This content is also available in:
![]() Čeština
Čeština ![]() Türkçe
Türkçe
HODGKIN LYMPHOMA (HL)
- General features
- Classification
- FNC evaluation
- Nodular lymphocyte predominant, Hodgkin lymphoma: Cytological findings
- Classical Hodgkin lymphoma: Cytological findings
General features
- HL represents approximately 30% of all lymphomas and has a bimodal age curve with a peak at 15-35 years and a second peak over forties. EB virus is probably involved in the pathogenesis, and progressively transformed germinal centres are considered a precursor lesion of the nodular lymphocyte predominant variant. Clinical signs, when present, are nocturnal sweating, itch, fever, weakness, cough or the mediastinal syndrome if the mediastinum is involved; corresponding patients are designed as B at the staging, or A when lymph nodal enlargement only are present without clinical signs. HL often arises in cervical lymph nodes and involves the contiguous nodes. The mediastinum is involved mainly in nodular sclerosis and the spleen in mixed cellularity.
- The lymph node architecture is effaced by a variable number of scattered large mononucleated cells: Hodgkin cells (HC); lobulated mononucleated cells: popcorn cells (L&H); and multinucleated cells: Reed-Sternberg cells (HRS) in a background composed by a heterogeneous admixture of fibrous stroma and non-neoplastic lymphoid cells, neutrophils and eosinophils. Treatment of HL is based on clinical and pathological staging and prognosis is excellent in most patients.
Classification
The World Health Organization Classification of Lymphomas (2001)
HODGKIN LYMPHOMA (HODGKIN DISEASE) (WHO 2001)
- Nodular lymphocyte-predominant Hodgkin lymphoma
- Classical Hodgkin lymphoma
Nodular sclerosis classical Hodgkin lymphoma Mixed cellularity classical Hodgkin lymphoma Lymphocyte-rich classical Hodgkin lymphoma Lymphocyte-depleted classical Hodgkin lymphoma
Power Doppler US pattern and FNC guide in Hodgkin lymphoma
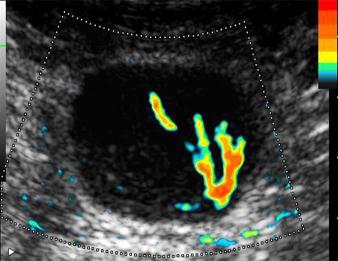
Power Doppler may reveal an abnormal vascular pattern in a defined area of the lymph node
that may be used as target in the FNC guide.

Power Doppler may reveal an abnormal vascular pattern
in a defined area of the lymph node that may be used as target in the FNC guide.
FNC evaluation
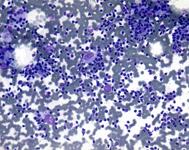
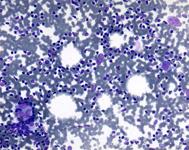
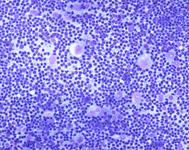
Smears may be highly or scantily cellular; the patterns are variable depending on the corresponding histotypes, the amount of fibrosis, and the different cell composition in the different areas of the lymph node. The general appearance of the smears is polymorphous with mature lymphocytes and follicular centre cells, and a variable amount of neutrophils and eosinophils. Epithelioid cells may also be present; nuclear crushes and lymphoid tangles are expression of concomitant fibrosis. The cytological diagnosis is made in the presence of HC and RSL, which may be present in variable amounts and are generally related to the corresponding histotypes: few in lymphocyte-rich and nodular sclerosis, more in mixed cellularity and lymphocyte depletion. In nodular lymphocyte-predominant Hodgkin lymphoma the diagnosis is related to the identification of L&C in a lymphoid background. Diagnostic cells are identified by ICC evidence of CD15 and CD30 positivity. ICC evidence of CD20+ of L&H cell may be equivocal because large follicular lymphoid cells may be CD20+ as well.
