This content is also available in:
![]() Español
Español ![]() Čeština
Čeština ![]() Magyar
Magyar ![]() Polski
Polski
Metastatic tumours
- Carcinoma
- Malignant melanoma
- Non-Hodgkin lymphoma
- Sarcoma
Metastatic carcinoma
Metastatic carcinomas are by far the most common tumors found in effusions. Adenocarcinomas are more common than squamous cell or undifferentiated carcinomas.
Histologic types which can be diagnosed:
- Adenocarcinoma
- Small cell carcinoma
- Squamous cell carcinoma
In most cases the cells are morphologically distinct from mesothelial cells. They are often larger and more pleomorphic than mesothelial cells, but they can be smaller and more uniform in size as well. Most commonly, they are distinguished from mesothelial cells by their tendency to form large clusters; however, some carcinomas exfoliate as isolated cells.
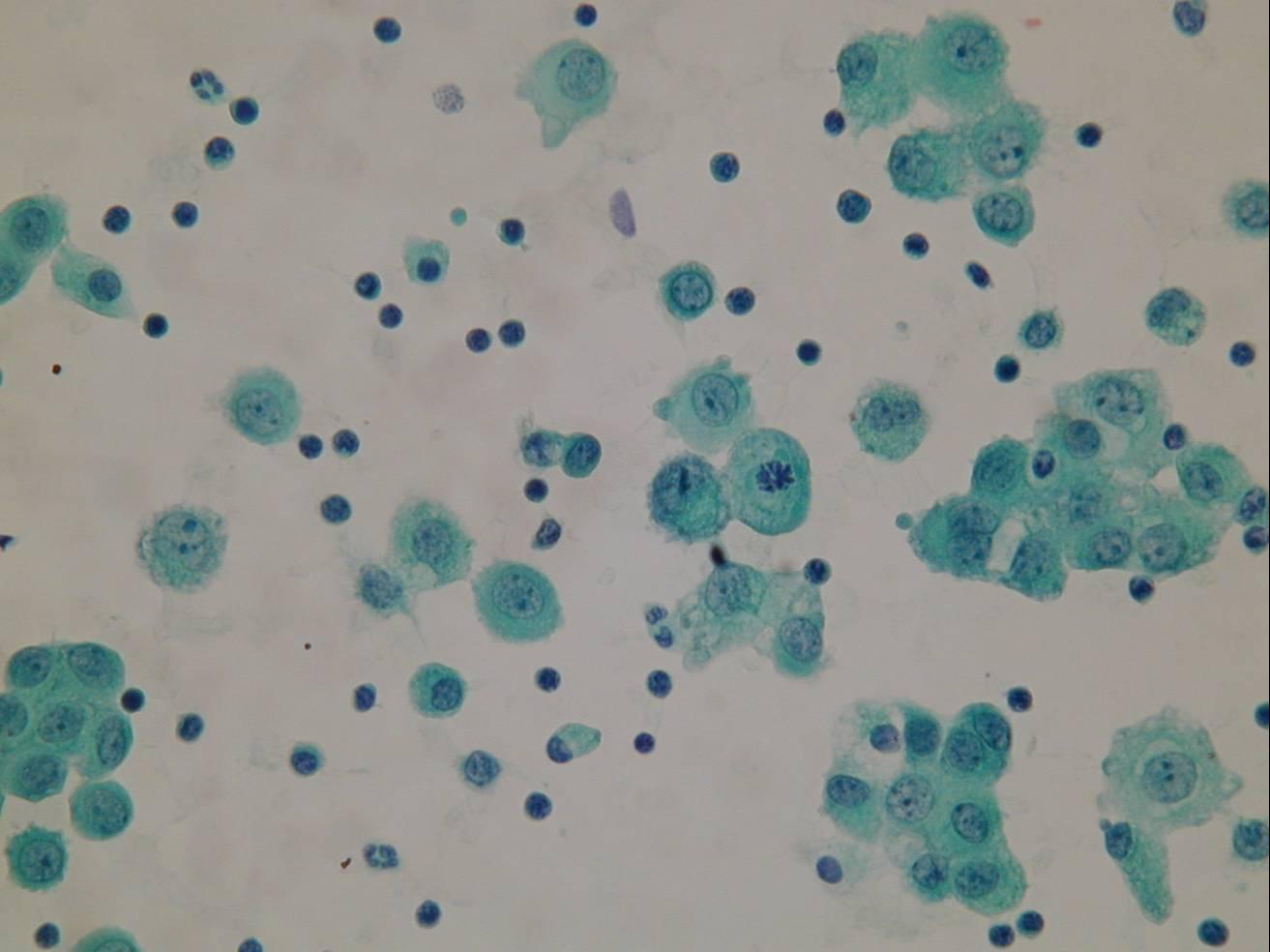
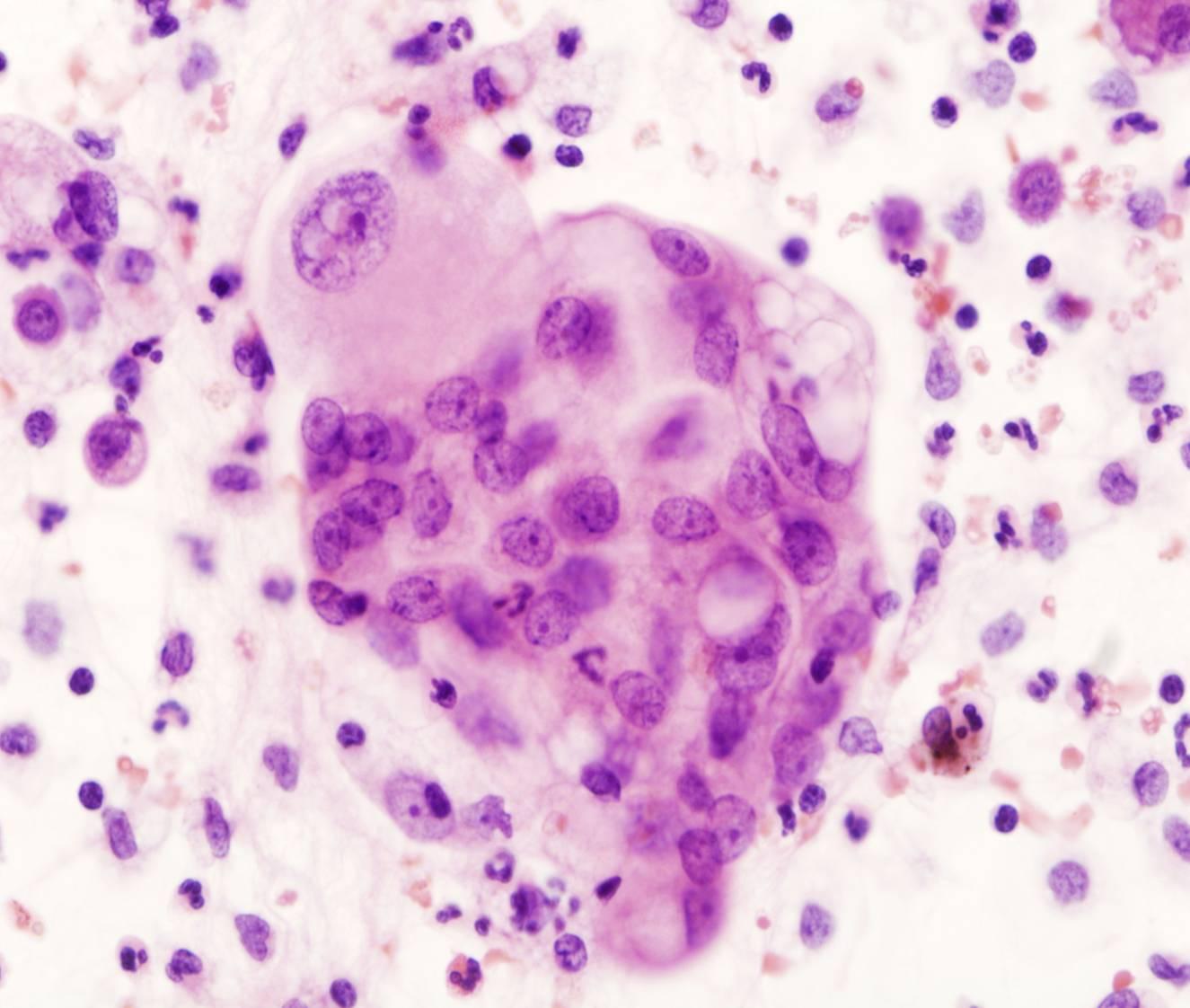
