This content is also available in:
![]() Español
Español ![]() Čeština
Čeština ![]() Magyar
Magyar ![]() Polski
Polski
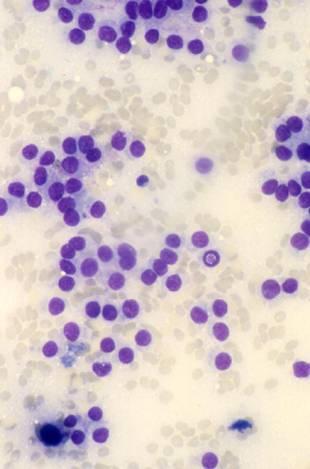
Cytologic diagnostic features:
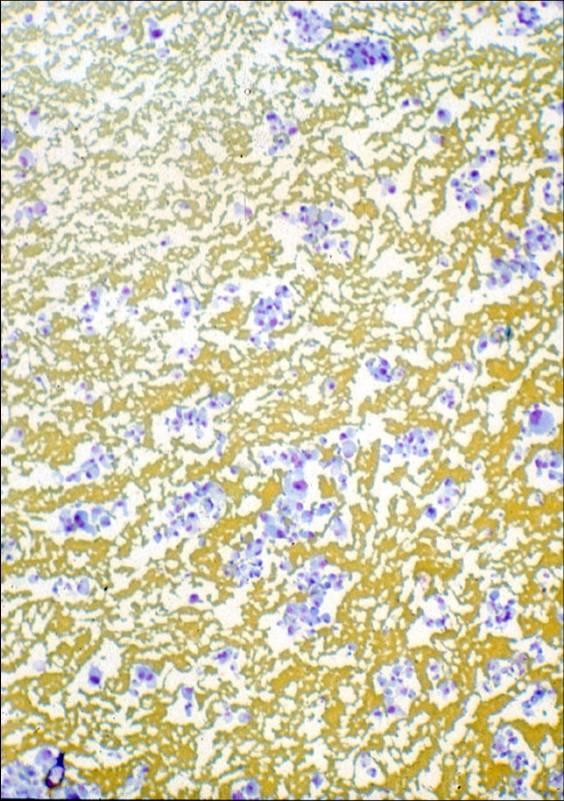
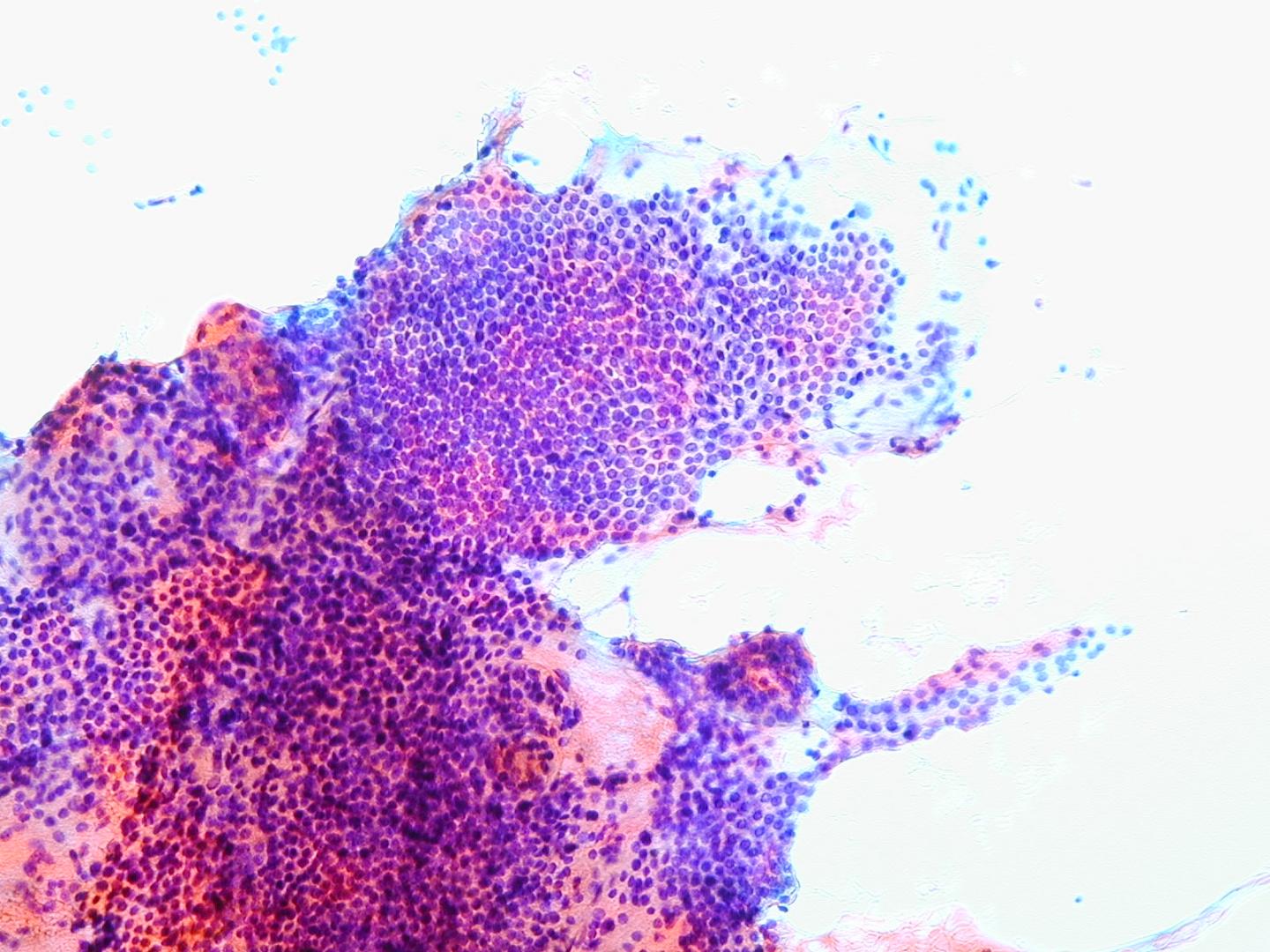
- high cellularity
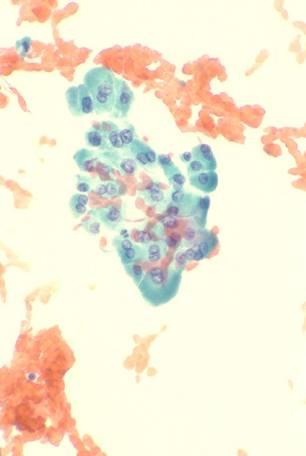
- predominantly microfollicular or trabecular pattern
- crowded, overlapping cells
- cellular alterations (mild atypia, an uniform enlargement)
- scanty or absent colloid
Several of all of these features should be present to diagnose a follicular lesion as ‘cytologically suspicious’. Marked nuclear atypia is uncommon, and so are mitosis. Macrophages are absent. Bare nuclei are usually few or absent.
