This content is also available in:
![]() Español
Español ![]() Português
Português ![]() Čeština
Čeština ![]() Magyar
Magyar ![]() Polski
Polski
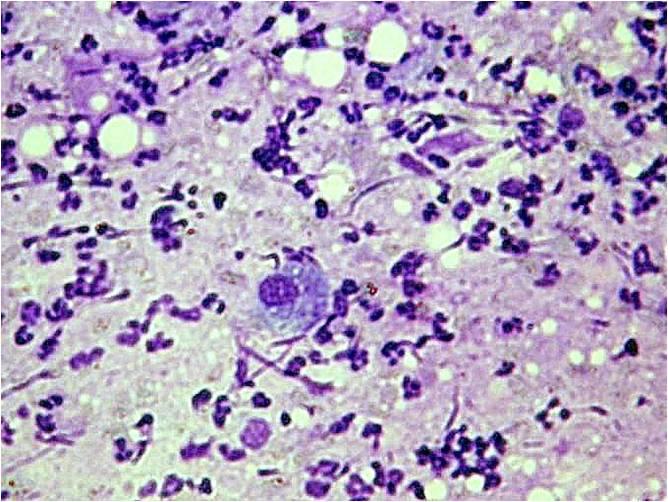
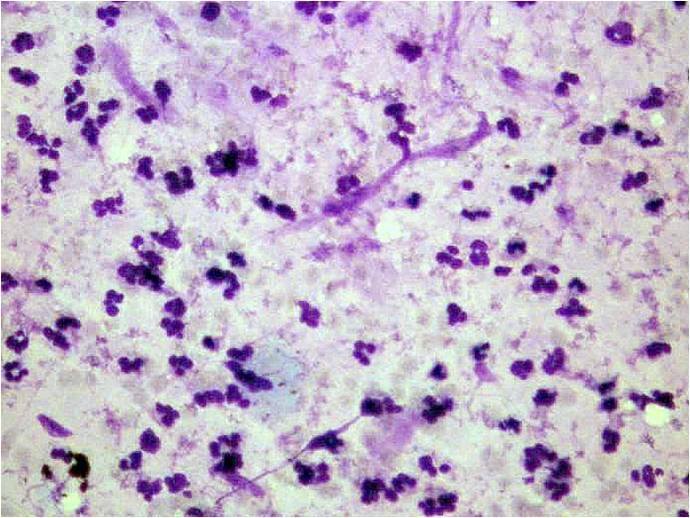
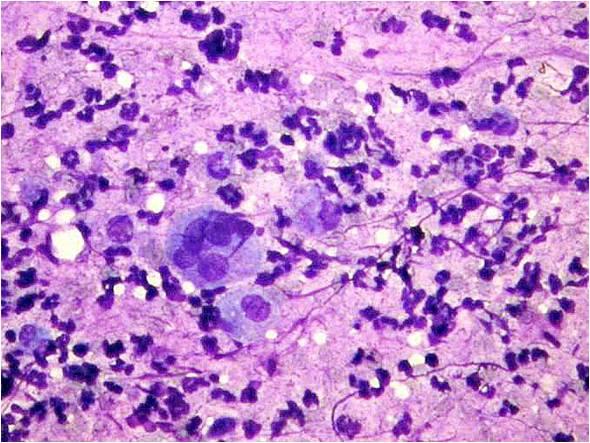
Acute sialoadenitis
The gland appears swollen and larger. The puncture is painful. A purulent necrotic material is aspirated, containing a few acinic and ductal cells. There are acute inflammatory cells (polymorphs), histiocytes and plasma cells. The acinic and ductal elements are vulnerable, many naked nuclei are also found. Multinucleated histiocytic giant cells are also usually present. The severe acute purulent parotitis in elderly patients is sign of a life threatening general status!
