mulheres na idade reprodutiva resulta em “desvio para a esquerda” com maior quantidade de células metaplásicas imaturas se comparadas com células superficiais. Esse fato é observado na reação ao Trichomonas vaginalis, que pode mimetizar HSIL – usualmente moderada em vez de acentuada.
- Endocervicite é caracterizada por perda da secreção de mucina pelas células colunares, tornando-as semelhantes a células esquamosas imaturas – por vezes mimetizando HSIL. Pode ser visto ainda em pólipos endocervicais benignos.
- Reparo é caracterizado por núcleos vesiculares com nucléolo proeminente e membranas nucleares regulares.
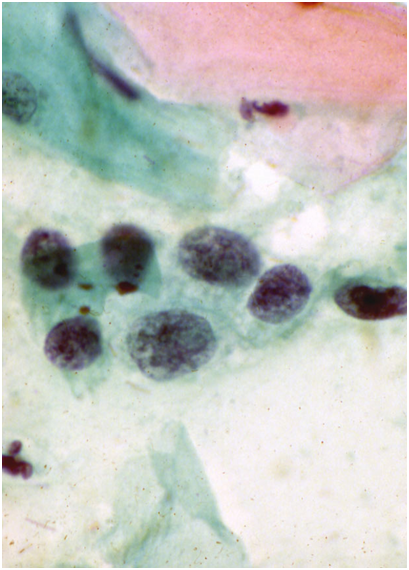
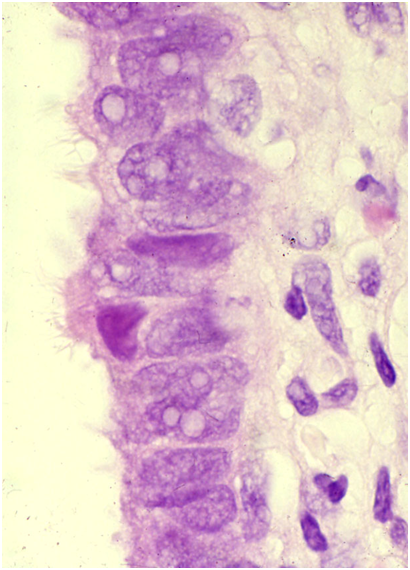
Figura 10.5 mostra exemplos de alterações reativas benignas com risco para erro diagnóstico de HSIL.
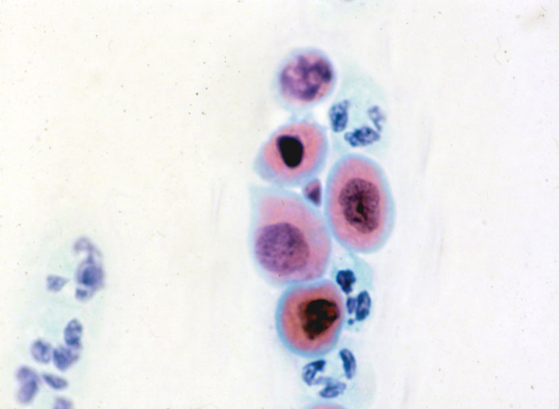
Núcleo degenerado e hipercromático com baixa relação núcleo/citoplasmática torna o diagnóstico de HSIL improvável em (a) e (b). Cariorrexis observada em grupo de células atróficas (a), típico da vaginite atrófica; facilitado quando o padrão se repete em todo o esfregaço. Pseudomultinucleação com citoplasma abundante e baixa relação núcleo/citoplasmática é observada em (b). A cromatina e as membranas são evidentes nas células glandulares pequenas e vacuoladas em (d). O padrão da cromatina e das membranas são regulares em (e) e não há pseudoestratificação para sugerir NIGC. Nucléolos proeminentes em (c) são típicos de reparo; nucléolo bem definido em (f), as membranas são bem definidas e com baixa relação núcleo/citoplasmática. A não ser em (a) e (d) nenhum desses casos foram considerados negativos; (c) foi erroneamente interpretado como “suspeito para adenocarcinoma”; (f) foi relatado como discariose moderada e Trichomonas foi identificado (em outra área da lâmina) na revisão; (b) e (e) foram considerados como limítrofes.