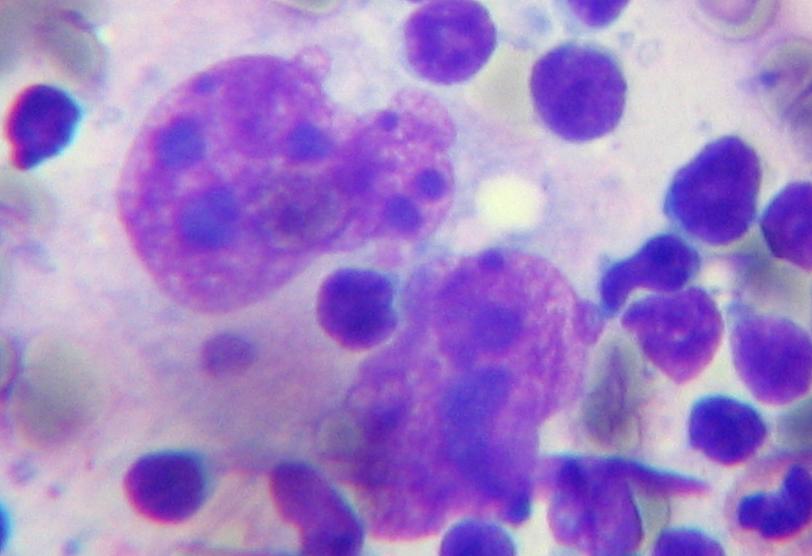
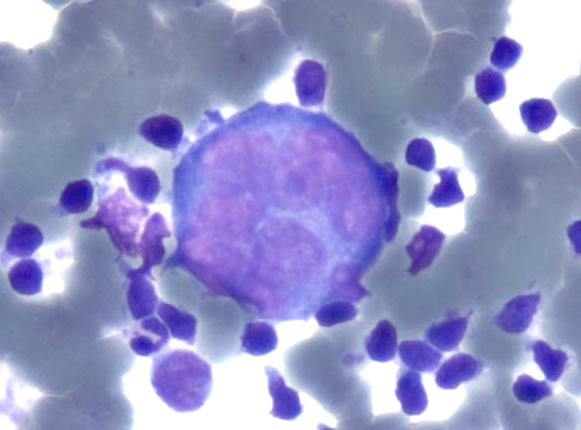
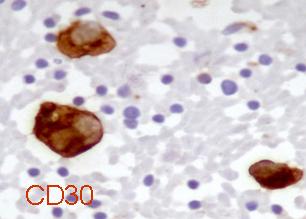
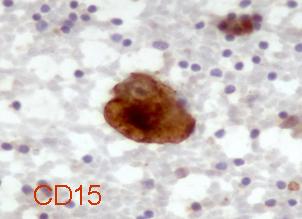
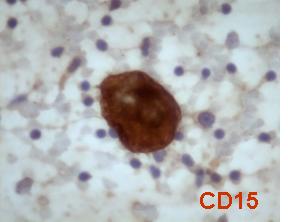
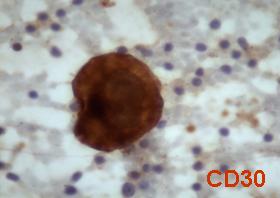
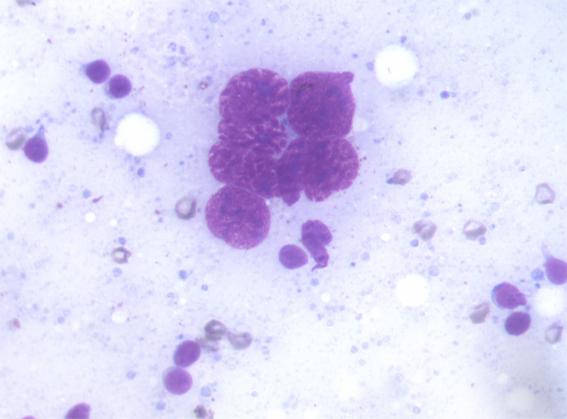
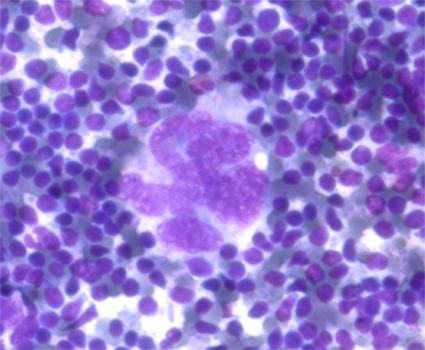
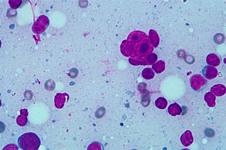
HODGKIN LYMPHOMA: diagnostic cells
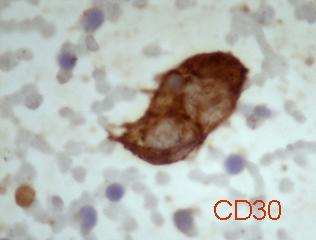
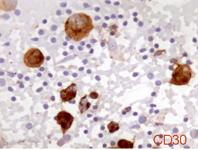
RS cells with lobated nuclei, clumped chromatin and large nucleoli, CD30+:

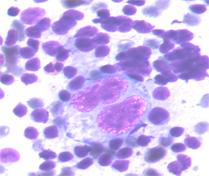
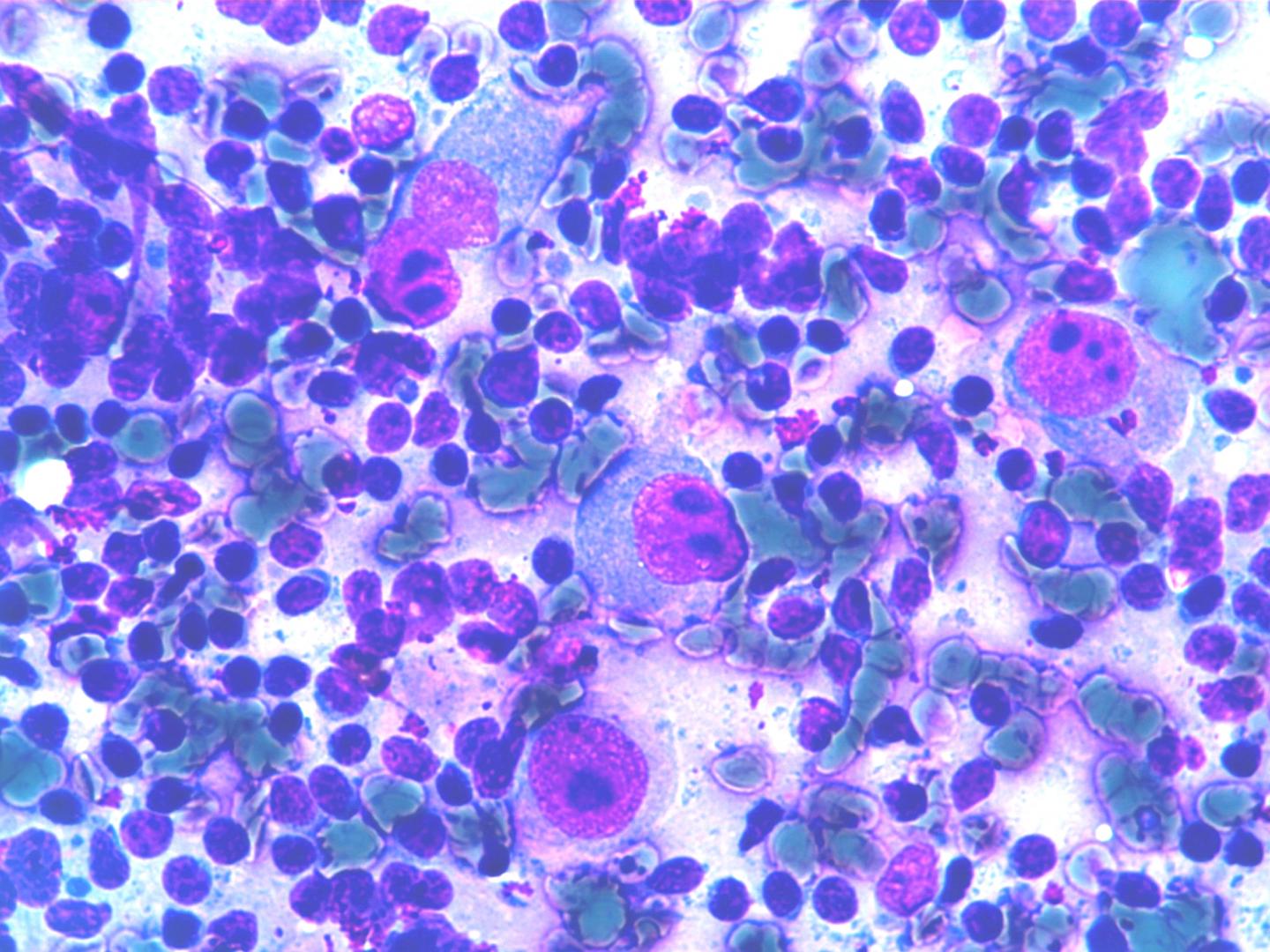
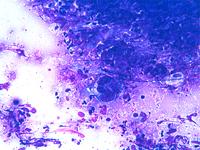
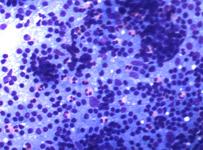
