This content is also available in:
![]() English
English ![]() Italiano
Italiano ![]() Português
Português ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
CIN und Plattenepithelkarzinom
Es gilt als anerkannt, dass dem invasiven Plattenepithelkarzinom, welches den häufigsten histologischen Typ des Zervixkarzinoms darstellt, ein präinvasives Krankheitsstadium vorangeht, in welchem sich die abnormen Zellen über das Epithel ausbreiten. Dabei wird das normale Plattenepithel der Zervix durch abnormes Epithel neoplastischer Zellen ersetzt. Dieses nicht-invasive Krankheitsstadium wird als zervikale intraepitheliale Neoplasie bezeichnet (CIN) und steht unmittelbar in Zusammenhang mit einer vorangegangenen Infektion und Integration von HPV (siehe Kapitel 3).
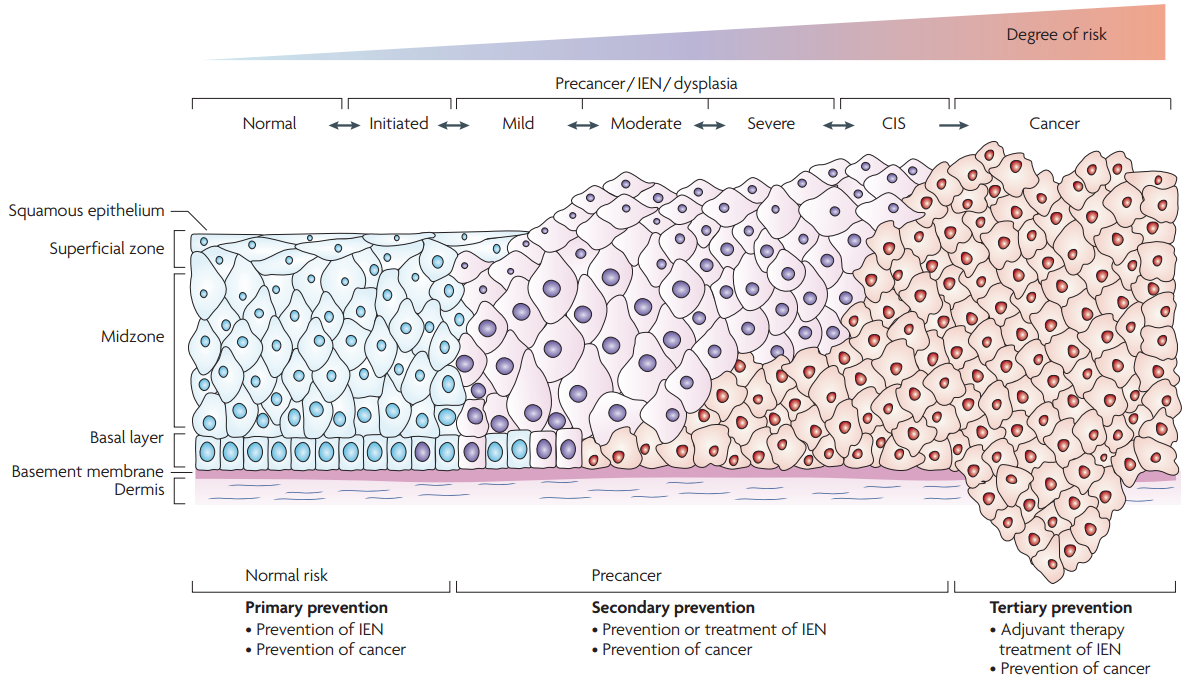
The development of CIN involves a progression from early changes (CIN1) involving the deeper layers of the epithelium to full thickness involvement at its most severe (CIN3) equating to carcinoma in situ (Figure 4.1).