Alterações metaplásicas
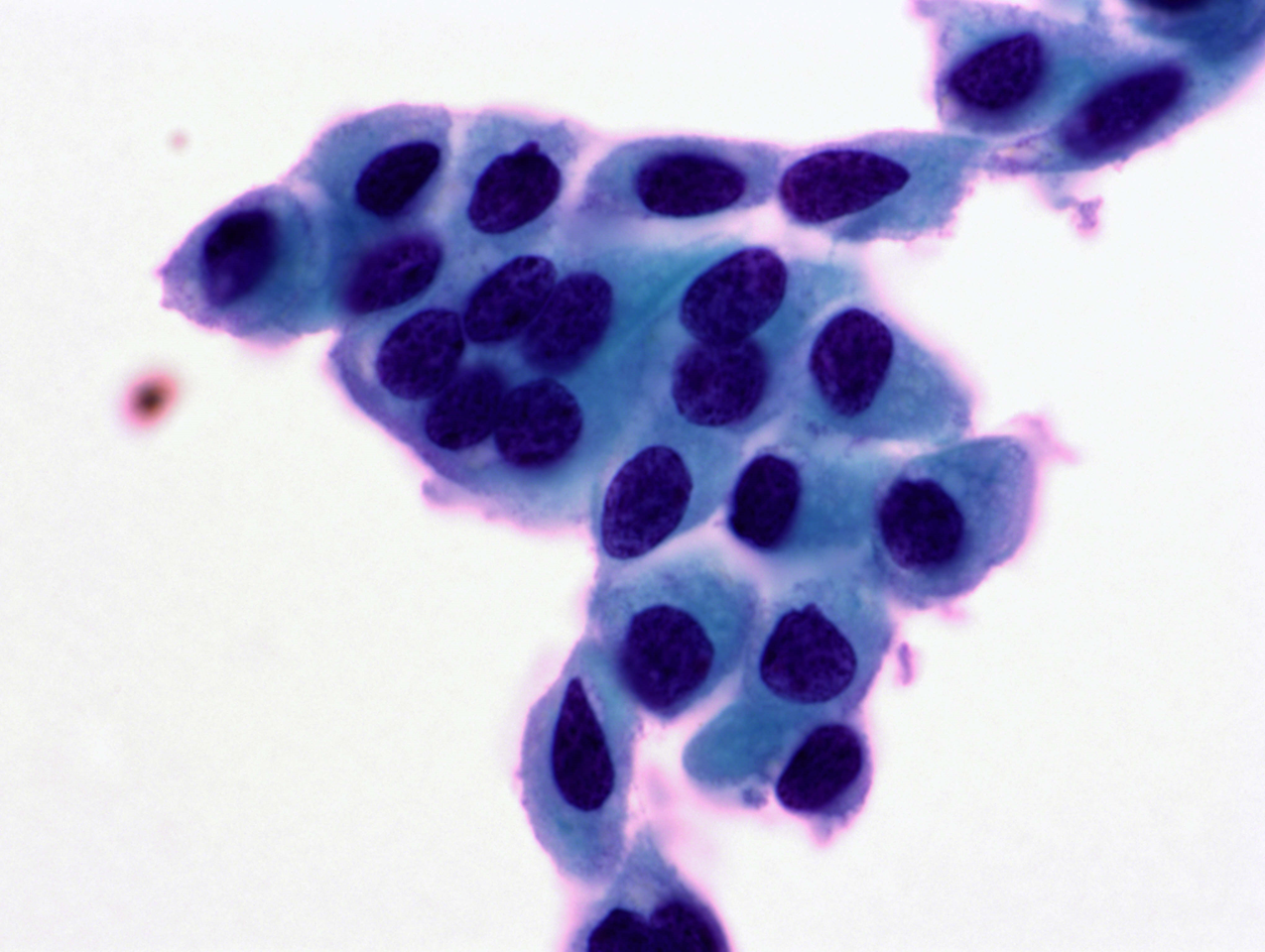
Metaplasia escamosa imatura é a armadilha mais comum e pode ser difícil de distinguir de HSIL – especialmente a “discariose moderada” ou “HSIL favorecendo NIC2”. Este problema é especialmente encontrado em citologias de meio líquido (ThinPrep) e foi considerado como um dos principais problemas na conferência da terminologia de BSCC.
- A atenção para a cromatina nuclear regular, membranas nucleares regulares e bem definidas, nucléolos proeminentes e relação núcleo/citoplasmática normal esperadas em uma célula metaplásica podem geralmente resolver a questão.
