This content is also available in:
![]() English
English ![]() Italiano
Italiano ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
A maioria são tipos de HSIL bem reconhecidos, que não passarão despercebidos se os citologistas são familiarizados com eles.
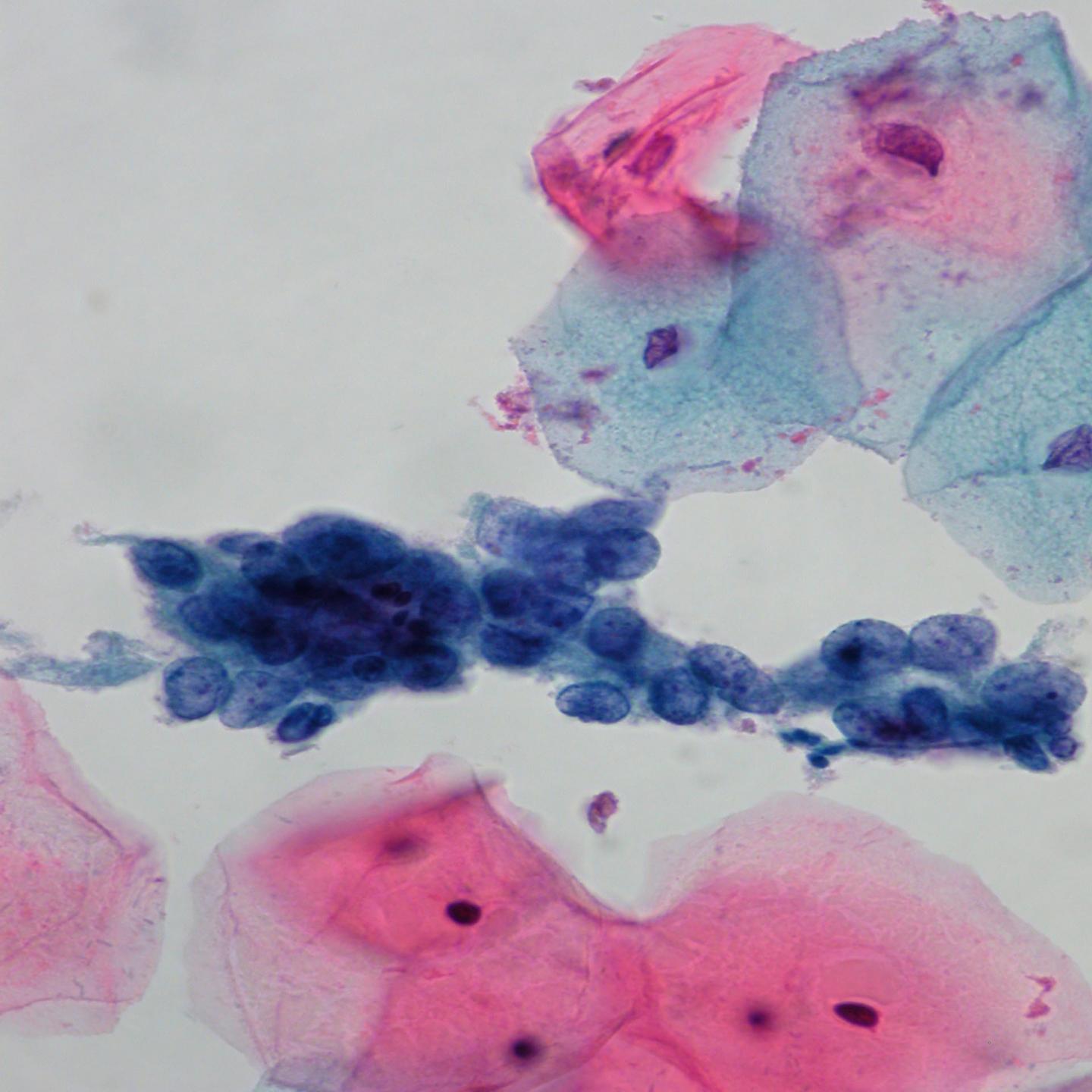
Discariose de pequenas células Essencialmente trata-se do carcinoma in situ, mas as células podem ser aparentemente pequenas, pouco maiores que neutrófilos. A atenção para o padrão da cromatina nuclear permitirá o reconhecimento desse tipo de HSIL, mesmo quando raras células atípicas estão presentes como na célula isolada abaixo, a única representada na lâmina.