|
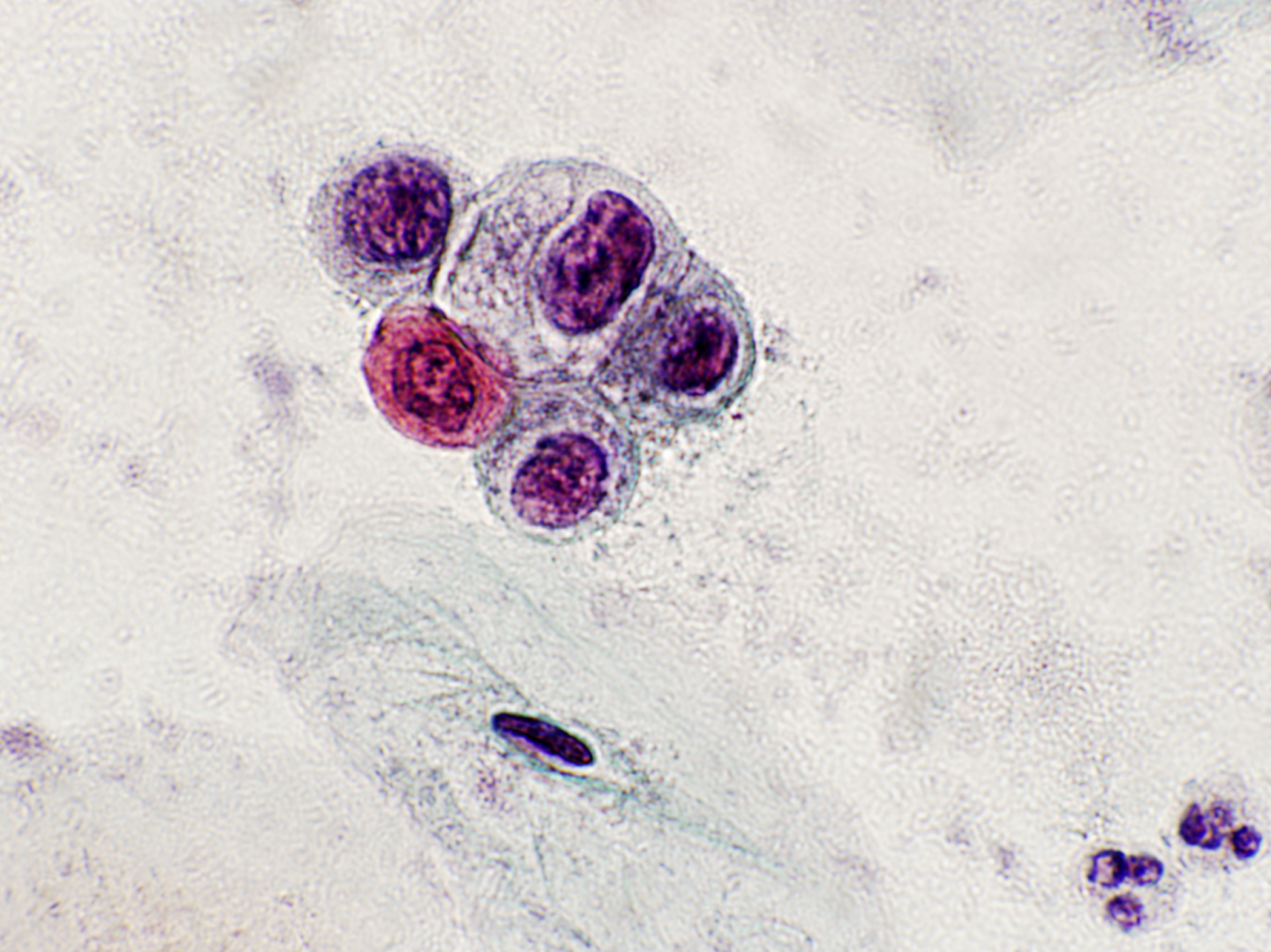
Figure 4.2 (a-c). CIN1
FIGURE
(a) CIN1 in a cervical biopsy; (b) LSIL in a Pap smear; (c) LSIL with koilocytosis (see Figures 9c-2a and 9c-3b in Chapter 9c and scanned slides linked to that chapter).
CIN1 bzw. Koilozytose einer HPV-Infektion bildet sich für gewöhnlich innerhalb von 9-12 Monaten spontan wieder zurück. Es gibt jedoch zahlreiche Follow-up Studien, die sehr unterschiedliche Progressionsrisiken zu CIN2-3 und für eine äußerst kleine Minderheit der Patientinnen eine resultierende Gefahr für ein invasives Karzinom zeigen (Ostör 1993; Holowaty 1999; Bansal et al. 2008).
Eine groß angelegte retrospektive Follow-up Studie von Holowaty et al. zur leichten, mäßigen und schweren Dysplasie konnte belegen, dass sich der Großteil der Fälle einer leichten Dysplasie (62.2%) und mäßigen Dysplasie (53.7%) zurückbildet (Endpunkt: zwei negative Abstriche innerhalb von 2 Jahren) während das Progressionsverhalten zu einer mäßigen Dysplasie oder höhergradigen Läsion (CIN2+) ca. 25% innerhalb von 5 Jahren beträgt, was sich auch mit den Ergebnissen anderer Studien deckt.
A large retrospective follow-up study of mild, moderate and severe dysplasia by Holowaty et al. showed that the majority of cases of mild (62.2%) and moderate dysplasia (53.7%) regressed (two negative smears within 2 years) while progression to moderate dysplasia or worse was approximately 25% within 5 years, which is consistent with other studies.