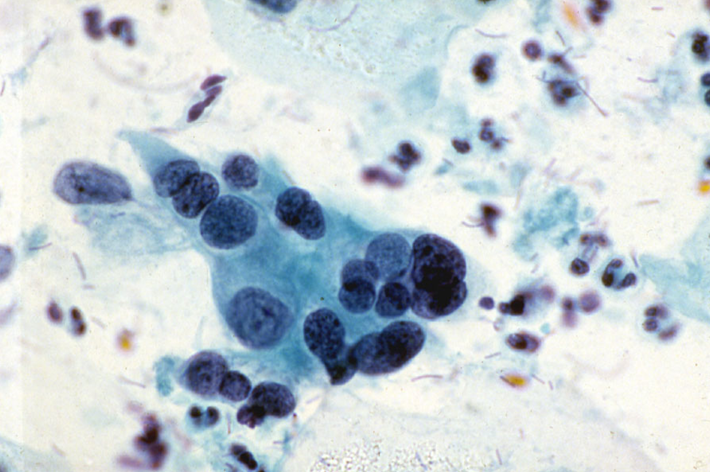
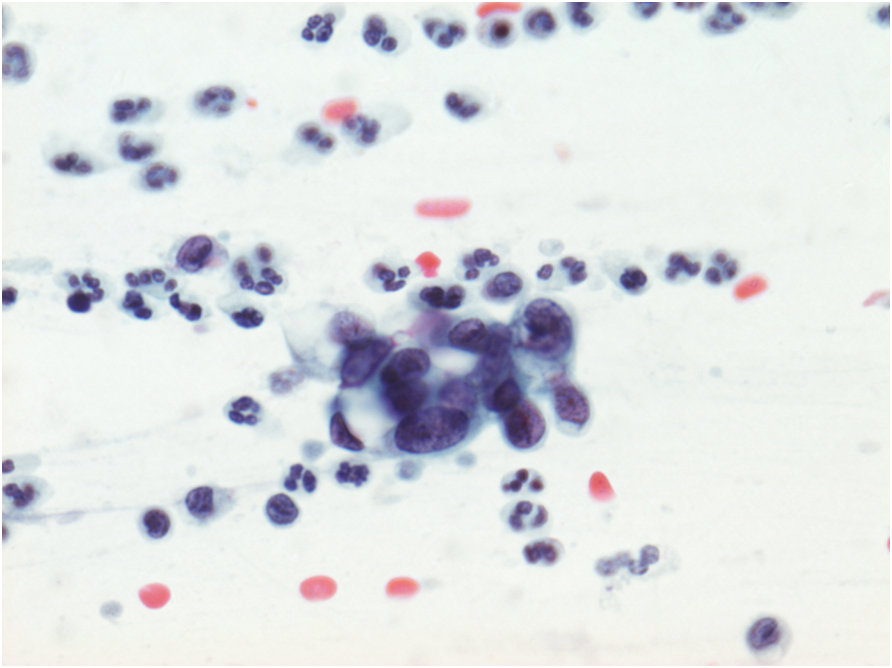
Figura10.6 Metaplasia imatura atípica
A LBC sample reported as moderate dyskaryosis/HSIL favour CIN2 that was found on cervical biopsy and LLETZ to be HPV only without CIN can be examined as a scanned slide [Link to win.eurocytology.eu/virtualslides/gyn/vs-031]. Cytology was reviewed as HPV change in squamous metaplasia, which could be regarded as ASC-US.)
Atypical immature squamous metaplasia
The term ‘atypical immature squamous metaplasia’ has been used in the past for histological biopsies, which corresponds to the difficulty of distinguishing immature metaplasia from SIL in cytology.