Hodgkin cell in a polymorphus background with numerous eosinophils:
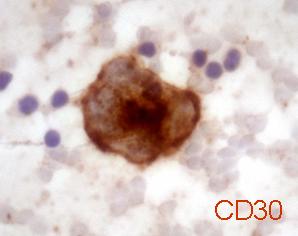
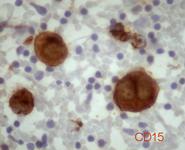
RS cells, CD15 and CD30 positives, with lobated nuclei, irregular chromatin and numerous large nucleoli:
RS cells with lobated nuclei, clumped chromatin and large nucleoli, CD30+:
Mononucleated HC cells with irregular chromatin and extremely large nucleoli:
CD15 and CD30 positive, mononucleated HC cells:
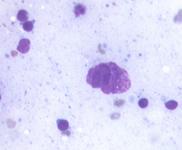
A multinucleated cell with clumping chromatin and hypercromasia. This cell may be considered a mummified RSH cells:
A polyploid, multinucleated, nucleolated RSH cells in a lymphoid background:
Nodular lymphocyte predominant, Hodgkin lymphoma: Cytological findings
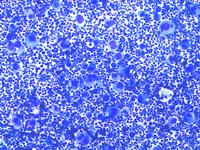
- Nodular lymphocyte-predominant Hodgkin lymphoma is characterized by a diffuse lymphoid background with a variable number of large neoplastic monucleated cells known as lymphocytic and/or histiocytic Reed-Sternberg cell variants (L&H). The nuclei are often folded or multilobated, the chromatin is mostly vesicular, the nucleoli are usually multiple and smaller than those seen in classical HRS cells. Small lymphocytes, histiocytes and some polyclonal plasma cells are present in the background.
- ICC: L&H cells: CD15-, CD30-, CD20+, CD79a+, BCL6+ and CD45+.
- FC: not contributive, CD4/CD8 co-expression has been reported.