No single criterion is sufficient to distinguish benign from suspicious nodules. The presence of several features increases the likelihood of malignancy, and that is the case for which a diagnosis of cytologically suspicious follicular nodule should be made. All the aspirates that are composed of a pure Hürthle cell population are suspicious by definition.
The differential diagnosis includes other thyroid neoplasms. Nuclear grooves and pseudoinclusions may be focally present in some follicular adenomas and carcinomas. If focal, they should not lead to a diagnosis of papillary carcinoma but will define the lesion as supicious. In the so-called hyalinizing trabecular adenoma, smears show oval or spindle cells in aggregates or isolated. Clues to the correct diagnosis are a whorling, parallel array of the cells, an amorphous hyaline material and a perinucleolar clear zone. The clear cell variant of follicular carcinoma may be confused with some parathyroid tumors or metastatic renal cell carcinoma, but cells are usually positive to immunostaining for thyroglobulin.
Only about 30-40% of cases diagnosed as ‘suspicious follicular nodules’ prove to be malignant. Among these, only 50-75% are follicular carcinomas, while the others prove to be follicular variants of papillary carcinoma.
The Thy classification has been devised clinically to separate lesions at higher risk of malignancy from the ones with a low risk. In both cases the surgeon will offer excision of the nodule but will point out that in the former (Th4 category) the risk is approximately 80% while in the latter (Th3) is approximately 20%.
In patients with a diagnosis of ‘suspicious follicular nodule’ a lobectomy is usually performed; if a carcinoma is diagnosed by the hystological examination, a complete thyroidectomy is recommended.
Adjunctive techniques have been advocated to discriminate between benign and suspicious follicular lesions. Morphology and image analysis proved not to be sufficiently accurate for clinical purposes. DNA measurements by flow cytometry is also not useful; in fact, aneuploidy does not guarantee that a tumor is malignant. Immunocytochemistry for MIB-1 is not of great value, since the proliferative activity in adenomas and carcinomas can be similar. Immunocytochemistry for galectin-3 appears to be promising, since most carcinomas are positive and most adenomas are negative, but is not specific or sensitive enough in clinical practice. The distinction could be made also with genetic markers: the translocation t(2;3) is a specific marker of follicular carcinoma.

Follicular carcinoma
It represents the second most common thyroid cancer (5-15% of thyroid malignancies). It is usually a solitary nodule but, differently from follicular adenoma, it shows capsular infiltration and vascular invasion. Follicular carcinoma is usually divided into two histological subtypes: a minimally invasive with a very good prognosis and a widely invasive with poor prognosis, which tends to metastatize to lung and bones.
The cells of follicular carcinoma never show the nuclear features of papillary carcinoma, which helps to distinguish follicular carcinoma from the follicular variant of papillary carcinoma.