Immunostaining for p16 and Ki67 (Duggan et al. 2006) or CK17 and p16 (Regauer & Riech 2007).) and can distinguish immature metaplasia from LSIL and HSIL in the majority of cases. [Link to Chapter 12 – Cytology in a multidisciplinary setting]
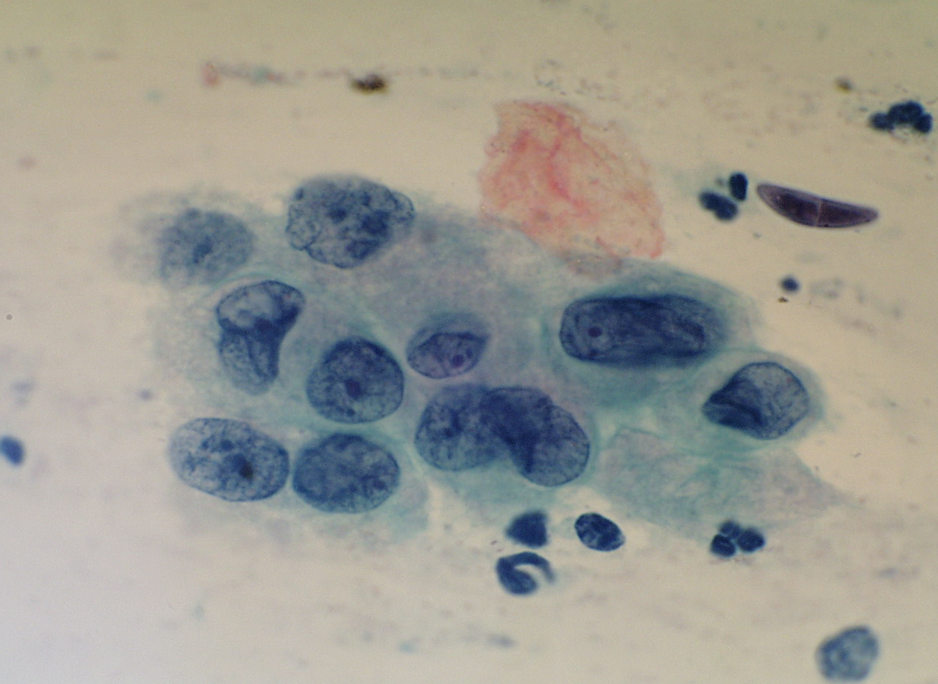
Tuboendometrioid metaplasia
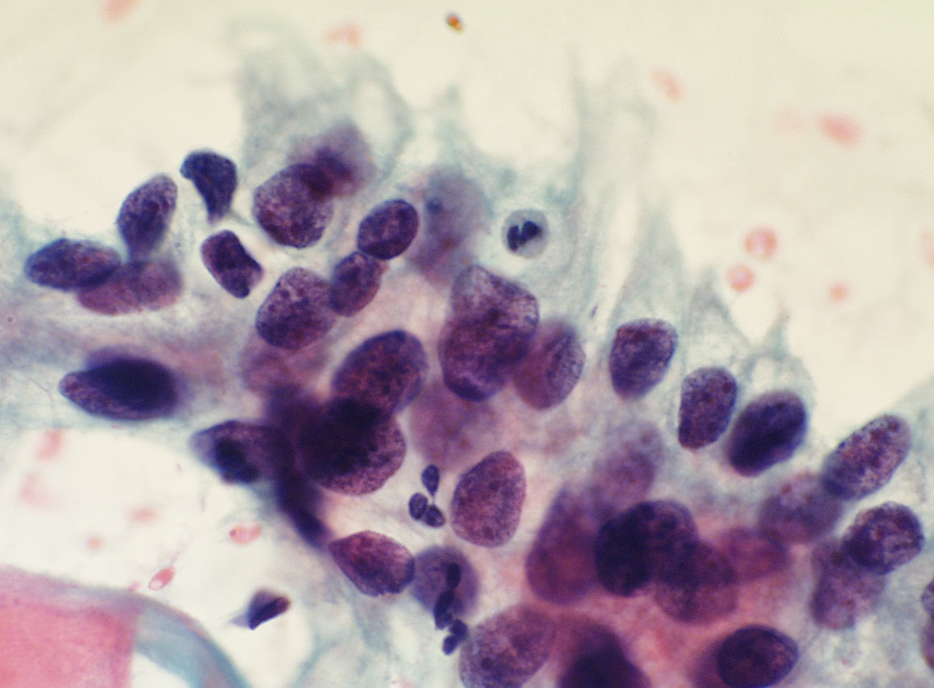
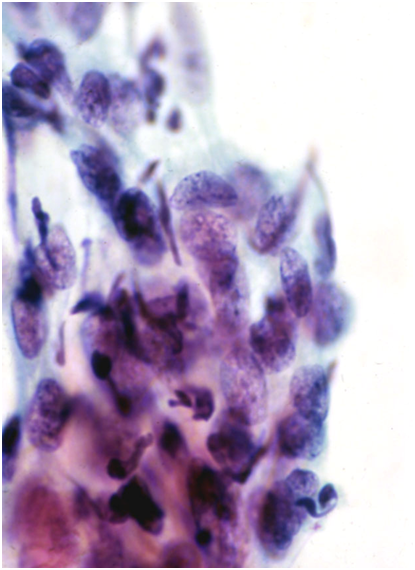
Tuboendometrioid metaplasia (TEM) and, less frequently, endometriosis may be seen on the cervix especially after procedures such as LLETZ and cone biopsy (Ismail 1991; Hirschowitz et al. 1994).Figure 10.7 (a-f) Endometrial and tubal metaplasia mimicking HSIL
Figure 10.7

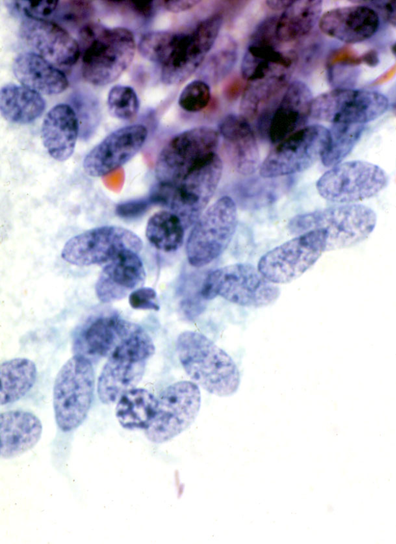
Tubal metaplasia
- Tubal metaplasia may be seen in the absence of TEM when it may mimic HSIL.
- Cytologically, the cells have plump enlarged nuclei. Basal plates can usually be seen even in the absence of cilia, which are diagnostic of tubal cells.
