This content is also available in:
![]() Čeština
Čeština ![]() Türkçe
Türkçe
Normal lymph node histology
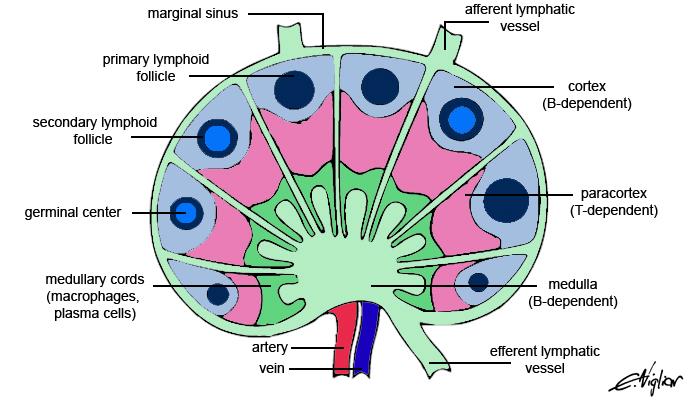
Lymph nodes are oval masses surrounded by a fibrous capsule and divided by septa. The internal areas are divided and supported by reticular fibers of variable thickness. The capsule is reached by afferent lymphatic ducts that carry the lymph flowing in the sub capsular sinus toward the peripheral sinus. Lymph nodes are anatomically and functionally composed of three distinct areas: the cortex, paracortex and medulla. The cortex is a B-cell dependent area containing primary and secondary follicles. Primary follicles are spherical aggregates of small lymphocytes. Secondary follicles are the site of antigen exposure, and of B lymphocytes recruitment and rearrangement; they are formed by a pale germinal centre encircled by a dark, thick border of small B-lymphocytes. The paracortex surrounds the follicles and is interposed between the cortex and the medulla; it is a T-cell depending area, formed by small lymphocytes. The medulla is the place of the sinus where the lymph is conveyed toward efferent lymphatic ducts and is a B dependent area; the medulla contains macrophages, plasma cells and lymphocytes. Each of these areas, far from being static, can undergo changes according to different pathological conditions, and the smears may reflect the prevalence of the corresponding cell composition.
FNC evaluation
Look at the smear at low magnification: is the smear highly or poorly cellular? Is it monomorphous or polymorphous? aggregated or dispersed?
Identify 1) isolated cells, 2) lymphoid cells in the different stages of development and their numerical prevalence, 3) granulocytes and 4) histiocytes.
Look at cell groups: are there immature lymphoid cells? macrophage-lymphoid complexes? epithelioid cells? metastatic cells?
Identify the stroma and vascular structures.
Evaluate nuclear atypia, but be aware that most NHL cells are a clonal expansion of the corresponding non-lymphomatous cytotypes.
Compare cytological findings with ICC and/or FC, FISH and molecular data, if available, to confirm the clonality or identify specific translocations.
Cytotypes and their prevalence in different pathological entities
Mature lymphocytes have small and dark nuclei with coarse chromatin and a thin rim of cytoplasm. The B and T phenotype cannot be distinguished based on the cytological features, whereas enlarged nuclei and small cytoplasmic tales seem typical of T-lymphocytes. T-lymphocytes may be excessively numerous in lymphocyte-predominant HL or in T-rich B-NHL.
Plasma cells have eccentrically located nuclei with cartwheel chromatin and large, well defined cytoplasm with a pale rim in the paranuclear area. Plasma cells can be predominant in syphilis, lymphoplasmacytoid lymphoma and plasmacytoma.
Macrophages are large cells with wide cytoplasm, often engulfed with phagocyted cellular debris, and one or two eccentrically located nuclei. The latter can be round or oval pale with dusty chromatin and small or inconspicuous nucleoli. Macrophages are predominant in sinus histiocytosis, or intermingled among lymphoid cells in reactive hyperplasia, and may produce a starry sky pattern in lymphoblastic lymphoma (Burkitt lymphoma).
Epithelioid cells are large cells of monocytoid origin. These cells have one or two nuclei and wide ill-defined cytoplasm that is pinkish at the Diff Quik stain. Epithelioid cells may be isolated or clustered in small groups, and even intermingled with lymphocytes. Epithelioid cells may be observed in all reactive hyperplasia, mainly in toxoplasmosis related or during haematological diseases and or after chemo- or radiotherapy.
Multinucleated giant cells are large cells with a wide cytoplasm and even a dozen nuclei. Foreign body giant cells may be clustered and contain phagocyted material. Asteroid bodies are rarely seen.
Centrocytes are medium-size centrofollicular cells with irregular nuclei and scanty cytoplasm. Nuclei have dispersed chromatin and irregular shape with small cleavages. Deeper nuclear cleavages are better appreciated in histological sections than in the smears, where centrocytes may appear vaguely polygonal rather than roundish. Centrocytes can be significantly present in some follicular hyperplasia, in follicular lymphoma and mantle cell lymphoma.
Centroblasts are large centrofollicular cells with pale round nuclei with coarse chromatin and two or more marginal nucleoli. The latter are almost attached to the nuclear membrane on histological sections and often only eccentrical in the smears. Centroblasts can be significantly present in some follicular hyperplasia and in high grade follicular lymphoma.
Immunoblasts of either B or T phenotype are the largest lymphoid cells; they present with pale nuclei and one or two centrally located, very large nucleoli. A well defined basophilic rim of cytoplasm is generally present. Immunoblasts may be numerous in viral, postvaccinial and mononucleosis lymphadenitis and immunoblastic NHL.