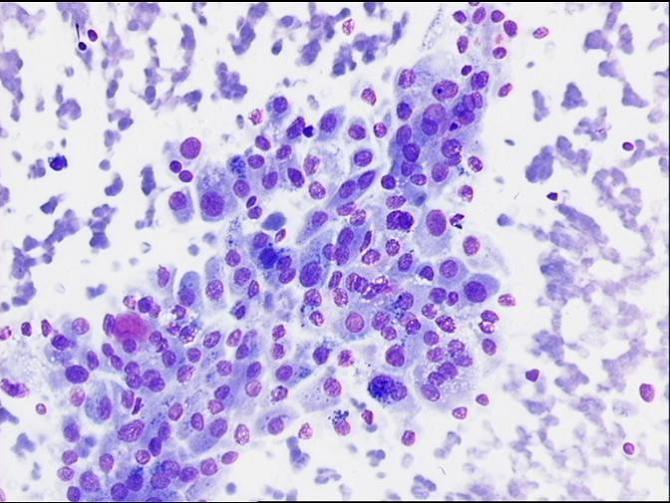
Hürthle cell tumours
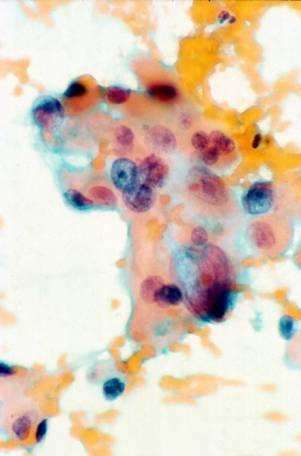
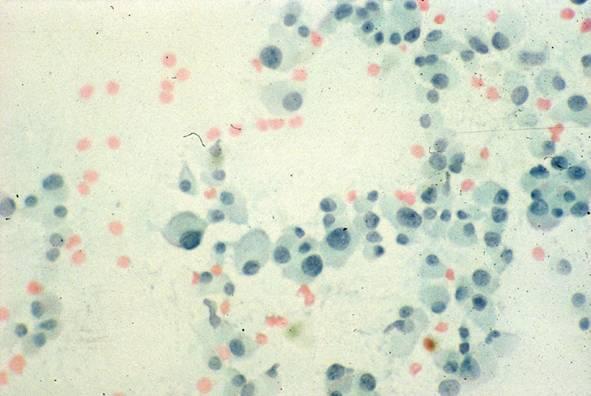
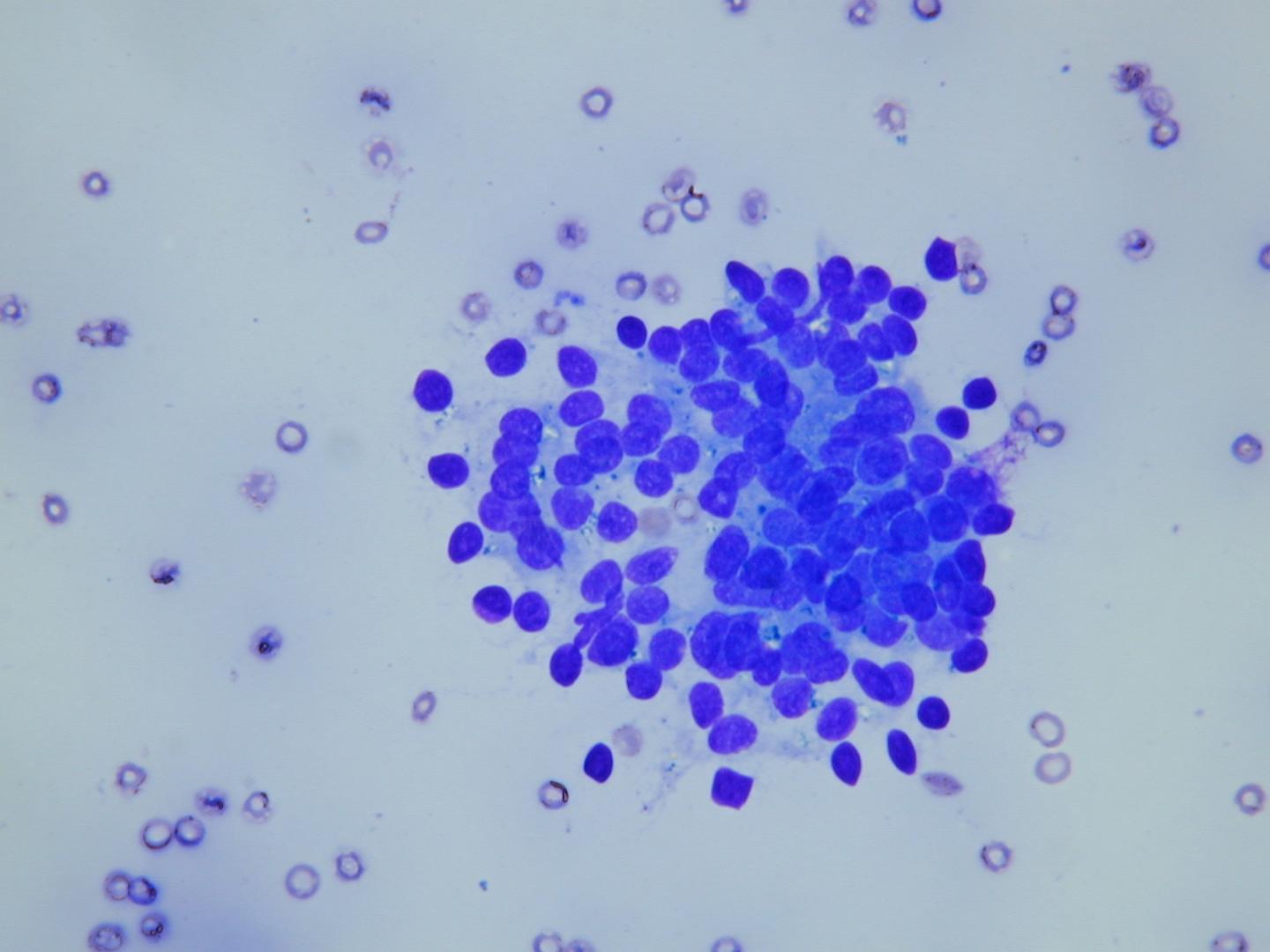
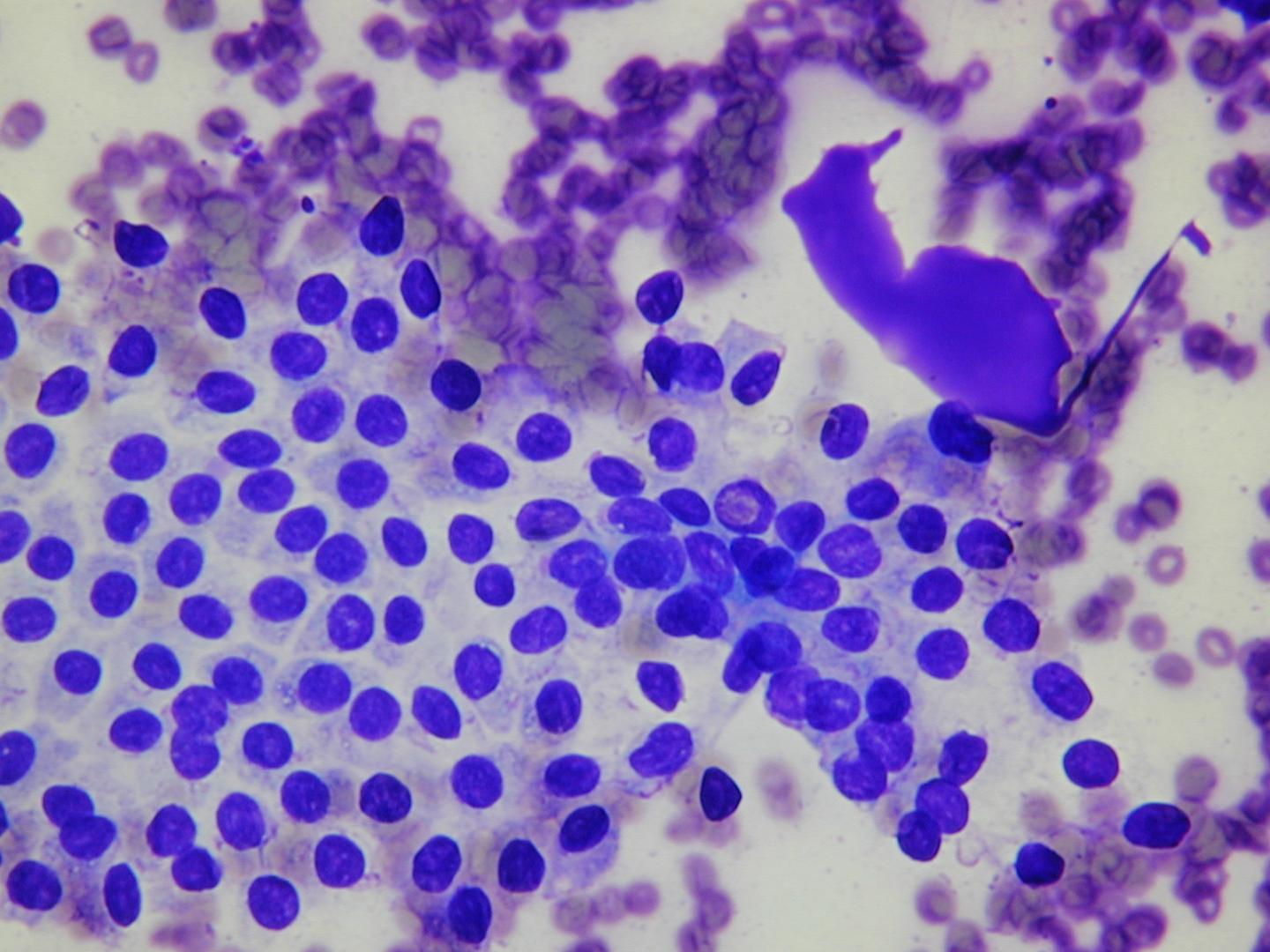
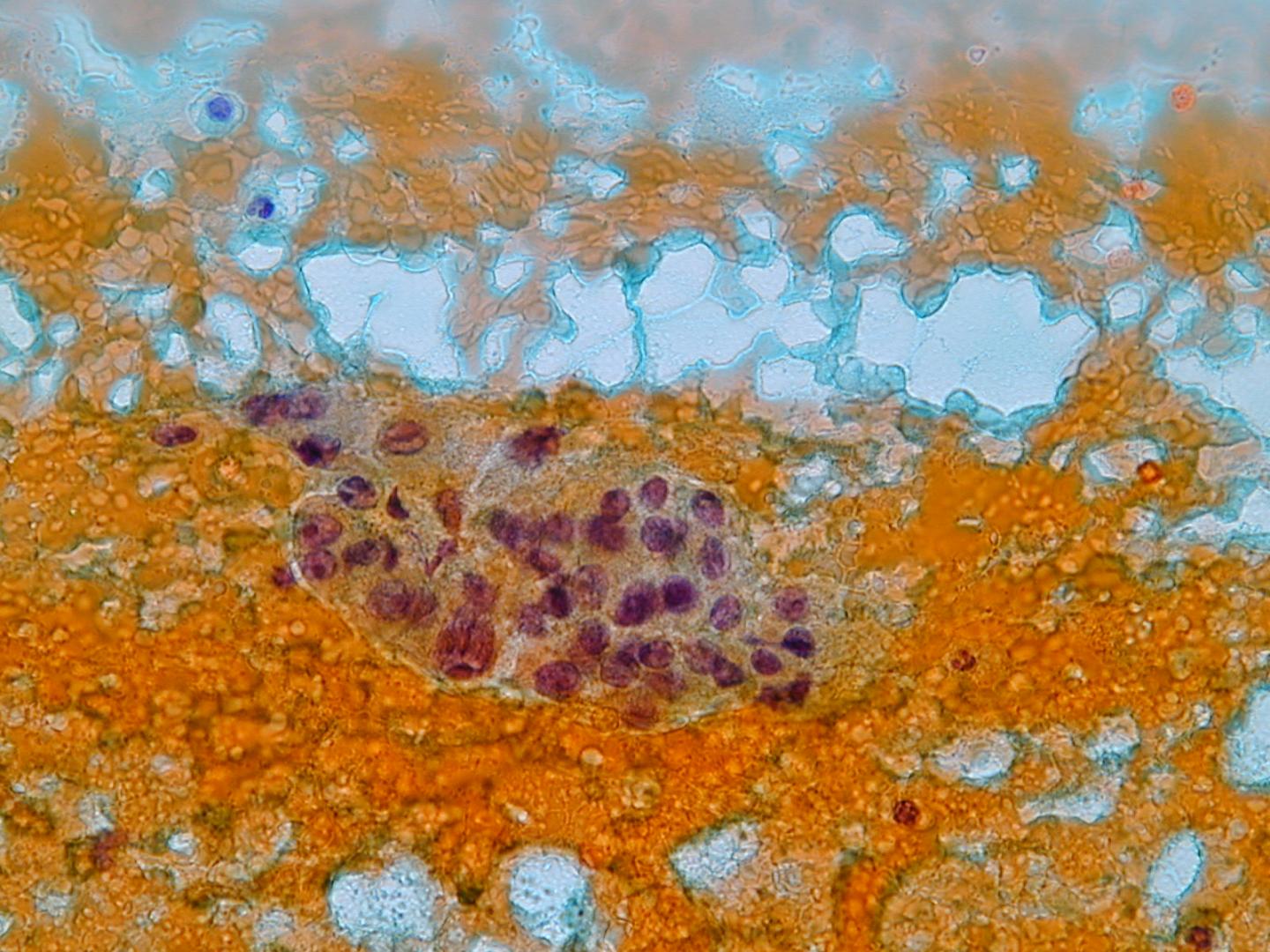
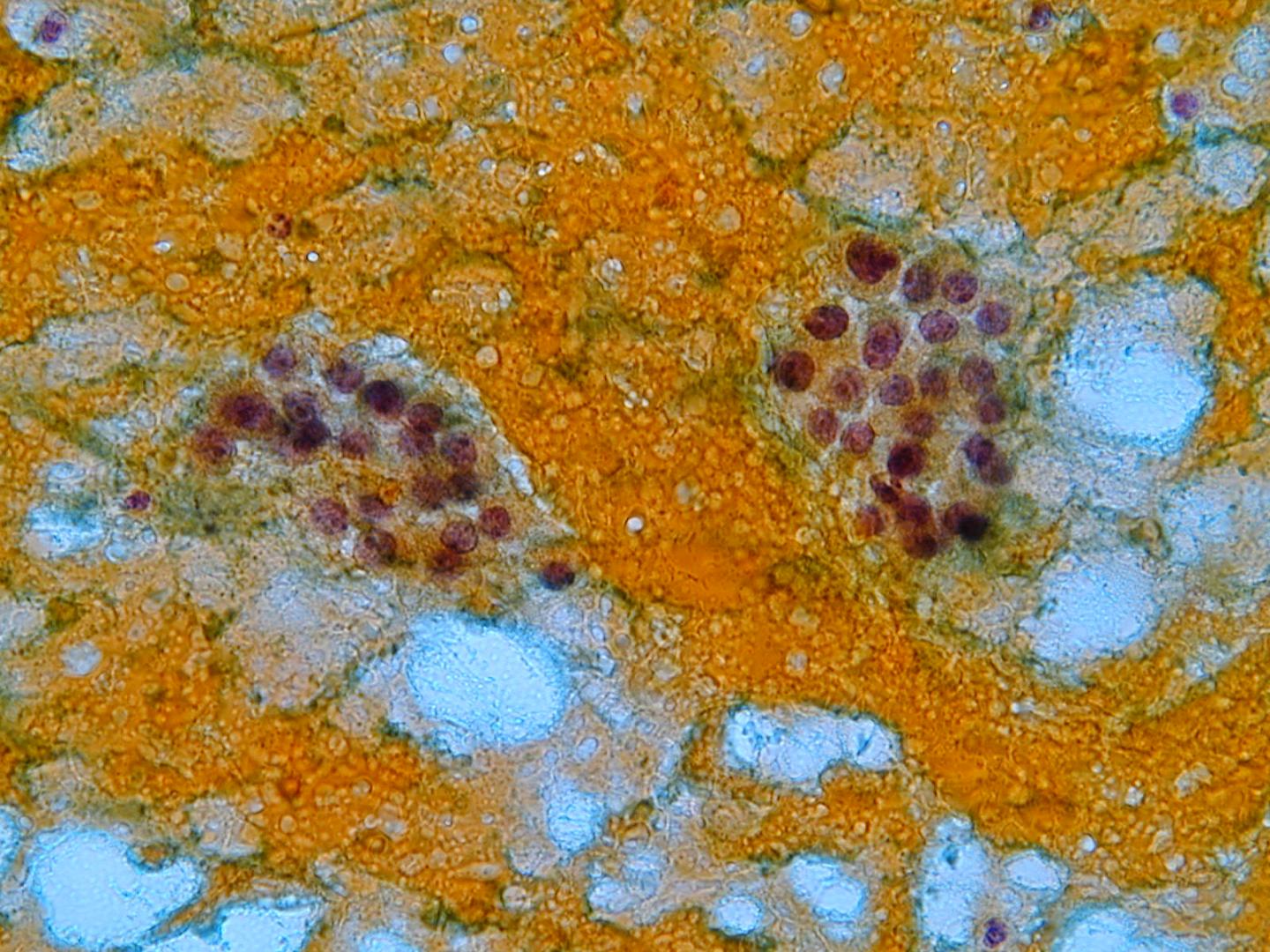
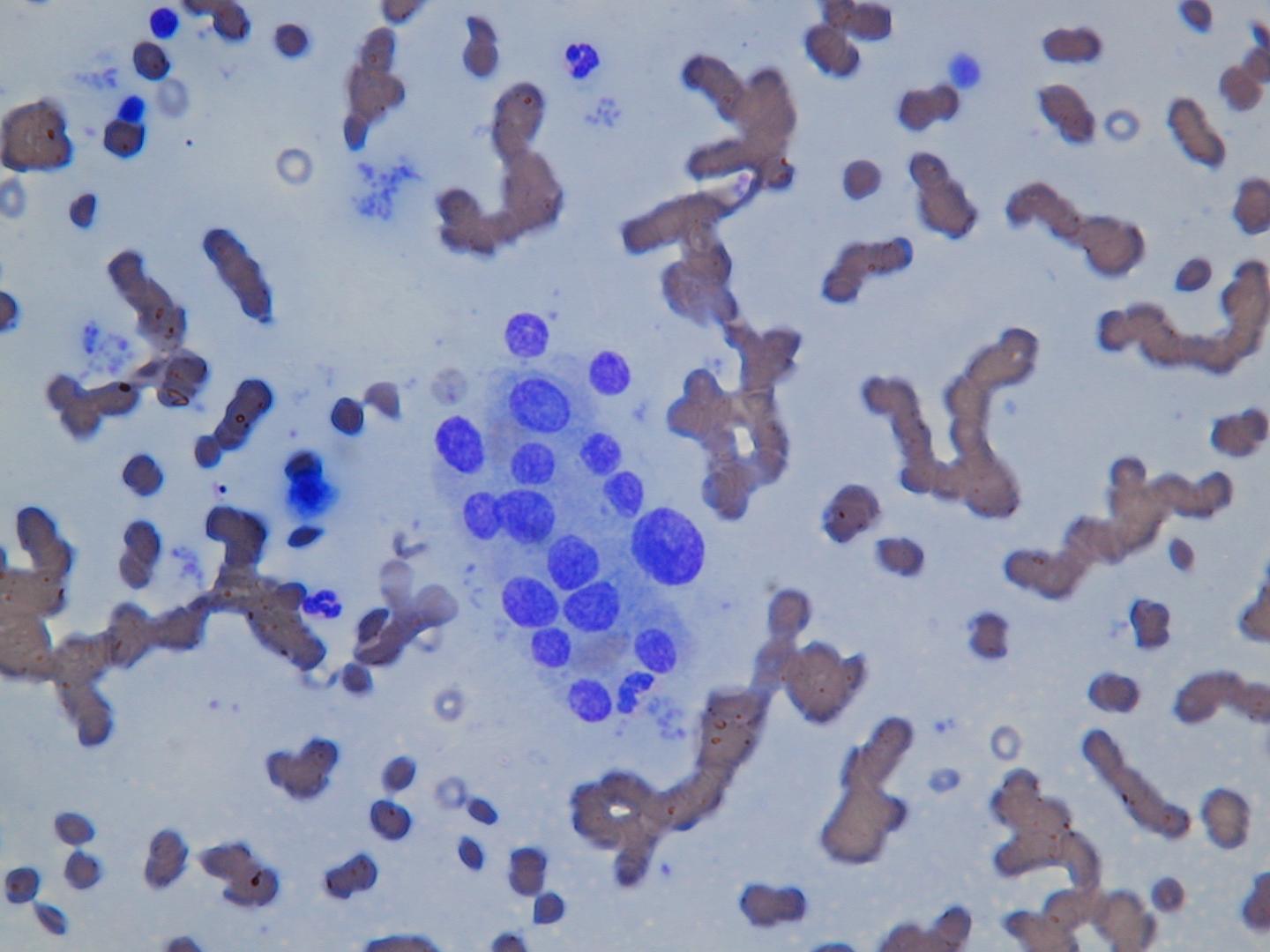
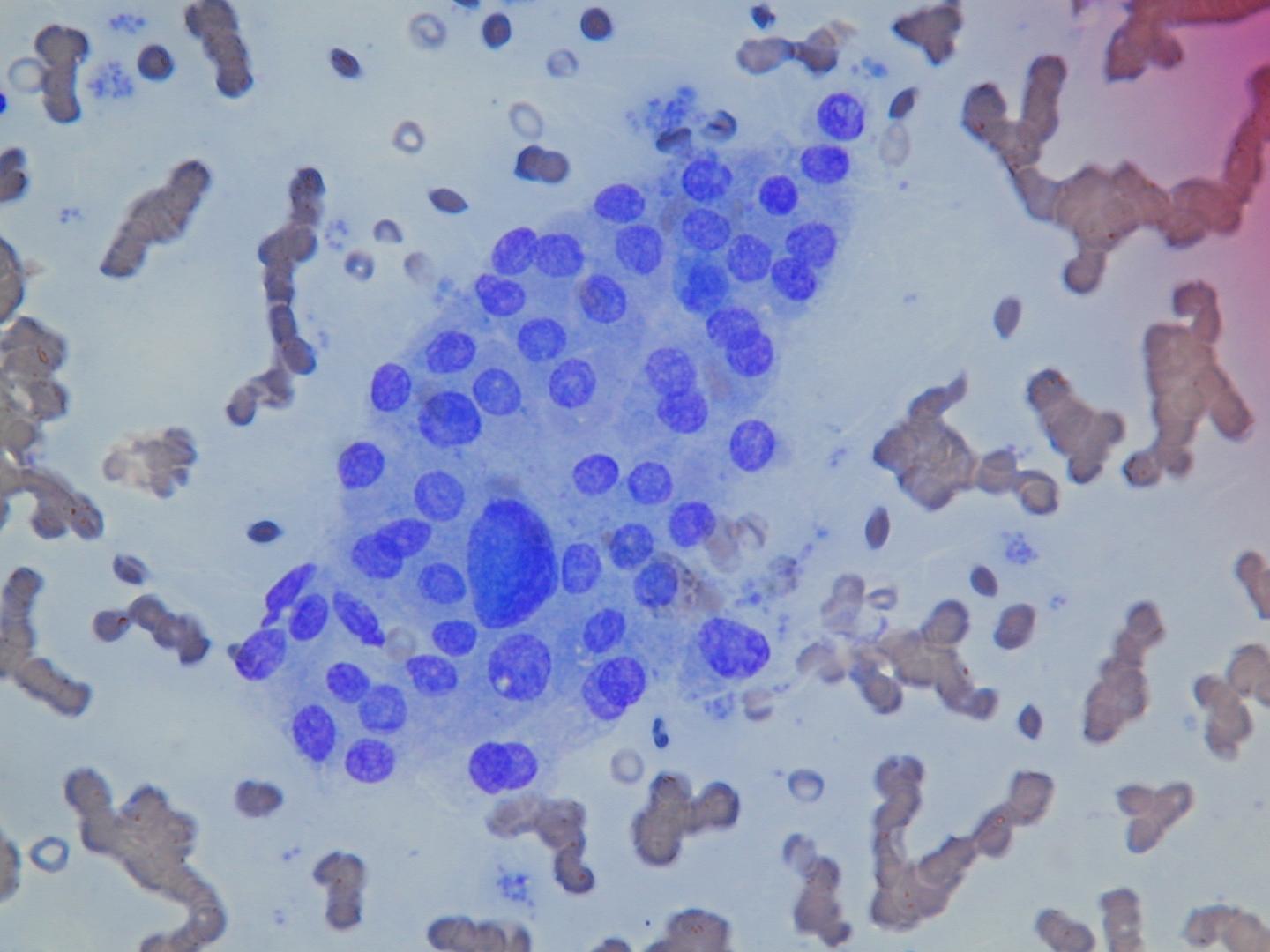
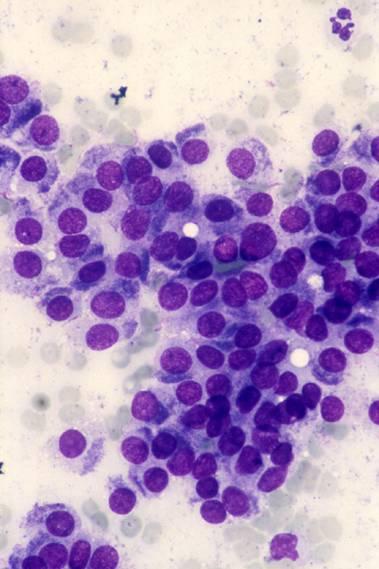