Progression der leichten Dysplasie (vgl. Holowaty et al.)Moderate Severe+ Innerhalb von 2 Jahren 11.1% 2.1% Mäßige Dysplasie 20.4% 5.5% Schwere Dysplasie 28.8% 9.9% |
Likelihood of progression depends on persistence of HPV, its integration into the host genome and its type (Jaisamrarn et al. 2013).
- HPV16 and 33 have the highest risk of progression to CIN3
- HPV16 and 31 to have the least likelihood of regression
High-grade CIN
CIN2 and CIN3 are managed as ‘high-grade’ CIN and usually treated by excision or ablation when diagnosed at colposcopy.
CIN2 is an intermediate lesion and there is evidence from the ALTS trial that around 40% resolves spontaneously but was less likely to do so when HPV16-related (Castle et al. 2009). The retrospective study by Holowaty et al. (1999) showed that the majority of moderate dysplasia regressed dysplasia regressed (53.7%) while progression was more likely than for mild dysplasia.
Progression of moderate dysplasia (from Holowaty et al.)Severe+ Within 2 years 16.3% Within 5 years 25.1% Within 10 years 32.0% |
Die kumulative statistische Progressionsrate der mäßigen Dysplasie (1.2) zum invasiven Karzinom bezogen auf 100 Frauen innerhalb von 5 Jahren, liegt zahlenmäßig zwischen der leichten Dysplasie (0.4) und der schweren Dysplasie (3.9) (kompletter Datensatz einschl. Konfidenzintervallen vgl. Holowaty et al. 1999)
CIN2 ist charakterisiert durch Kernatypien mit erhöhter Mitoserate ausgedehnt auf die basalen 2/3 des Epithels. Eine Koilozytose ist kaum bis nicht vorhanden.
Figure 4.3 (a-b). CIN2 (moderate dysplasia): intermediate risk of progression
FIGURE
(a) HSIL, favour CIN2, on a LLETZ; (b) HSIL (favour CIN2) (see Figure 9c-7b and scanned slides linked to Chapter 9c)
In view of its intermediate position between CIN1 and CIN3 in terms of risk of progression and the clinical importance of deciding whether CIN2 should be managed as a high-grade precancerous lesion, immunohistochemistry using the cyclin-dependent kinase inhibitor p16INK4A is now recommended in the US to improve consistency of diagnosis and define high-grade CIN (Galgano et al. 2010; Darragh et al. 2012).
P16INK4A Färbung hilft in der Unterscheidung einer CIN2 zu
|
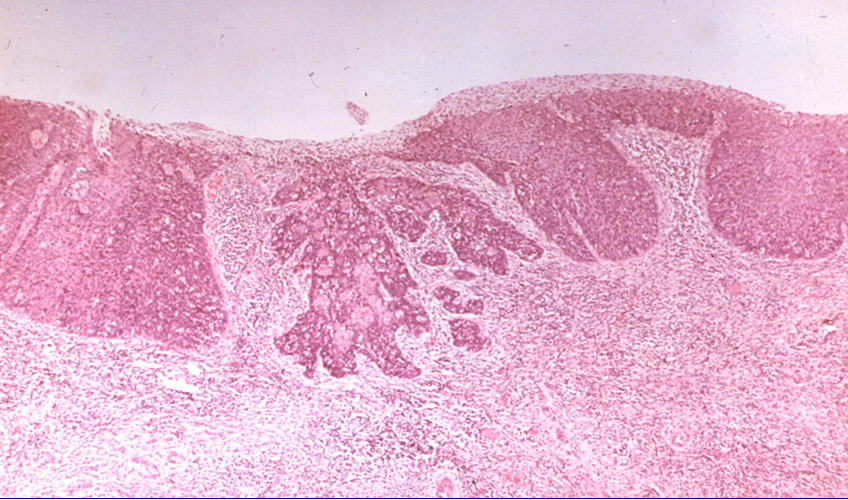
CIN3 ist charakterisiert durch Kernatypien, die die gesamte Epitheldicke betreffen, mit erhöhter Mitoserate in allen Schichten. CIN3 (and severe dysplasia) equates to carcinoma in situ, which term is seldom used nowadays.
Risk of progression is highest for CIN3 and inter-observer variation is considerably less than for CIN1 or CIN2 (Stoler et al. 2001). Microinvasive carcinoma is almost always seen in a background of widespread CIN3 further demonstrating its malignant potential. The exact risk is difficult to calculate because most CIN3/carcinoma in situ is treated when diagnosed.
Figure 4.4 (a-c). CIN3 and occult cancer