This content is also available in:
![]() Español
Español ![]() Português
Português ![]() Čeština
Čeština ![]() Magyar
Magyar ![]() Polski
Polski ![]() Türkçe
Türkçe
Exfoliative cytology of oral cavity
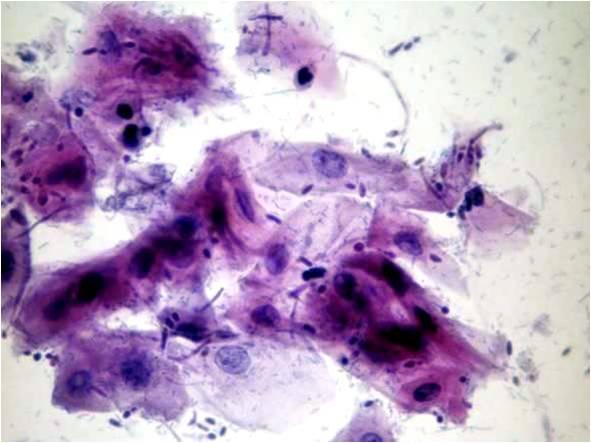
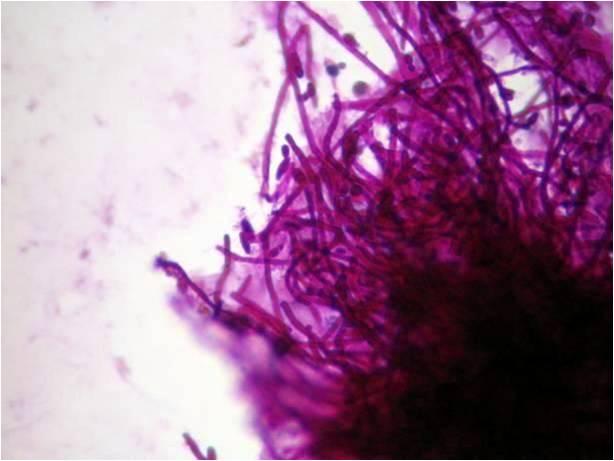
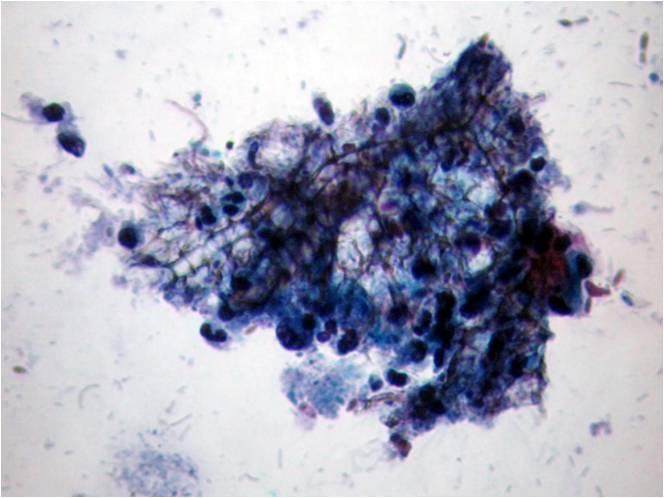
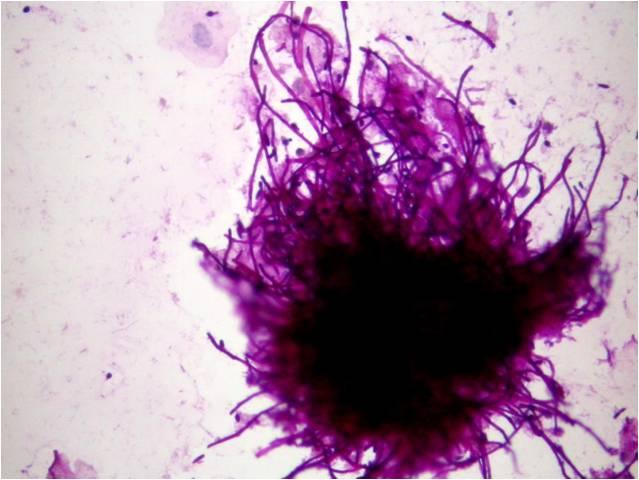
Infections without inflammation (AIDS): cells of the superficial squamous epithelium in a dirty background which contains many different types of infectious agents, such as bacteria, fungi, etc. The complete absence of inflammatory cells is diagnostic in these cases! The differential diagnostics is certainly any kinds of immunosuppressed status (anti-cancer treatment, treatment in autoimmune diseases, etc.)