Hürthle cells (oncocytes) are altered follicular cells which are very rich in mitochondria. In cytologic smears, they appear as polygonal cells, with large and finely granular cytoplasm, purple with MGG staining and orangeophilic with Papanicolaou staining. They can be binucleated, nuclei are enlarged and their size may be variable, often with prominent nucleoli.
Hürthle cells are common in Hashimoto`s thyroiditis and in multinodular goiter, where they can also form macroscopic nodules. Benign Hürthle cells are usually cohesive and do not have prominent nucleoli; a slight or moderate pleomorphism can sometimes be observed. In Hashimoto`s thyroiditis, they are admixed with numerous lymphoid cells. In nodular goiter, they are admixed with macrophages and colloid.
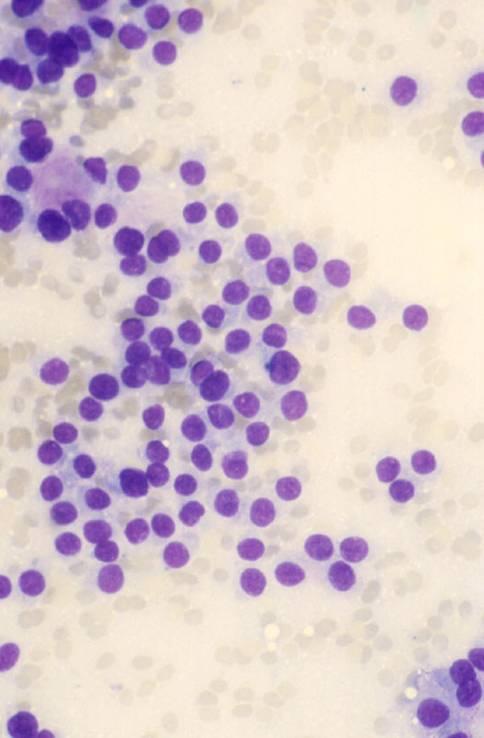
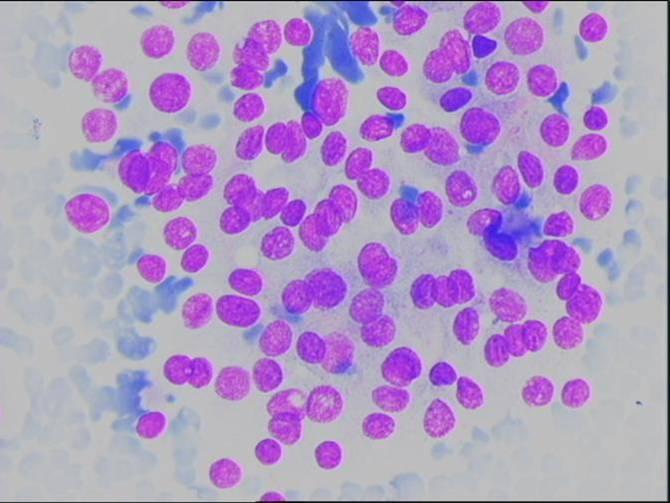
