This content is also available in:
![]() English
English ![]() Português
Português ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
La maggior parte sono tipi di HSIL ben conosciuti che non verrebbero persi se fossero più familiari ai citologi.
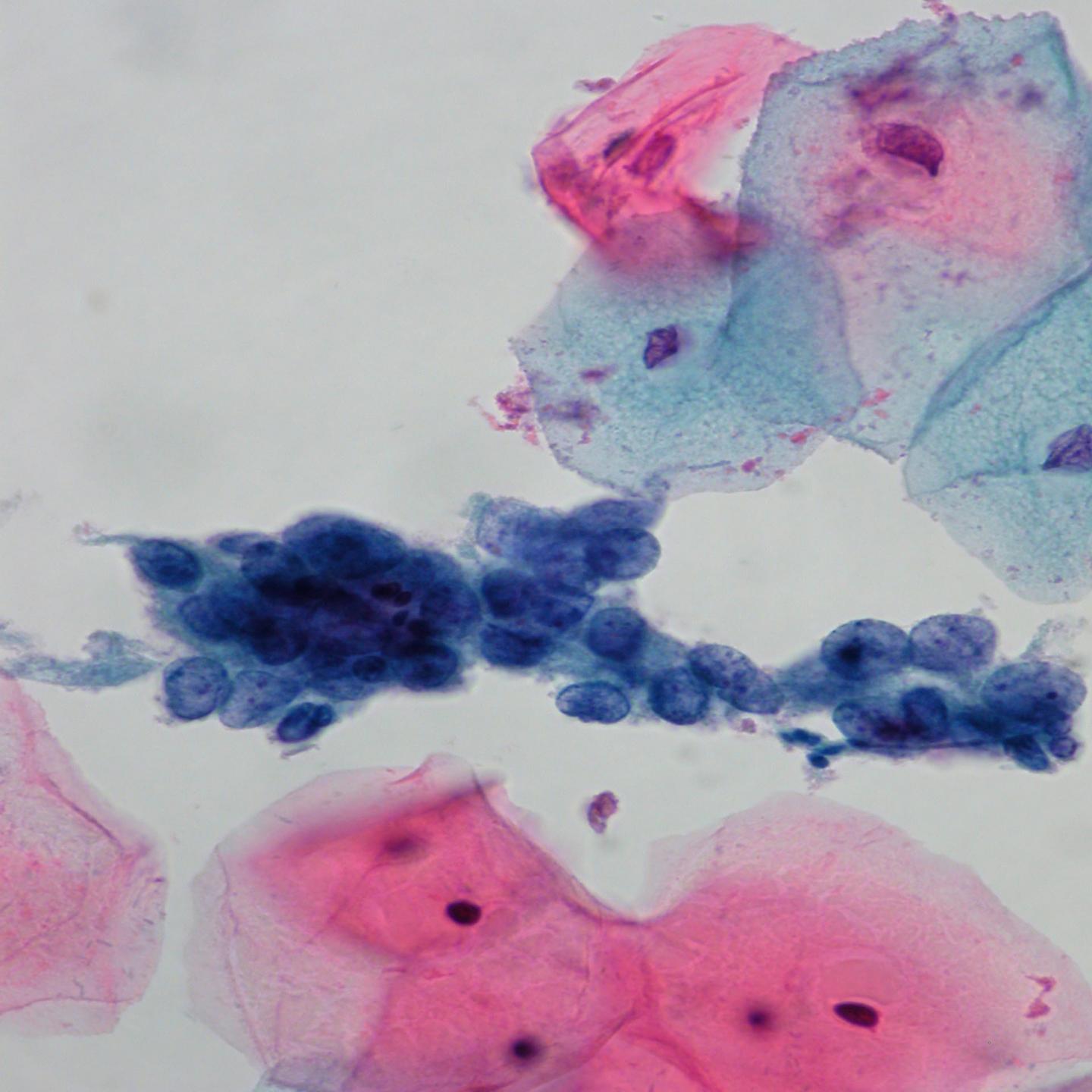
Discariosi a piccole cellule
Essenzialmente è un tipico carcinoma in situ ma le cellule appaiono ingannevolmente piccole e potrebbero essere un pò più grosse di un neutrofilo. Questo tipo di HSIL viene riconosciuto facendo attenzione al pattern della cromatina nucleare, anche quando sono presenti solo poche cellule anormali come la singola cellula nella figura sottostante che era l’unica nel vetrino.