Nodular lymphocyte predominant, Hodgkin lymphoma
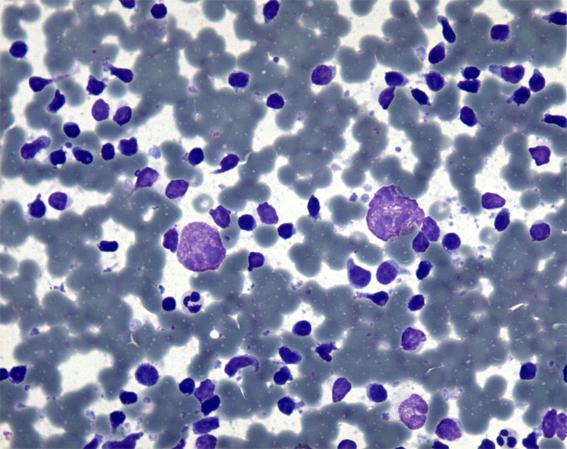
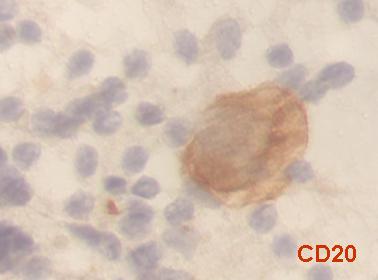
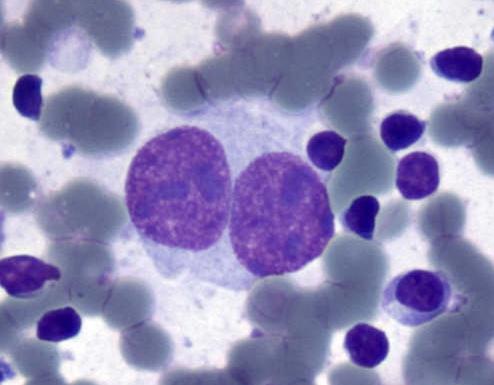
Lymphocytic and/or histiocytic Reed-Sternberg cell variants (L&H). The nuclei may be round, folded or multilobated, the chromatin is mostly vesicular, the nucleoli are usually multiple and smaller than those seen in classical HRS cells. L&H cells are CD20+, CD15-,CD30-.
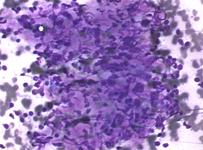
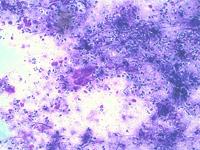
Classical Hodgkin lymphoma: Cytological findings
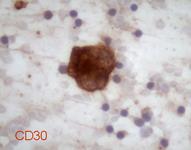
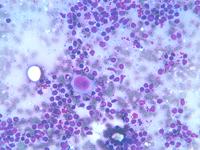
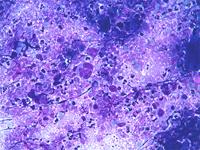
Classical Hodgkin lymphoma: HRS cells are large and show abundant, slightly basophilic, cytoplasm and two or more nuclear lobes or nuclei. Diagnostic RS cells have at least two nucleoli in two separate nuclear lobes. Mononuclear variants are termed Hodgkin cells, and the cells represent only a minority of the cellular infiltrate. The background is composed by reactive cellular infiltrate that varies according to the histological subtype. HRS cells are positive for CD30 in nearly all cases, for CD15 in the majority of cases and usually negative for CD45. Most HRS cells express the proliferation-associated nuclear antigen Ki-67.
Classical Hodgkin lymphoma is classified as:
Nodular sclerosis, Lymphocyte-rich, Mixed cellularity and Lymphocyte-depleted
- Nodular sclerosis contains a variable number of HRS cells in a background of small lymphocytes and other non-neoplastic inflammatory cells. Diagnostic cells may be rare or extremely numerous as in the syncitial variant. The HRS cells of this subtype tend to have more lobated nuclei with smaller lobes, and less prominent nucleoli. Lacunar HRS, determined by formalin fixation, which characterize this entity on histological sections are not observed on the smears. Eosinophils may be numerous.
- Mixed cellularity HRS cells are typical; the background cells consist of a mixture of eosinophils, neutrophils, histiocytes and plasma cells. One cell type may prevail over the others. The histiocytes may show pronounced epithelioid differentiation and may form granuloma-like clusters.
- Lymphocyte-rich: scattered HRS cells in a background characterized by an abundance of small lymphocytes. Eosinophils and neutrophils may be present in small numbers. The small lymphocytes may be admixed with a large number of histiocytes with or without epithelioid features.