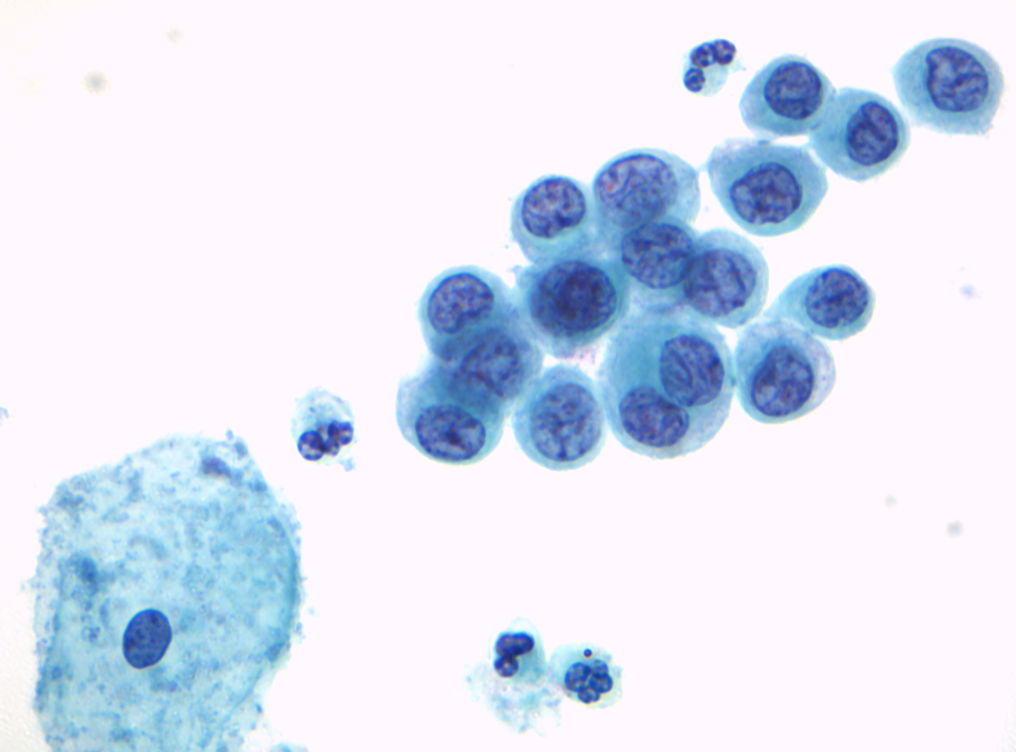
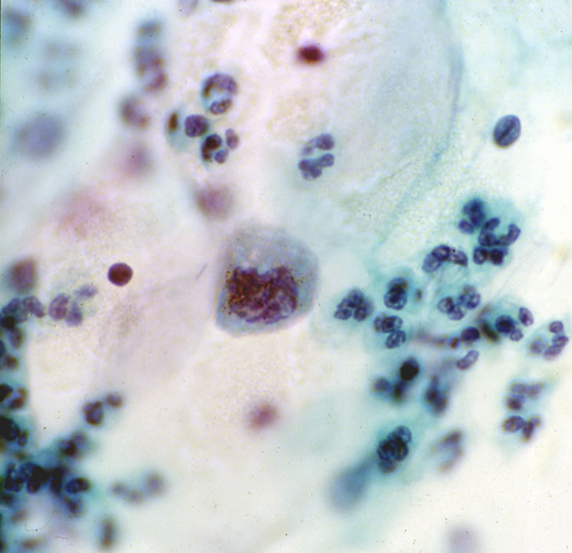
Figura 10.1 (b) Célula atípica isolada
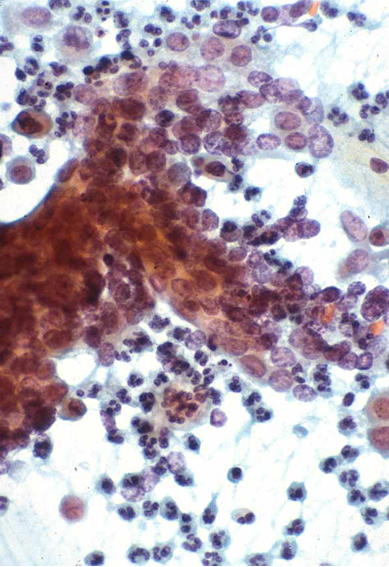
Discariose pálida Apesar do HSIL ser caracterizado frequentemente por hipercromasia, o núcleo pode ser pálido, tornando o diagnóstico diferencial com metaplasia escamosa imatura difícil – ou de células endocervicais quando as células são grandes.