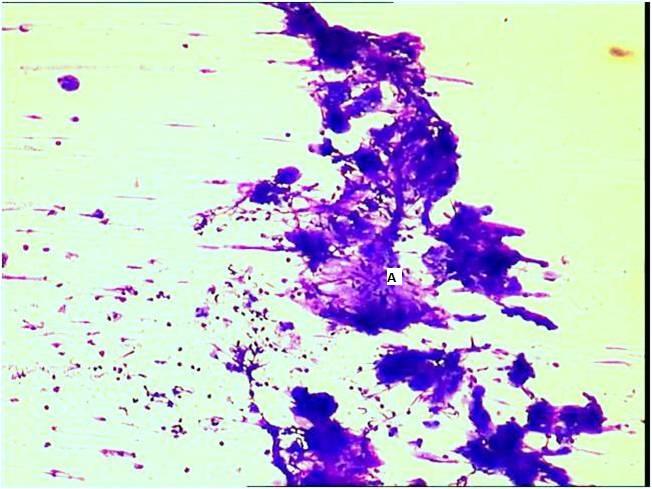
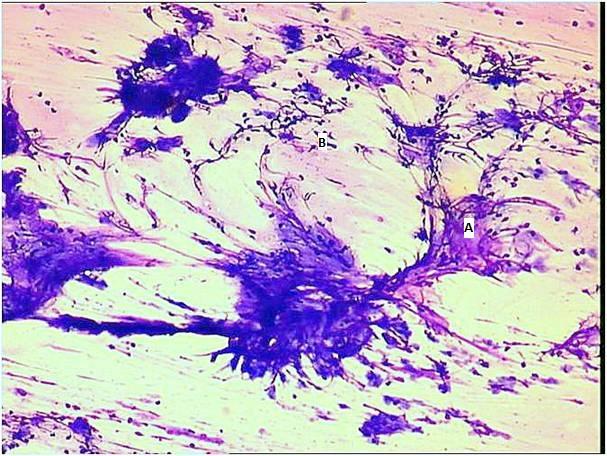
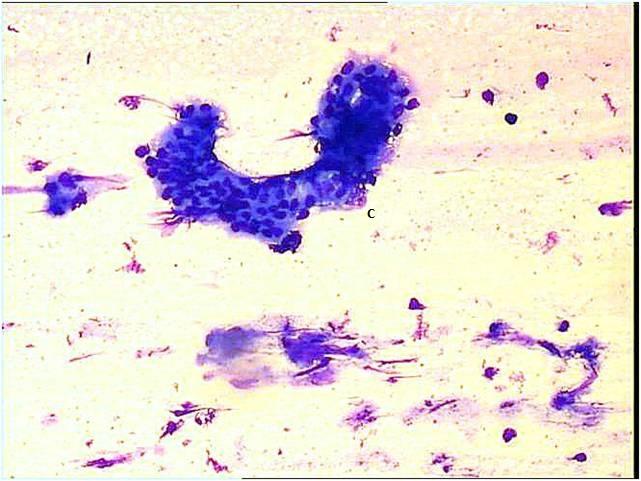
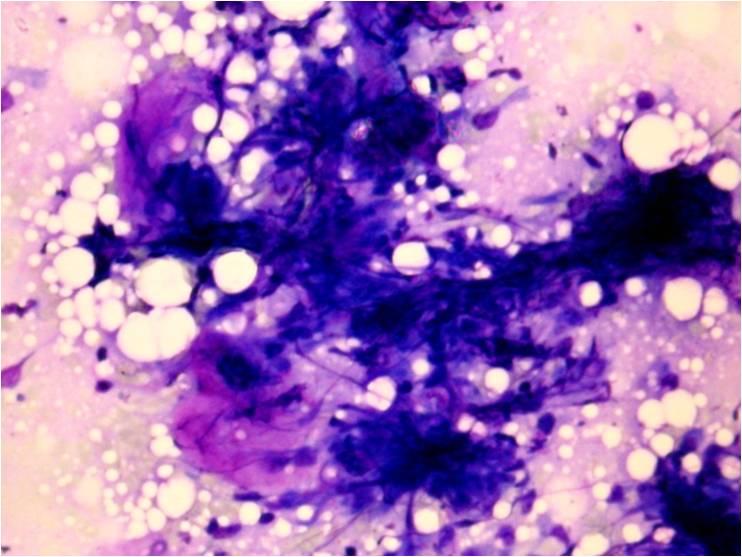
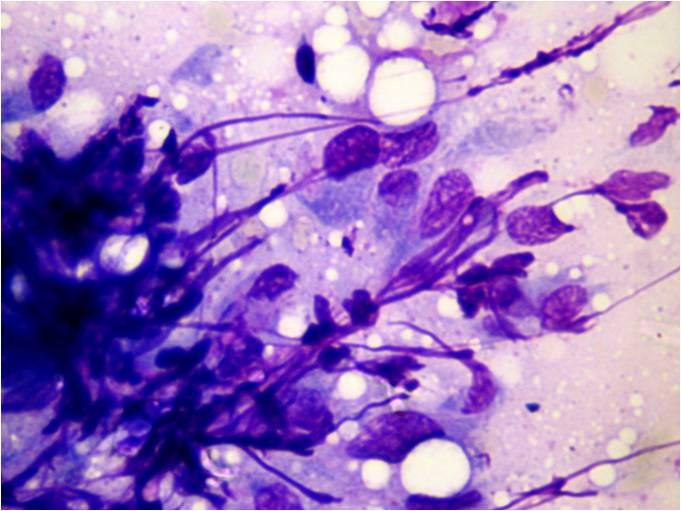
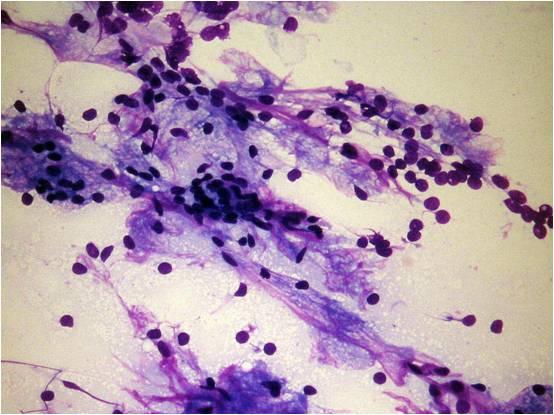
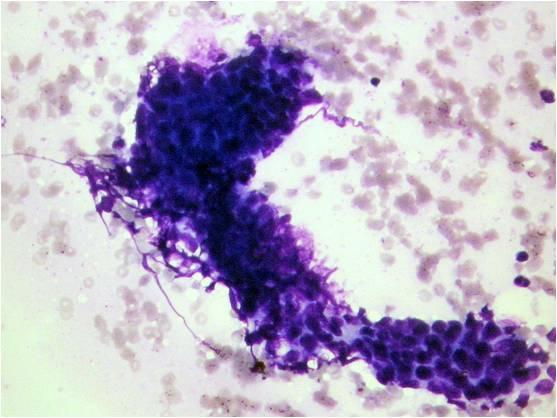
Chronic sialoadenitis
There are chronic inflammatory cells, usually in a dirty background of saliva. The acinic cells are extremely vulnerable, sometimes having larger cytoplasm. There are many naked nuclei in the background which represent probably the nuclei of the damaged acinic cells. The myoepithelial cells are arranged in sheets, there is a lympho-plasmacytic background. The ductal cells show proliferation. Just the presence of lympho-plasmocytes in a parotid aspirate is not sign of chronic inflammation: since there are many lymph nodes in the parotid gland, if only lymphocytes and plasma cells are found without the above alterations of the epithelial elements, it is more likely to be an aspiration of an intraglandular lymph node than a chronic sialoadenitis!
