This content is also available in:
![]() English
English ![]() Português
Português ![]() Čeština
Čeština ![]() Română
Română ![]() Türkçe
Türkçe
Cellule squamose atipiche di incerto significato (ASC-US)
- ASC-US (o alterazioni borderline nelle cellule squamose) al limite con LSIL può essere largamente risolto dal triage con HPV.
- La negatività per HPV escluderebbe le alterazioni minori nelle cellule squamose mature o intermedie senza coilocitosi (l’unica caratteristica diagnostica di una infezione da HPV)
- Un lieve ingrandimento nucleare e l’ipercromasia sono frequenti nelle donne in perimenopausa ma vengono refertati ugualmente come ASC-US.
- Cambiamenti minori causati da HPV, confermati al triage per HPV ad alto rischio, dovrebbero essere approfonditi con ulteriori esami se persistono come LSIL.
How to avoid unnecessary ASC-US reports
|
Cellule squamose atipiche, non si può escludere HSIL (ASC-H)
ASC-H viene utilizzato quando le carateristiche di HSIL non sono certe dopo aver cosiderato tutte le condizioni precedentemente descritte come falsi positivi e falsi negativi. E’ facile vedere come le figure 10.1 (b), 10.2 (a-b), 10.3 (a-c) e 10.6 (b e c) potrebbero essere refertate come ASC-H se quelle viste fossero state rappresentative delle cellule più anormali del vetrino. A dire il vero, alcuni di quei casi sono stati refertati come ASC-H. Allo stesso modo, con alcuni esempi di metaplasia squamosa immatura e metaplasia tubarica, dovrebbe essere difficile evitare una diagnosi di ASC-US come nella figura 10.7 (c e d).
Cellule ghiandolari atipiche (AGC)
AGC ha due problemi:
- Distinguere i processi benigni o metaplastici dalle cellule ghiandolari neoplastiche come nella figura 10.7 (a-c)
- Distinguere le cellule ghiandolari reattive da HSIL come nella figura 10.5 (e). Le caratteristiche tipiche di AIS devono essere distinte dalle celule endocervicali reattive, metaplasia tubarica e TEM facendo attenzione al pattern della cromatina, all’architettura a palizzata e all’assenza di cellule stromali o di cilia.
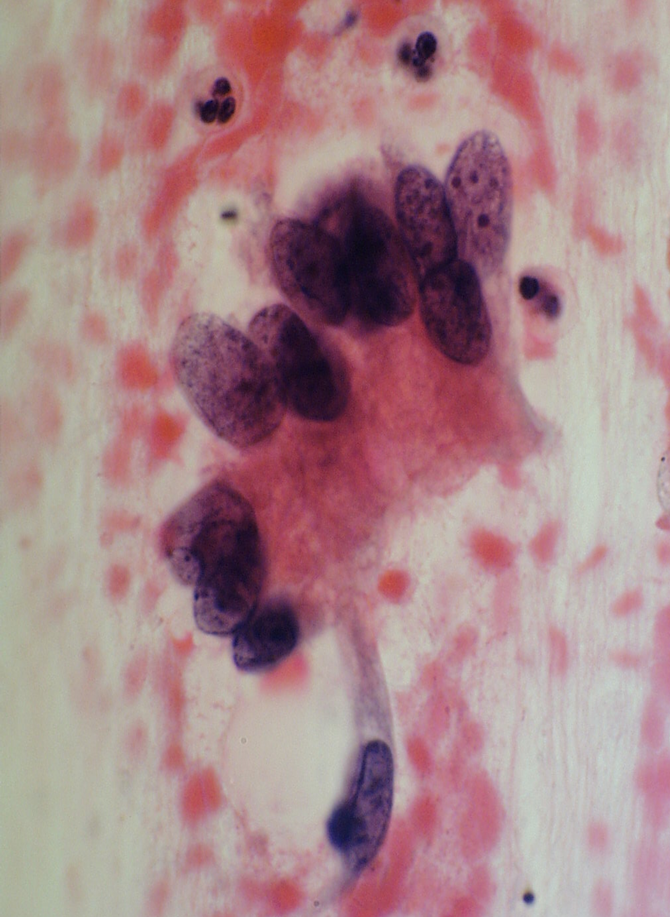
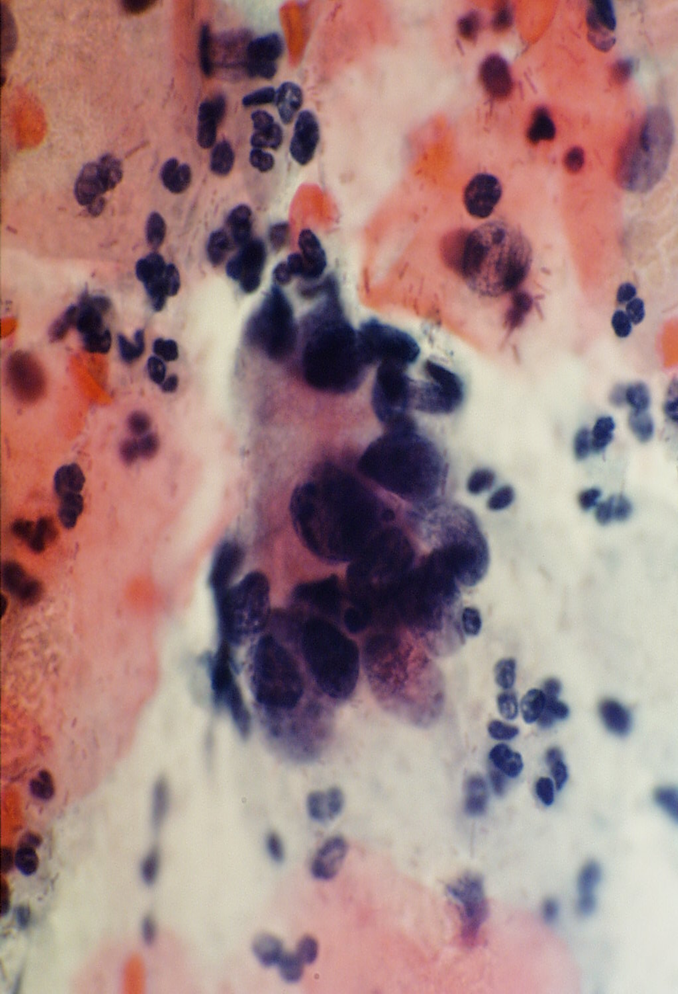
Figure 10.11 Atypical glandular cells favour neoplasia

How to avoid unnecessary ASC-H and AGL reports
|
Learning points from Chapter 10
|