In the BSCC Terminology Conference, approximately one-third of the respondents recognised Figure 10.2 (b) as severe dyskaryosis; one-third diagnosed follicular cervicitis and one-third ‘other reactive change’; 4% thought it was glandular neoplasia.
Small and pale cell HSIL as pitfalls in cervical cytology are described and illustrated in detail by Smith & Turnbull (1997).
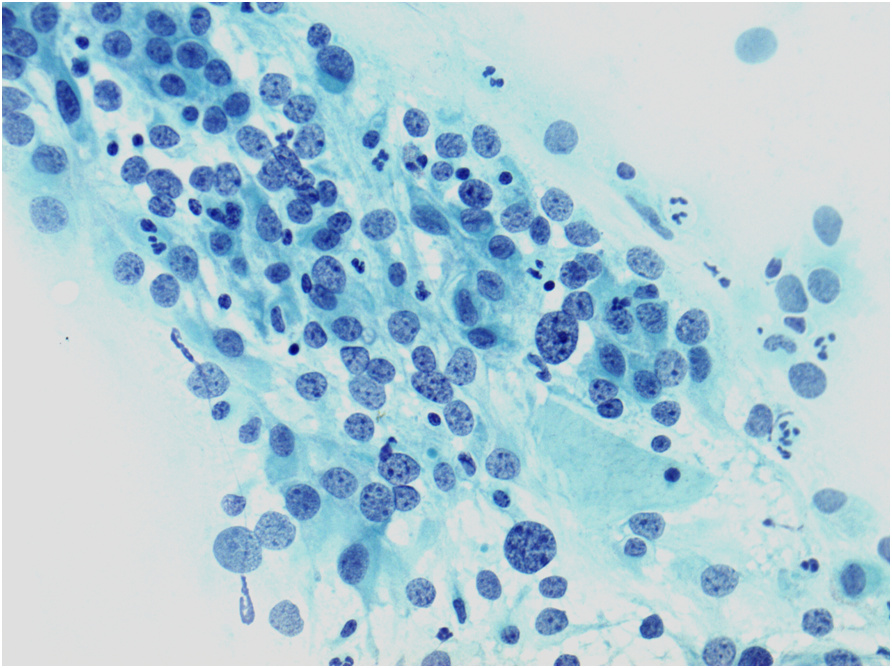
Grupos celulares hipercromáticos e sobrepostos
Microbiopsias ou grupamentos hipercromáticos e sobrepostos de HSIL ou até mesmo carcinoma podem ser negligenciados no escrutínio primário ou equivocadamente interpretados na revisão. Essas células podem mimetizar células endometriais, lençóis de células do segmento uterino inferior ou grupamentos de células endocervicais com alterações reacionais.