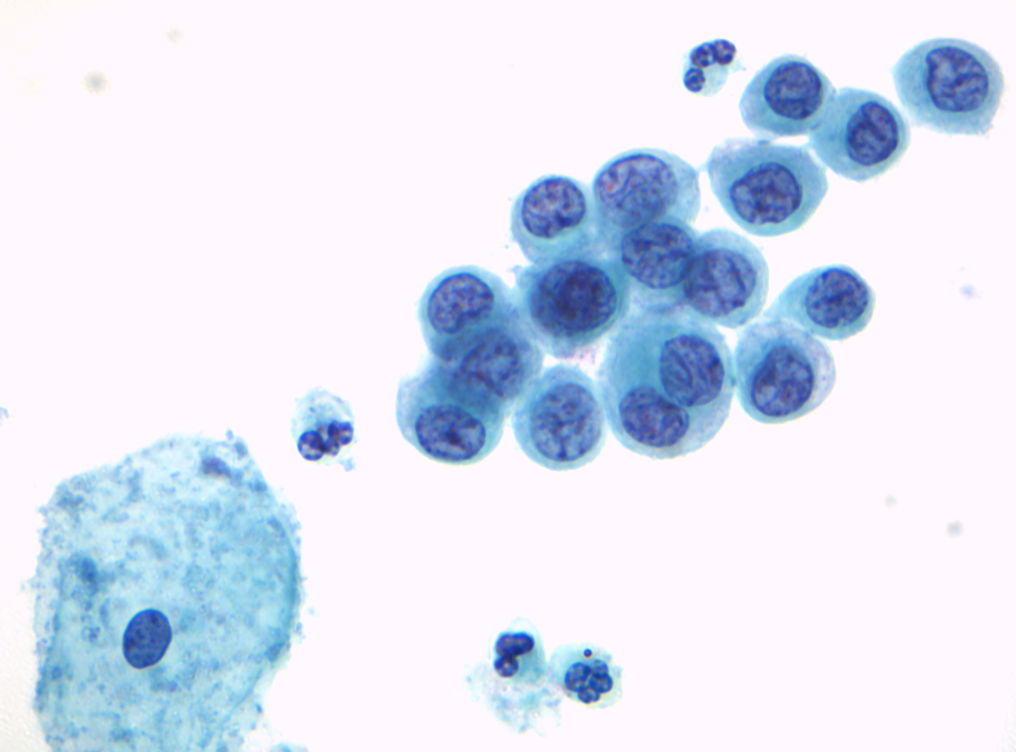
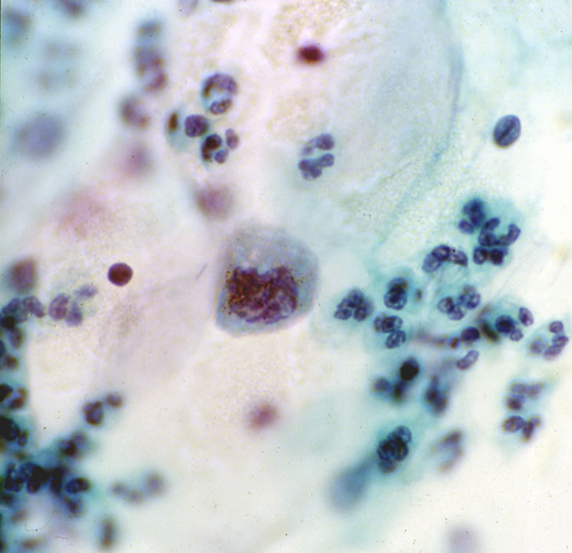
Figura 10.1 (b) Cellule anormali isolate
Discariosi Pallida
Sebbene HSIL sia di solito caratterizzato da ipercromasia, il nucleo potrebbe essere chiaro, rendendo difficile distinguerlo dalla metaplasia squamosa immatura o dalle cellule endocervicali, quando le cellule sono grandi.
