This content is also available in:
![]() Čeština
Čeština ![]() Türkçe
Türkçe
General features
NHL is a heterogeneous group of neoplasms which represent 2-3% of all tumors in the Western World. They encompass both the slowest and the fastest growing tumors, ranging from chronic lymphatic leukemia/small lymphocytic lymphoma which, in the early stages, may be left untreated (watch and wait), to lymphoblastic lymphoma, which require timely and intense therapies. Moreover some entities are well identified by clinical, phenotypical, genetic and molecular profiles, as is generally the case for small-cell lymphomas. Others, such as diffuse, large, B-cell lymphoma, seem to be a container for different molecular phenotypical and clinical entities. Clinical signs, when present, are weight loss, itch, fever, weakness, cough or the mediastinal syndrome if the mediastinum is involved, or only lymph nodal enlargement. The site of the lymph nodes involved is quite variable, although anterior cervical nodes are the ones most frequently affected, followed by supra-clavear and axillary nodes. The NHL classification has been reformulated several times, reflecting the huge amount of knowledge gathered in the field of immunology and genetics of lymphomas.
NHL Classification
The World Health Organization Classification of Lymphomas (2001)
- B-CELL NEOPLASMS
- Precursor B cell neoplasm
- Precursor B-lymphoblastic leukemia/lymphoma
- Precursor B-cell acute lymphoblastic leukemia
- Mature (peripheral) B-cell neoplasms
- B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma (SLL/CLL)
- B-cell prolymphocytic leukemia Lymphoplasmacytic lymphoma (LPCL)
- Splenic marginal zone B-cell lymphoma (with/without villous lymphocytes)
- Hairy cell leukemia
- Plasma cell myeloma/plasmacytoma
- Extranodal marginal zone B-cell lymphoma of MALT type (MALT)
- Nodal marginal zone B-cell lymphoma (with/without monocytoid Bcells) (MZL)
- Follicular lymphoma (FL)
- Mantle-cell lymphoma (MCL)
- Diffuse large B-cell lymphoma (DLBCL)
- Burkitt lymphoma/Burkitt cell leukemia (BL)
- Precursor B cell neoplasm
- T-CELL AND NK-CELL NEOPLASMS
- Precursor T-cell neoplasm
- Precursor T-lymphoblastic lymphoma/leukemia
- Precursor T-cell acute lymphoblastic leukemia
- Mature (peripheral) T-cell neoplasms
- T-cell prolymphocytic leukemia
- T-cell granular lymphocytic leukemia
- NK-cell lymphomaleukemia (NKL)
- Adult T-cell lymphoma/leukemia (HTLV-1 positive)
- Extranodal NK/T-cell lymphoma, nasal type
- Enteropathy-type T-cell lymphoma
- Hepatosplenic gamma-delta T-cell lymphoma
- Subcutaneous panniculities-like T-cell lymphoma
- Mycosis fungoides/Sezarysyndrome
- Anaplastic large-cell lymphoma, T/null cell, primary cutaneous type
- Peripheral T-cell lymphoma, not otherwise characterized (PTL)
- Angioimmunoblastic T-cell lymphoma
- Anaplastic large-cell lymphoma, T/null cell, primary systemic type
- Precursor T-cell neoplasm
Role of cytology
The cytological diagnosis of NHL is hampered by objective difficulties. As for other neoplasms, many NHLs lack significant nuclear atypia because they are the clonal expansion of lymphoid cells in specific stages of maturation. Moreover these cells may be intermingled with different amounts of benign reactive lymphocytes, as in T-rich B-cell NHL, where reactive lymphocytes may prevail over neoplastic ones.