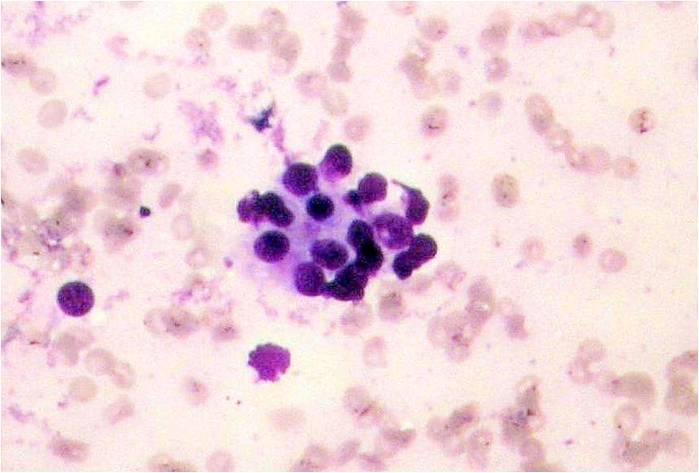
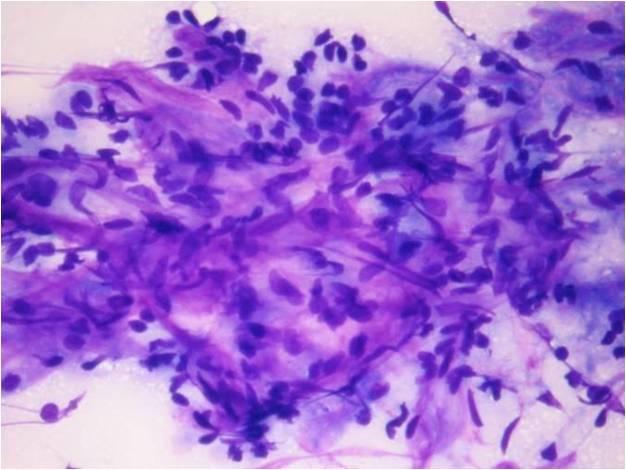
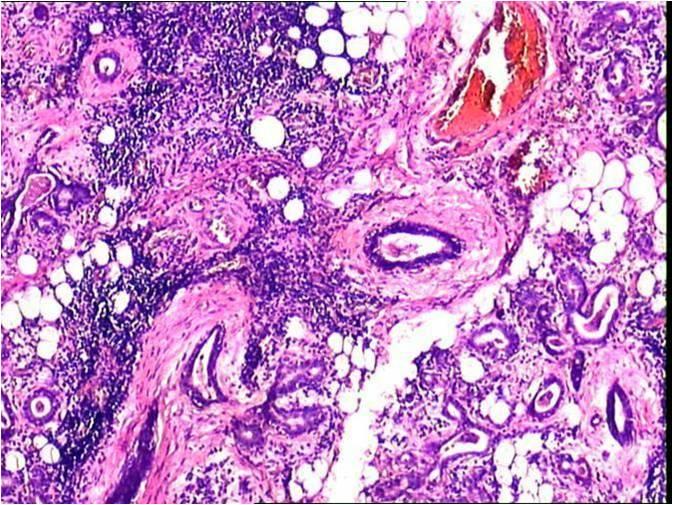
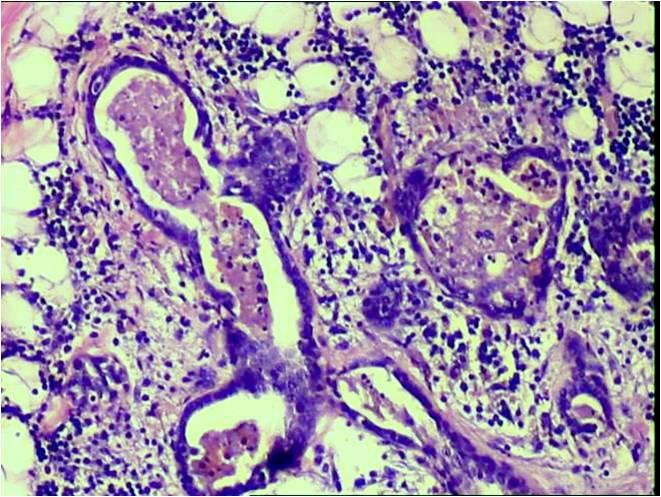
Chronic sclerosing sialoadenitis (Küttner tumor)
This lesion involves most often the submandibular gland, sometimes the parotid gland. Destructed cellular elements of the salivary gland in a background of dirty saliva are seen. It is almost always accompanied by squamous metaplasia and nonmalignant atypical squamous cell changes mimicking well differentiated squamous cell carcinoma. . The lesion there are some data supporting it may be related to other autoimmune sclerotic inflammatory processes, like retroperitoneal fibrosis, autoimmune pancreatitis or sclerosing cholangitis. In this background it is probably the so called IgG4 related disease-group.