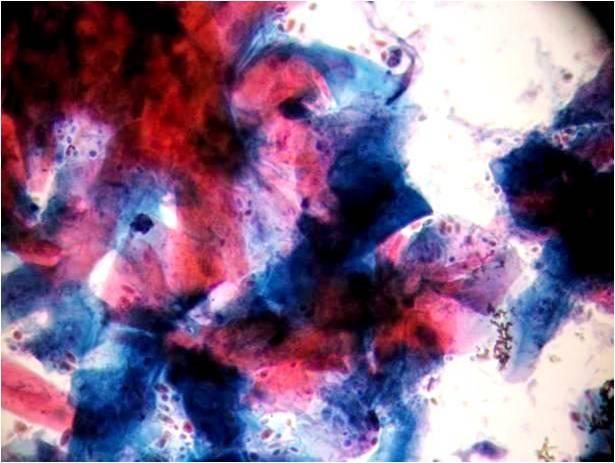
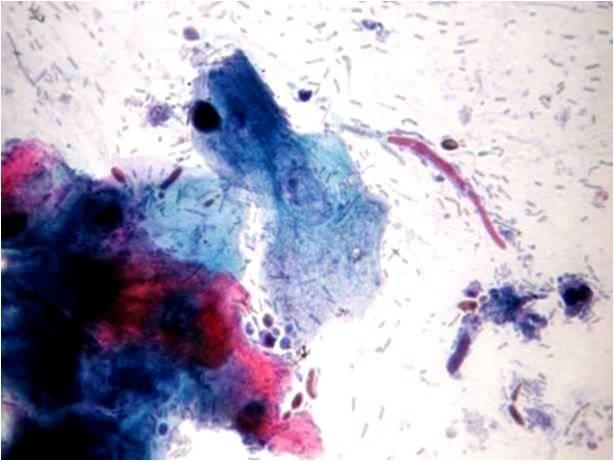

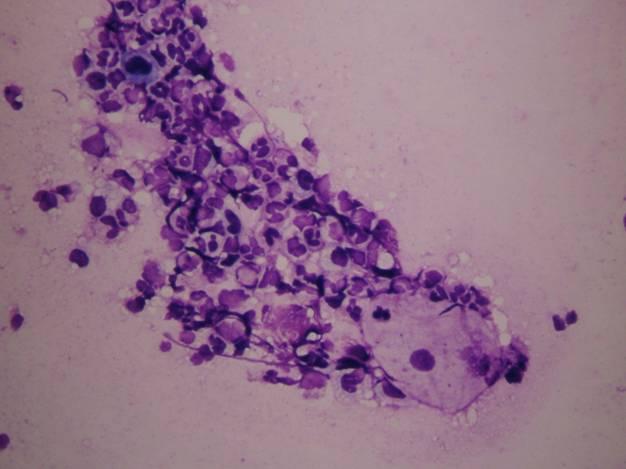
Squamous cell carcinoma of the oral mucosa shows very high incidence in Melanesia, France, Hungary, Western Europe. It can be sampled using cytobrush, or oral washing fluid can be prepared by using any kinds of LB techniques. The morphology of the cells is exactly the same as in the uterine cervical squamous cell carcinoma. Probably the best method for staining in this case is Papanicolaou stain. Important fact is that the eventual connection to HPV infection should always be traced (p16ink staining, Ki67, HPV molecular diagnostics). Those HPV related benign or malignant epithelial lesions need to be treated less aggressively.
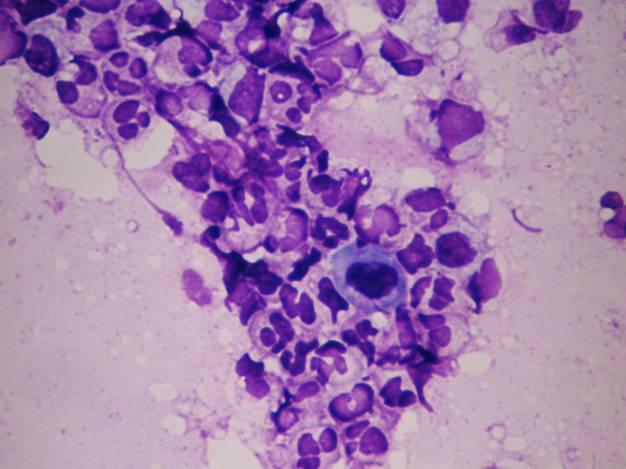
Pemphigus vulgaris and its variants show the presence of bullous lesions. The content of the vesicula or bulla can be smeared using cytobrush technique. One of the earliest cytology diagnoses was that of the recognition of the Tzanck cells: they are large, acantolithic cells with large pale nucleus and sometimes large nucleolus. The background shows features of acute inflammation. The site of the first diagnosis of pemphigus vulgaris often is the oral cavity!

Palpable lesions of the tongue are very rare. They can be aspirated. Squamous cell carcinoma is superficial, whereas non epithelial (usually benign) tumors are deep lesions. The well-known Abrikoszov tumor can also be detected on aspirates based upon the characteristic more or less monomorphic granular non-epithelial cells.