- Tubal metaplasia with inconspicuous cilia and basal plates may be a cause of false positive reports (Figure 10.8 b-c).
Figure 10.8
Endometrial cells
Endometrial cells may be a cause of false positive reports when they are seen outside the dates expected by date of the last menstrual period and when they do not present the classical appearances illustrated in Chapter 9b.
Two situations when endometrial cells have presented pitfalls in diagnosis are illustrated below: i) IUCD changes when the presence of a device was not known and ii) lower uterine segment sampling, especially when the endocervical canal is shortened after excisional biopsies of CIN.
Figure 10.9
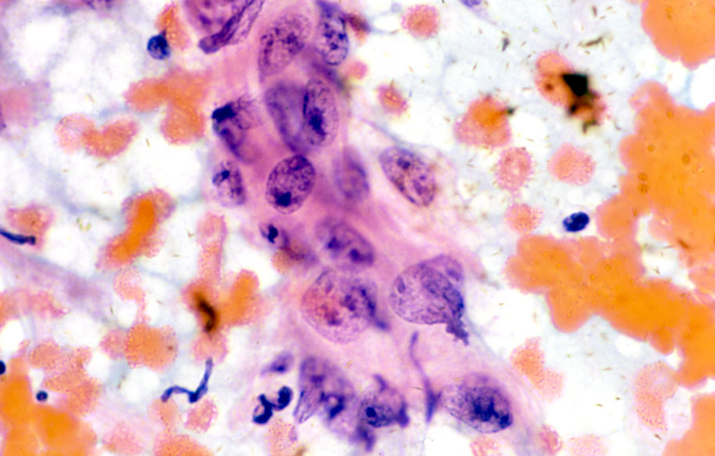
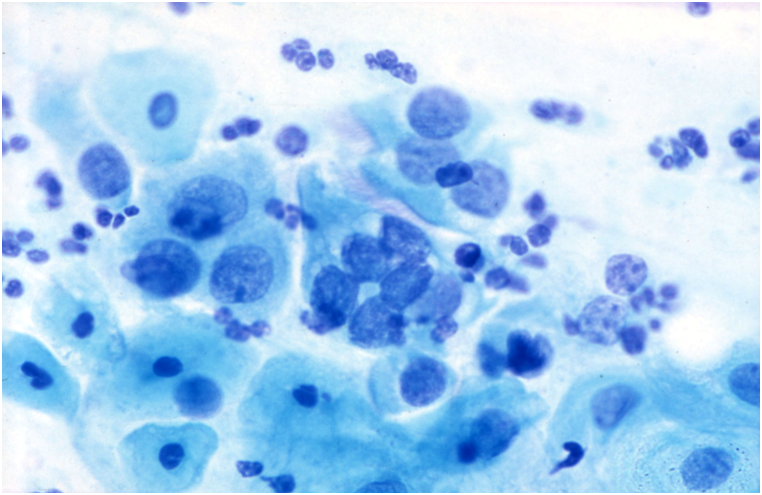
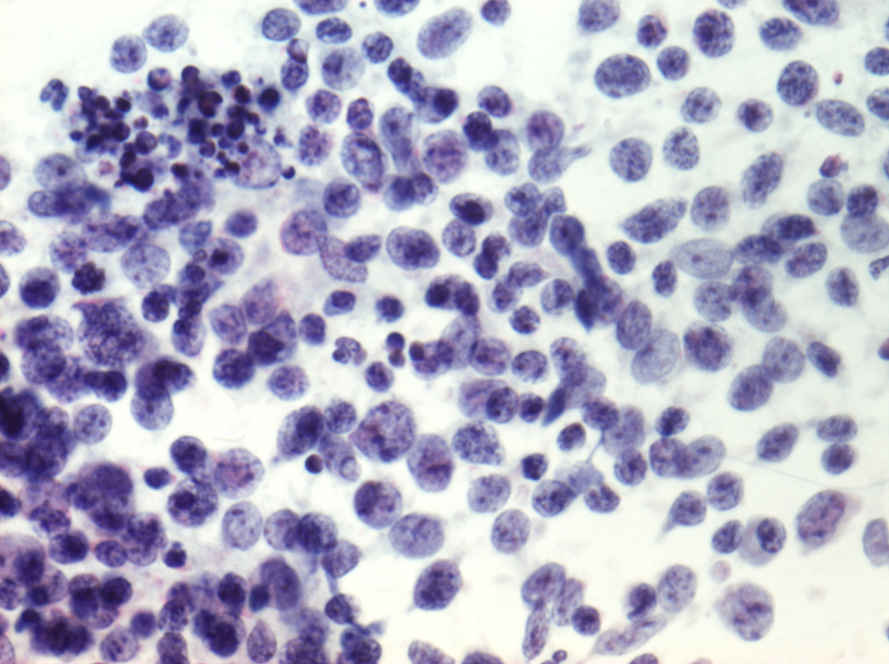
Células inflamatórias que podem simular HSIL (Figura 10.8)
Os histiócitos podem ter núcleos um tanto hipercromáticos que simulam células metaplásicas imaturas. Atenção para os arranjos com células isoladas do restante do arranjo e a presença de núcleos rechaçados podem ajudar no reconhecimento destas células