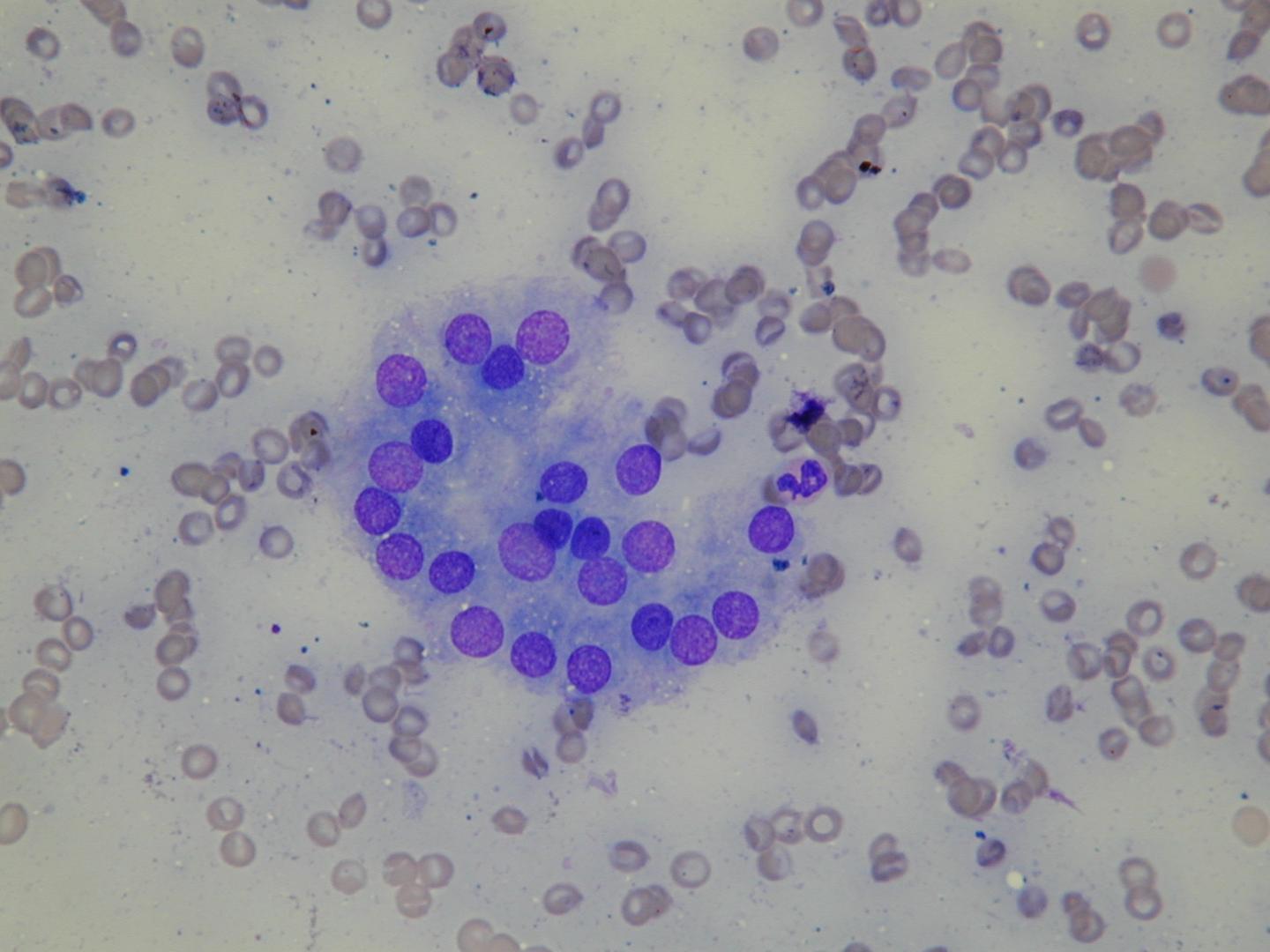
In Hürthle cell tumors the aspirate is generally composed of a pure Hürthle cell population. The cells are usually discohesive, but aggregates can be seen. Vesicular nuclei and prominent nucleoli are often present. In the case of a Hürthle cell neoplasm, normal follicular cells are usually absent and so are abundant lymphocytes; colloid may be present.
The differential diagnosis includes some variants of papillary carcinoma, such as tall/pink cell and oncocytic. Moreover, rare Hürthle cell tumors show papillary architecture (oncocytic papillary neoplasm). Variants of papillary carcinoma can be excluded by the absence of the characteristic nuclear features in almost all cases. Metastatic renal cell carcinomas may mimic Hürthle cell neoplasms, but immunocytochemistry for thyroid transcription factor 1 (TTF-1), which is positive in follicular and Hürthle cells, is negative in the cells of renal cell carcinoma. Medullary thyroid carcinoma shows a dispersed cell pattern and a cytologic appearance that can mimic a Hürthle cells neoplasm. Prominent nucleoli are usually absent in medullary carcinoma. With MGG stains, the granules of Hürthle cells are blue, the ones of the cells of medullary carcinoma are red.