This content is also available in:
![]() Español
Español ![]() Português
Português ![]() Čeština
Čeština ![]() Magyar
Magyar ![]() Polski
Polski ![]() Türkçe
Türkçe
The head and neck region shows the presence of many organs, many different kinds of tissues, many different cell types in each organ and tissue.
What do we mean by ‘head and neck’ tumors or head and neck pathology/cytopathology?
- In general: all pathology/cytopathology lesions or tumors of the head and neck region.
- In particular: nasal, paranasal, nasopharyngeal, hypopharyngeal, laryngo-tracheal, oral cavity, oropharyngeal, salivary glands related, odontogenic, ear lesions (WHO 2005).
- In a broader sense: any kinds of pathological changes which may occur on the above circumscribed anatomic area: see above, +: vascular tumors, lympoma, skin tumors, adnexal tumors, lachrymal gland lesions, thyroid/parathyroid lesions, dental pathology/cytopathology.
In the following Chapter we will discuss the most important lesions, diseases of the area with some anatomical exceptions: thyroid, parathyroid cytopathology belongs to another Chapter. It will be referred to the Chapter Cytopathology of the Lymph Nodes in cases where the primary diagnostic tool may be cytopathology in case of head and neck lymph nodes. The most common lymph node lesions however will be mentioned here: e.g. metastatic lesions, etc. Detailed lymph node cytology is not part of this Chapter. Hence the title of the course is: Cytopathology of the head and neck with special emphasis on salivary gland Cytopathology
What is characteristic in tumor pathology of the head and neck?
- The anatomical region
- There are significant geographical characteristics of some of these lesions (nasopharyngeal carcinoma)
- Environmental influence is important
- Viruses may be involved in the development of cancer (HPV, EBV)
- Distant metastases are rare, local complications are severe
- typical anatomical site for distant lymph node metastases from whatever region of the human body
Main diagnostic questions

- What kind of tissue was aspirated?
Most of the punctures are US guided (there are however lesions which are more easily punctured without!). The US image gives you hints concerning the organ; this should be reassured by microscopy. In case the sampling is performed by the cytopathologist the answer usually is simple. In case of transported smears we always need to be informed of all the important clinical and US data, symptoms and the way of sampling. (Any kinds of cells may be present in the smear which have been located on the way of the needle track)
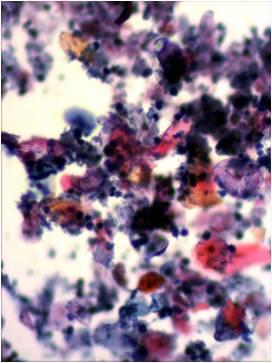
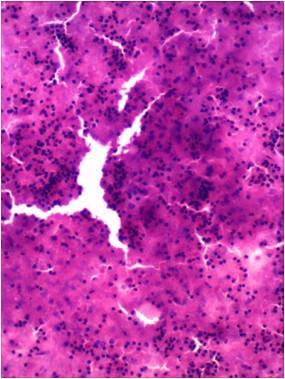
- What do the general cellular features of the smear tell us? Is it a benign or malignant lesion?
The head and neck region is controversial: yellowish looking thick cystic fluid may equally represent a squamous (lateral) cyst or a colliquated necrotic squamous cell carcinoma or just simply purulent content of an abscess.
Malignancies can be either primary or metastatic. The classical signs of malignancy may have different significance in this region: Cellular pleomorphism which is usually sign of malignant growth is characteristic in benign mixed salivary gland tumors, whereas a slightly atypical homogeneous cell population may be characteristic of acinic cell cancer or even adenoid cystic carcinoma without other morphology signs of malignancy.