Linfócitos observados nos arranjos da cervicite folicular podem causar um problema se os núcleos dos corpos tingíveis não estiverem presentes. A borda fina do citoplasma azul nos linfócitos é indistinta em preparações fixadas em álcool e as células podem ser agrupadas em amostras de meio líquido, ao invés de dispersas como é visto em esfregaços convencionais. O padrão típico da cromatina finamente granular de pequenos linfócitos, associado a células linfóides imaturas maiores com nucléolos proeminentes adjacentes à membrana nuclear, é distinto das células endometriais do estroma e HSIL.
Figure 10.10 Células inflamatórias simulando NIC
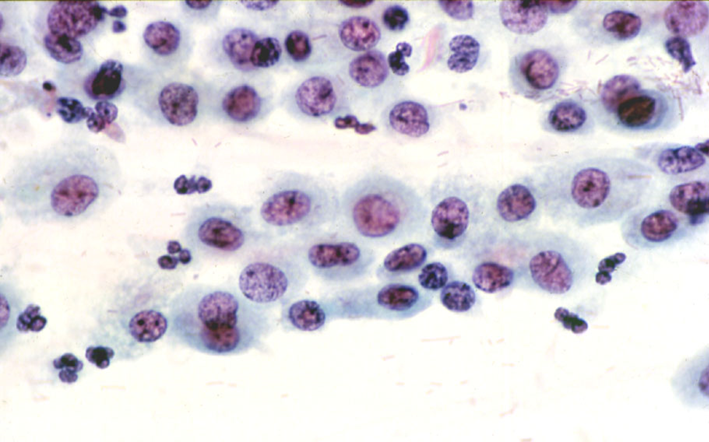
(a) Histiócitos num esfregaço normal
Como está óbvio a partir da seção anterior, o diagnóstico diferencial em muitos desses casos falsos positivos, podem ser confundido com alterações reativas e com risco de serem falsos negativos.
The main causes of false positive cytology
|