This content is also available in:
![]() Español
Español ![]() Português
Português ![]() Čeština
Čeština ![]() Magyar
Magyar ![]() Polski
Polski ![]() Türkçe
Türkçe
Sampling methods
Simple cytobrush sampling is easier in the oral cavity in case the lesion is localized (vesicular, ulcerated lesions).
Free hand FNAB is useful in superficial lesions since they must be localized and fixed using the samplers fingers. Superficial, subcutaneous or submucosal lesions may not need US guidance; US guidance is useful to see the anatomical situation of the nodule for avoiding complications (bleeding, hematoma) and is absolutely necessary in deep seated lesions (tumors of nasopharynx, deep lobes of salivary glands) or large cystic lesions. Small lesions localized next to the large vessels also need guidance.
Since CT guidance is not a real time method, it is useless in this anatomical area. We may however use the indirect CT guidance: having had the opportunity of an onsite US scan or having visible CT scan on site the site of the entering point of the puncture, the direction of the needle movement and the length of it can be determined in beforehand for a free hand puncture. This combination of methods, knowledge and experience is extremely important in our everyday practice.
“indirect” CT localization

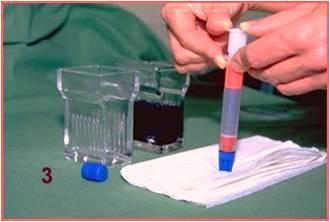
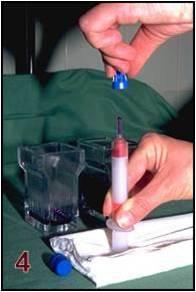
Staining methods
We may use Giemsa (air dried smears), Papanicolaou or H&E staining as well. Papanicolaou is informative in squamous cell lesions, and so is H&E. Giemsa stained specimens can show metachromasia: extracellular matrix and the cytoplasm of myoepithelial and connective tissue cells show metachromatic purple staining. Giemsa stain is furthermore a simple, quick, one step method resulting in different colours.These cellular and extracellular components play a very important role in the diagnostics of head and neck, especially salivary gland lesions.
Immunocytochemistry can be performed if needed. For immonucytochemistry cell block preparation, handmade CellPrint® specimens or cytospin prepared cells may also be used.In the 21st century molecular diagnostic methods may also be important in diagnosing some tumors. If needed, think of a possible molecular preparation when processing cytology material. All aspirated cells do contain the DNA and RNA needed for molecular methods, the preparation is simple. The identification of single cells from which the DNA or RNA has been removed may be difficult, for we get a mixture of cells on the slides. In case the tumor cells were chosen following introductory staining and diagnosis the method is easily evaluable. For direct molecular studies FISH technique must work easily in all kinds of cells.
The most important questions to be answered by using molecular tests in the head and neck cytopathology:
- Diagnosis of metastatictumors: e.g. malignant melanoma, epithelial metastatic tumors from the thyroid, lung, breast, etc. Soft tissue tumor metastases, stomach, other gastrointestinal tumor metastasis or metastasis of ovarian origin.
- The MASC (mammary like serous carcinoma of the salivary gland) always contains a diagnostic translocation resulting in a fusion gene: (t(12;15) (p13;q25) ETV6-NTRK3 fusion gene) this can be studied by FISH method already.
- Very much promising is the translocation in mucoepidermoidcarcinoma: t11;19) (q21;p13) MECT1(CRTC1)-MAML2.. The presence of this translocation seems to result in a more stable karyotype hence it suggests a better prognosis
There are some more molecular studies in the salivary gland pathology, (e.g. PLAG1 and HMGA2 gene in pleiomorphic adenomas they are however no specific important diagnostic role yet.
Hand made CellPrint® LB preparation