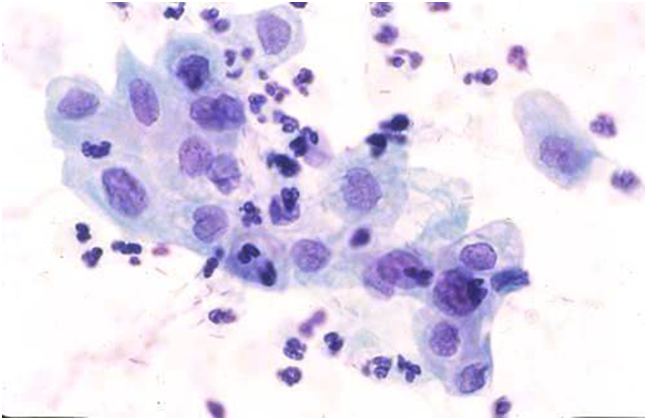
Gli HSIL con cellule piccole e chiare sono descritti come pitfalls e illustrati in dettaglio da Smith & Turnbull (1997)
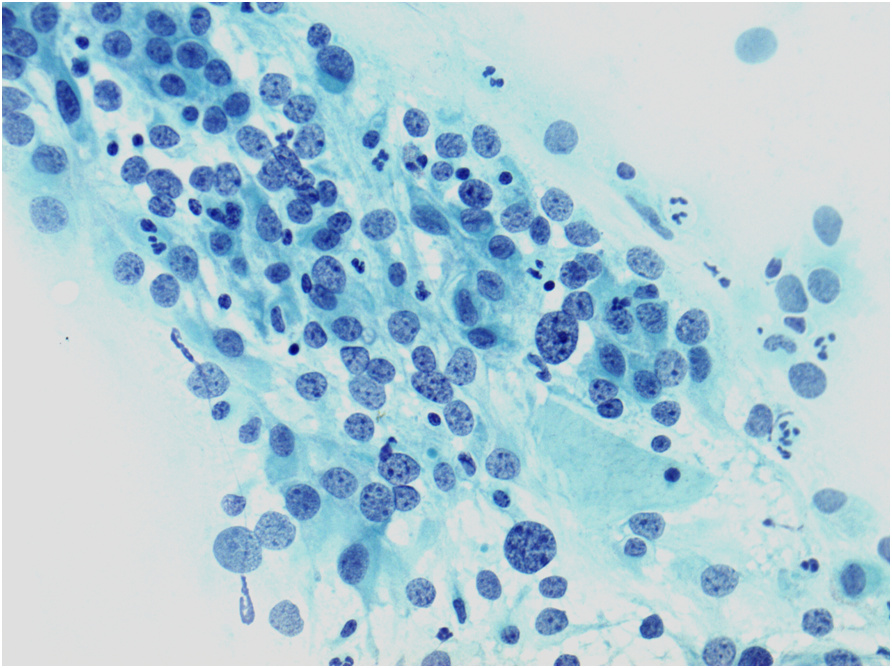
Gruppi ipercromatici affollati di cellule
Microbiopsie o gruppi ipercromatici affollati di cellule di HSIL o neoplastiche possono sfuggire allo screening primario o essere interpretate erroneamente durante la revisione. Queste cellule possono assomigliare a quelle endometriali, ai fogli di cellule provenienti dell segmento uterino inferiore o ai clusters di cellule endocervicali con alterazioni reattive.