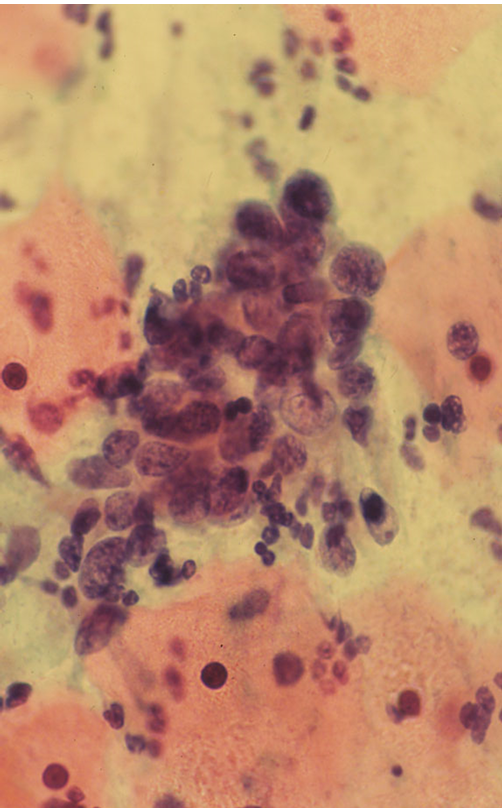
If the cells are not recognised as HSIL, in these cell groups or elsewhere on the slide, false negatives may be avoided in any or all these cases by reporting them as ASC-H rather than normal or reactive
‘Esfregaços inflamatórios’
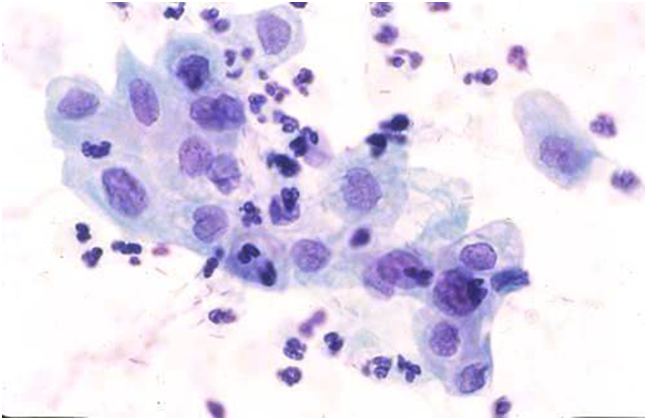
A interpretação equivocada de HSIL e até mesmo de carcinoma como achado inflamatório inespecífico Tem sido um risco para erros diagnósticos no passado. Atenção cuidadosa ao detalhe celular em objetiva de grande aumento permite que tal erro seja evitado.
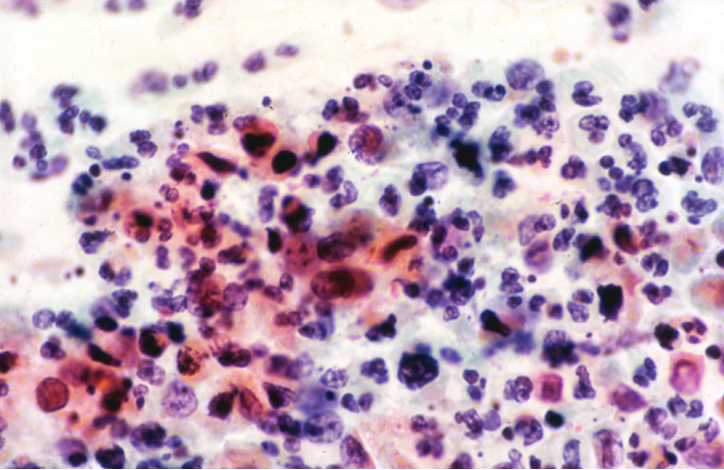
Figura 10.4 HSIL+ com processo inflamatório acentuado
Alterações citológicas com risco para laudos falsos negativos
Em citologia convencional, os esfregaços que apresentam células pequenas, com citoplasma pálido e em pequena quantidade representam um risco para laudos falsos negativo (Mitchell & Medley 1995; Demay 1996) e se microbiopsias são negligenciadas no escrutínio (Robertson &Woodend 1993; Demay 2000). Achados semelhantes são relatados em citologia em meio líquido utilizando-se ThinPrep (Leung et al. 2008). Microbopsias/grupos sobrepostos de células hipercromáticas e células atípicas esparsas são consideradas as causas mais comuns de falsos negativos e potenciais falsos negativos utilizando SurePath (Gupta et al.2013).
The main causes of false negative cytology
|
How to avoid false negative results
|