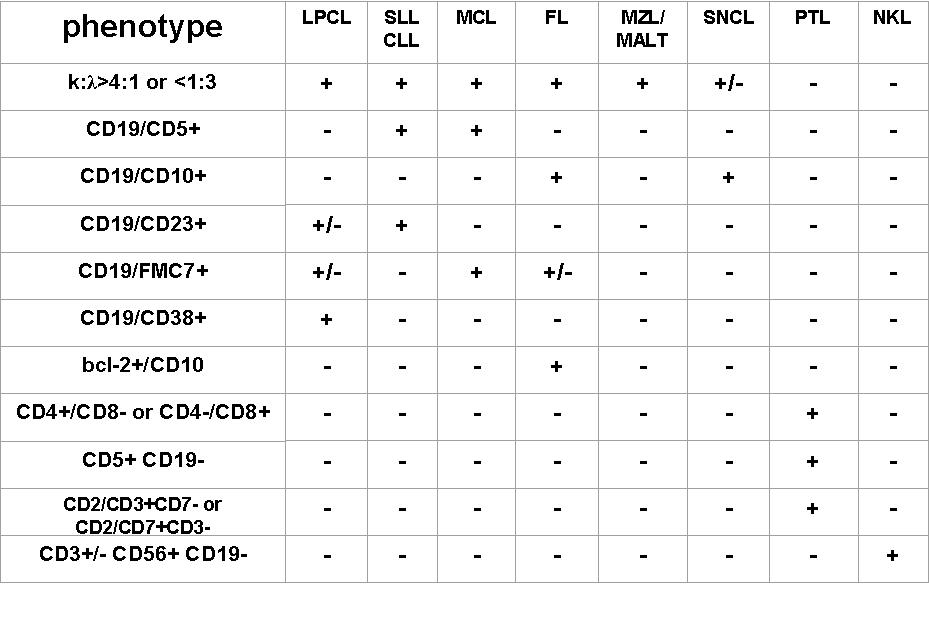
In practice, the cytological diagnosis of NHL is determined by a combination of microscopic features and ancillary techniques. Differentiated B-cell lymphomas generally show a more monomorphous cell pattern, but a definitive diagnosis may be made only by light chain clonality (?/? >4:1 or <1:1) or IGH rearrangement. Attention should be paid to quantitatively small unbalancements, especially if detected by FC (less than 20% of gated cells). In fact, small unbalancements, in the absence of lymphoma, may occur in reactive lymph nodes mainly in cases of autoimmune or immunodeficiency syndromes. Other than light chain restriction, there are other phenotypic patterns, mainly assessed by FC, which define a lymphoid cell population as B-lymphoma, and are frequently sub-type specific: CD5/CD19 co-expression (CLL/SLL or MCL); CD10/Bcl-2 co-expression (FL), CD10+ in all the gated cells, combined with a specific cytological pattern (BL, FL). T-cell lymphoma are more complex; peripheral T-cell generally express CD2/3/7 and alternatively CD4 or CD8. Loss of one antigen (often CD7) may suggest a clonal proliferation. CD3/CD56 over-expression is indicative of NK lymphoma.
Large cell B-cell lymphoma (DLBCL), generally presents more evident nuclear atypia in all its microscopic and phenotypic variants (centroblastic, immunoblasic, anaplastic). In these cases cytological features and phenotypic assessment can be diagnostic (CD19+, aberrant phenotypes by FC, ALK+,CD30-, EMA+ in DLBCL ALK+ by ICC).
Cytological features combined with ancillary techniques allow a correct diagnosis and classification in most cases. However cytopathologists should be aware that objective limitations still exist in both the diagnosis and classification of NHL. When a defined diagnosis of B NHL has been assessed, a possible sub-classification may be attempted combining cytological features and phenotypic patterns using ICC or FC.
In many institution the cytological diagnosis of NHL is accepted without histological control in cases of relapses and in peculiar primary cases; conversely the histological confirmation is necessary for primary diagnoses and in all cases where cytological, clinical and instrumental findings appear contradictory. In addition to repeating the test, surgical excision and histological examination should always be included in the cytological reports of all doubtful cases.