- Lymphocyte-depleted: rich in HRS cells and/or depleted in non-neoplastic lymphocytes. In some cases pleomorphic HRS cells may predominate, producing a sarcomatous appearance.
- ICC: HC and HRS cells: CD15+, CD30+, CD20-, CD45-.
- DD: DLBCL: all types or metastasis in syncitial variant.
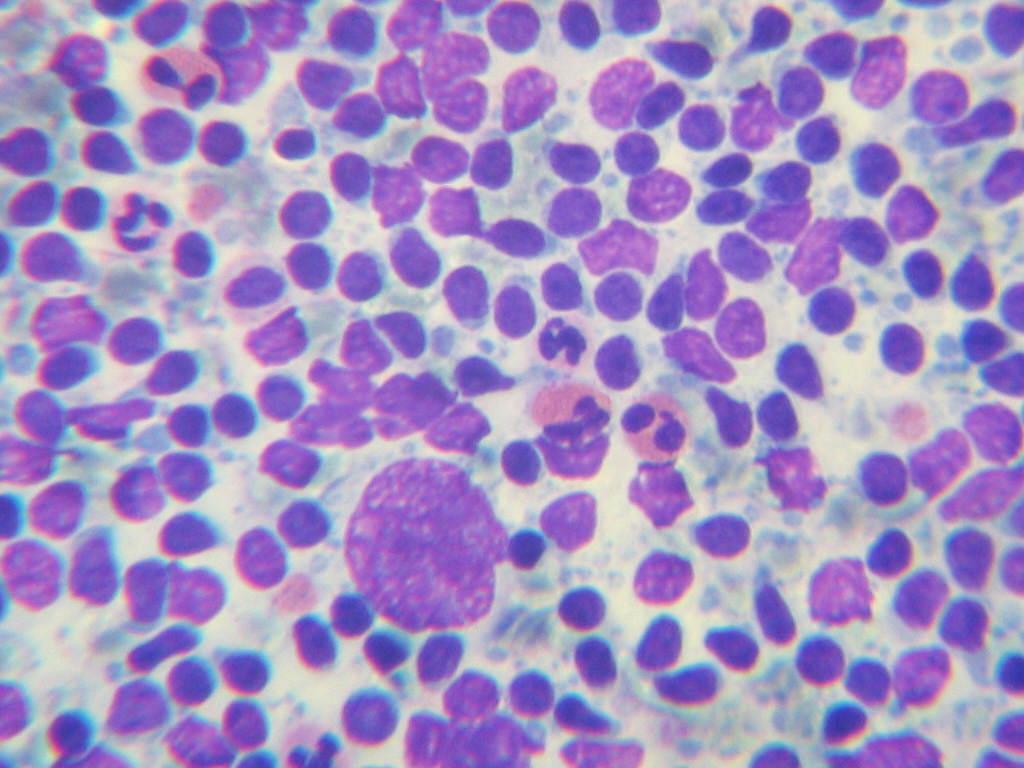
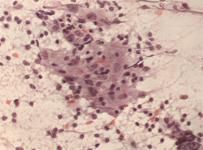
Classical Hodgkin lymphoma
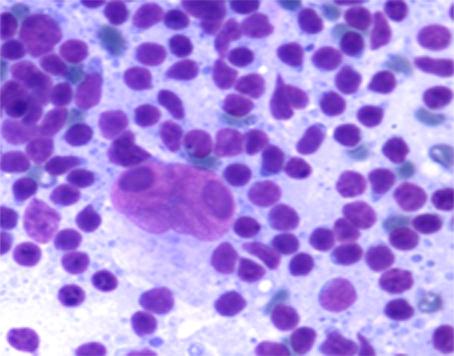
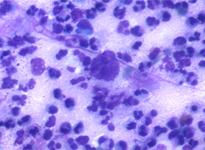
HL: One RSH cell (lower left) and two HC (center) in a lymphoid background.
A granulomatous pattern without a consistent clinical context might hide a HL. At the same time granulomatous pattern may be observed in the follow-up of HL and NHL