Figura 10.3 (a-c) Gruppi ipercromatici affollati di cellule
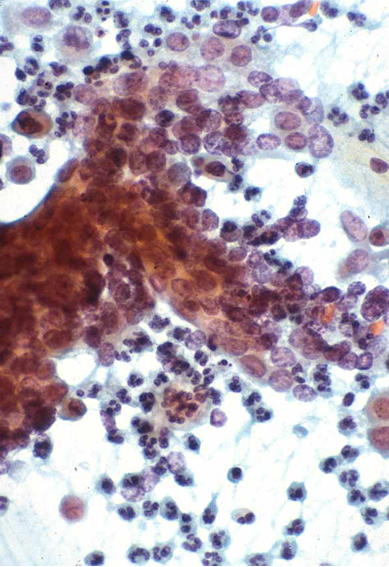
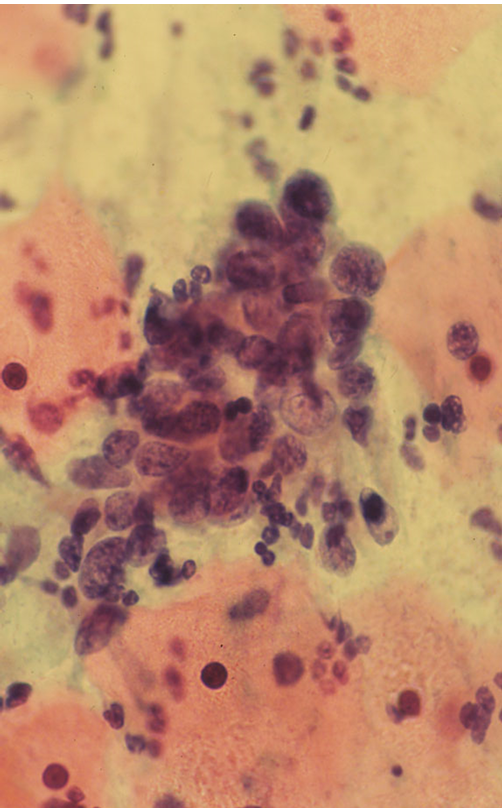
Questi esempi di gruppi ipercromatici affollati di cellule di HSIL sono stati dimostrati essere tutti CIN3. Alcuni possono essere visti sui link diretti al questionario della terminologia BSCC e Denton et al. 2008.
“Campioni infiammatori”
Una interpretazione errata di un HSIL o addirittura di una neoplasia come una infiammazione non specifica è stata causa di diagnosi errate nel passato. Fare attenzione ai dettagli cellulari ad alto ingrandimento dovrebbe evitare questo pitfall.
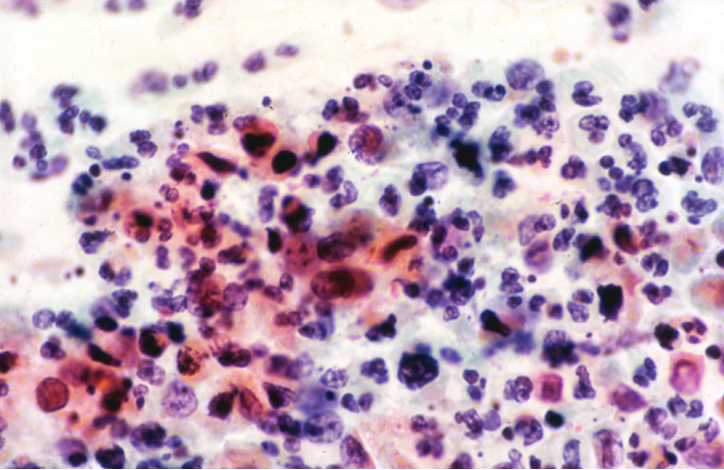
Figura 10.4 HSIL+con infiammazione severa
Alterazioni citologiche a rischio di falso negativo
Gli strisci convenzionali hanno il rischio di venire refertati come falsi negativi quando le cellule appaiono piccole, pallide e ridotte in numero (Mitchell & Medley 1995; Demay 1996) e se le “microbiopsie” vegono trascurate allo screening primario (Robertson & Woodend 1993; Demay 2000). Sono stati riportati anche gli stessi risultati per la citologia su base liquida con ThinPrep (Leung et al. 2008).
Microbiopsie/gruppi ipercromatici affollati di cellule e singole cellule anormali disperse sono le cause più comuni di falsi negativi e potenziali falsi negativi se si usa SurePath (Gupta et al.2013).
The main causes of false negative cytology
|
How to avoid false negative results
|