This content is also available in:
![]() Español
Español ![]() Čeština
Čeština ![]() Magyar
Magyar ![]() Polski
Polski
This is an autoimmune disease in which the parenchima is virtually replaced by a lymphoid infiltrate with germinal centers, sometimes with a prominent fibrosis in longstanding disease. Several autoantibodies are identified in affected patients, such as antibodies against thyroid microsomal antigens and against TSH receptors.
The gland is usually enlarged, painless, with or without nodularity. Some patients may be hyperthyroid or euthyroid at the begininning, but later most of them become hypothyroid.
Cytologic diagnostic features
- mixed population of lymphocytes
- tingible-body macrophages
- lymphohistiocytic aggregates
- Hürthle cells
The aspirate is usually cellular, prodominantly composed of lymphocytes (small lymphocytes, centroblasts and centrocytes), which may be intraepithelial, and plasmacells. Lymphohistiocytic aggregates, with tingible-body macrophages, are also present. Occasional clusters of thyrocytes may be observed, usually with degenerative changes and oncocytic morphology: they have abundant, eosinophilic granular cytoplasm and enlarged nuclei (Hürtle cell metaplasia). Multinucleated giant cells can be present too. Colloid is usually absent or scanty.
The cytologic diagnosis is usually straightforward and needs a confirmation by identifying serum autoantibodies.
Differential diagnosis
- Non-Hodgkin lymphoma
- Hürthle cells neoplasm
The prevalence of lymphoma is increased in patients with Hashimoto`s thyroiditis; lymphoma usually consists of a uniform population of atypical lymphoid cells. Hürthle cell tumors have to be differentiated from hyperplastic Hürthle cell nodules, which may occur in Hashimoto`s thyroiditis; the cells of tumors usually have prominent nucleoli and are less cohesive than in thyroiditis.
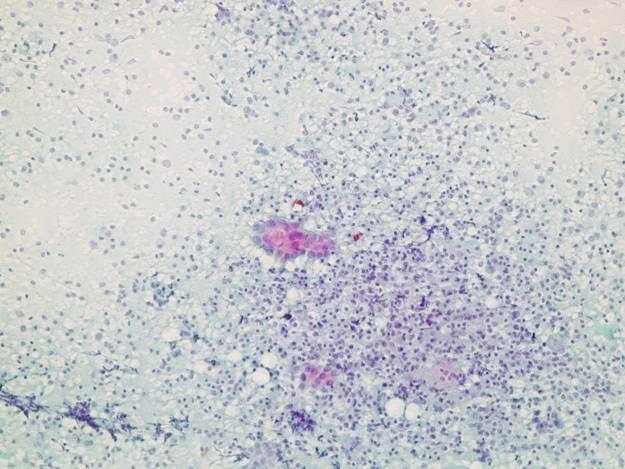


Follicular cells surrounded by lymphocytes.
A group of epithelial cells surrounded and partially infiltrated by lymphocytes. Note the variability of nuclear size and granular chromatin. Often individual cells may cause problem at high power. When clear cut nuclear pseudoinclusions are seen the suspicion of a papillary carcinoma in a background of chronic thyroiditis should be raised.
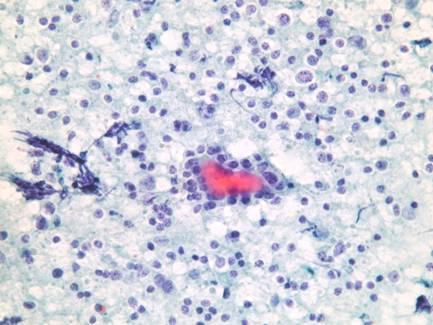
A follicle infiltrated by lymphocytes.
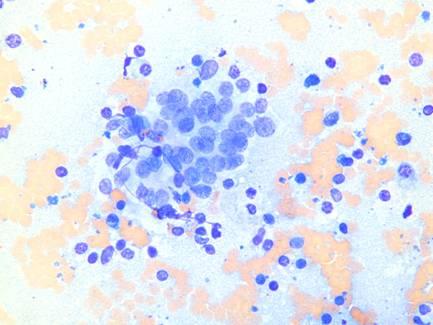
A group of slightly crowded epithelial cells in a follicular arrangement, infiltrated by lymphocytes. Note the nuclear streaking.