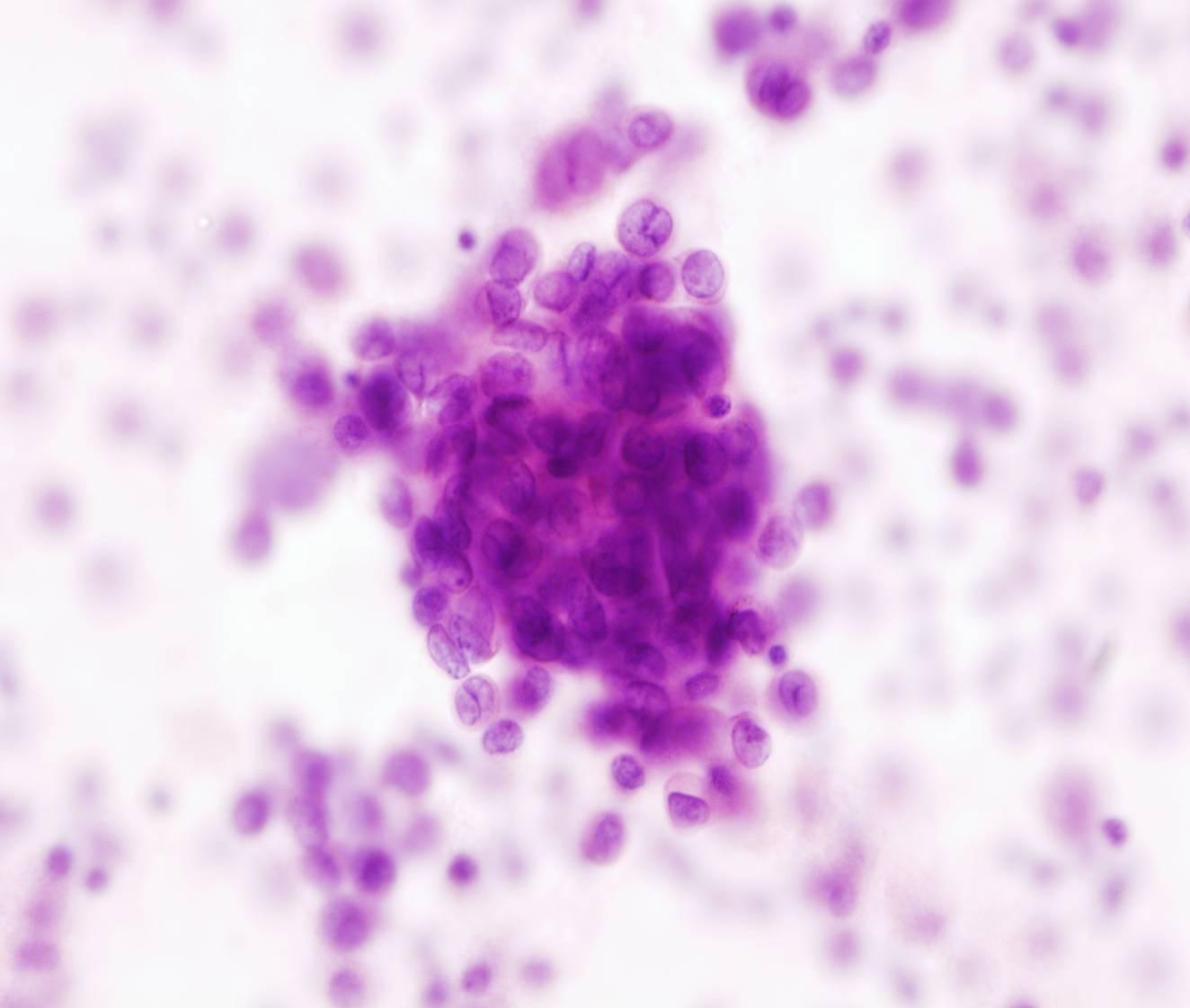
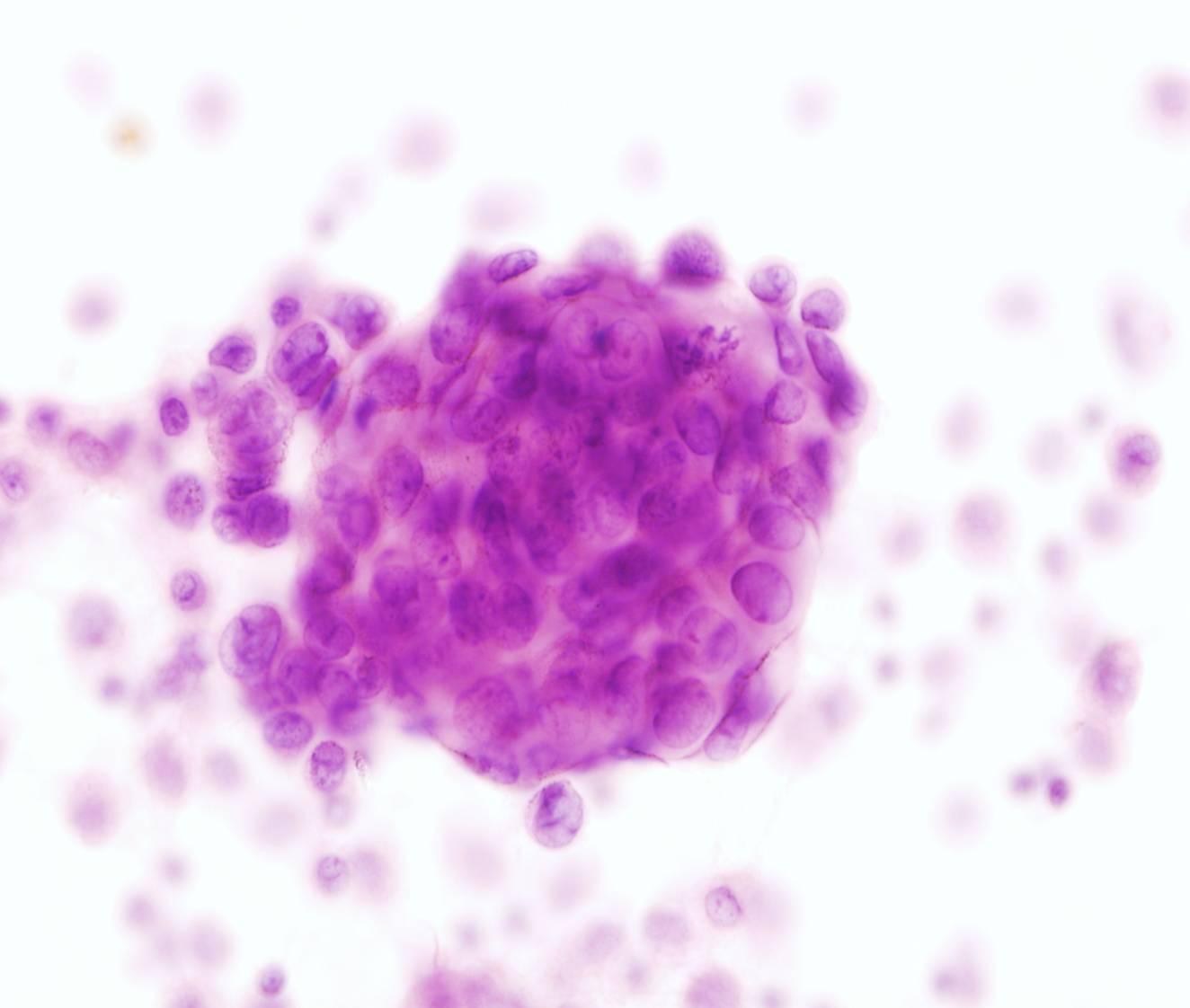
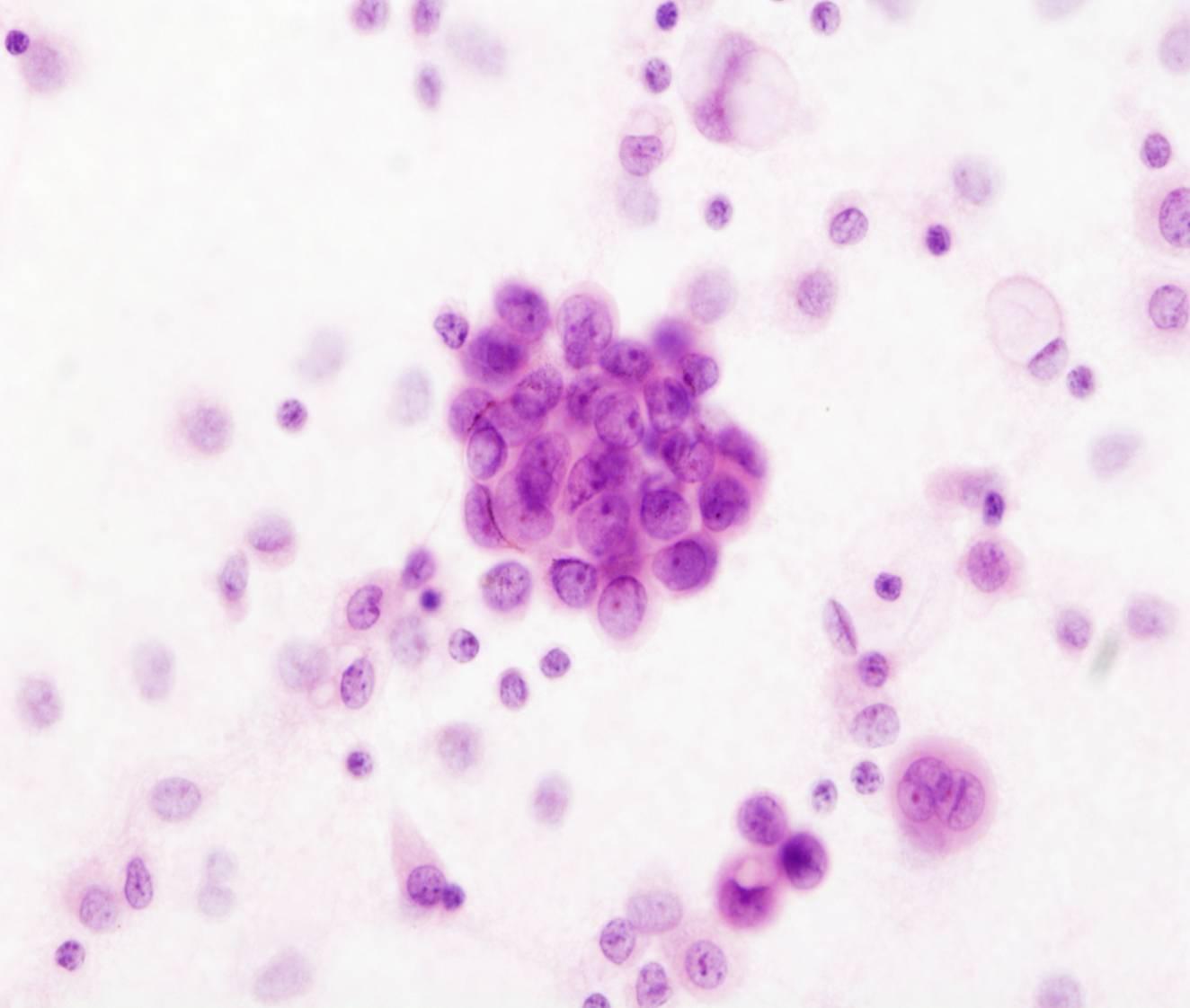
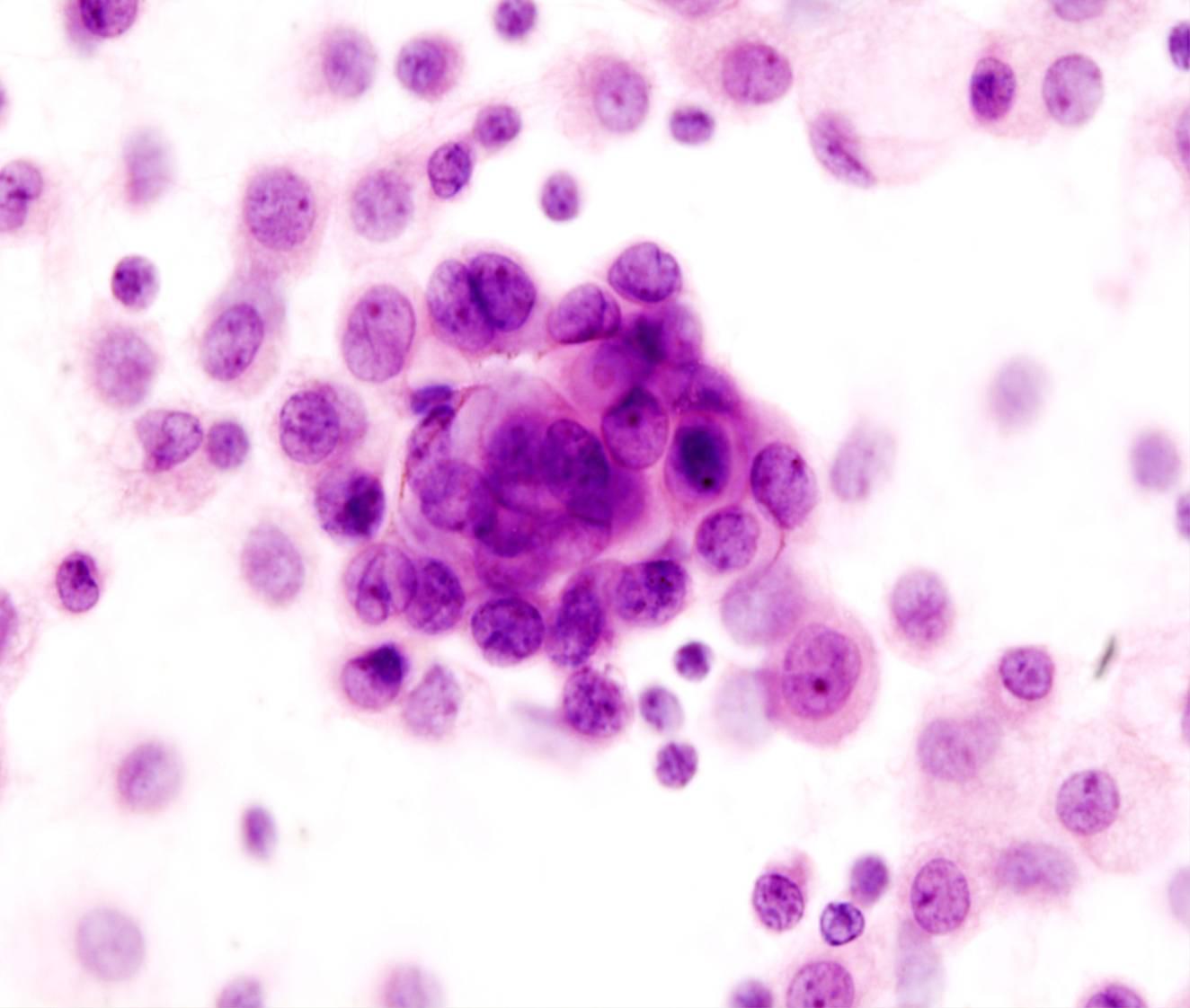
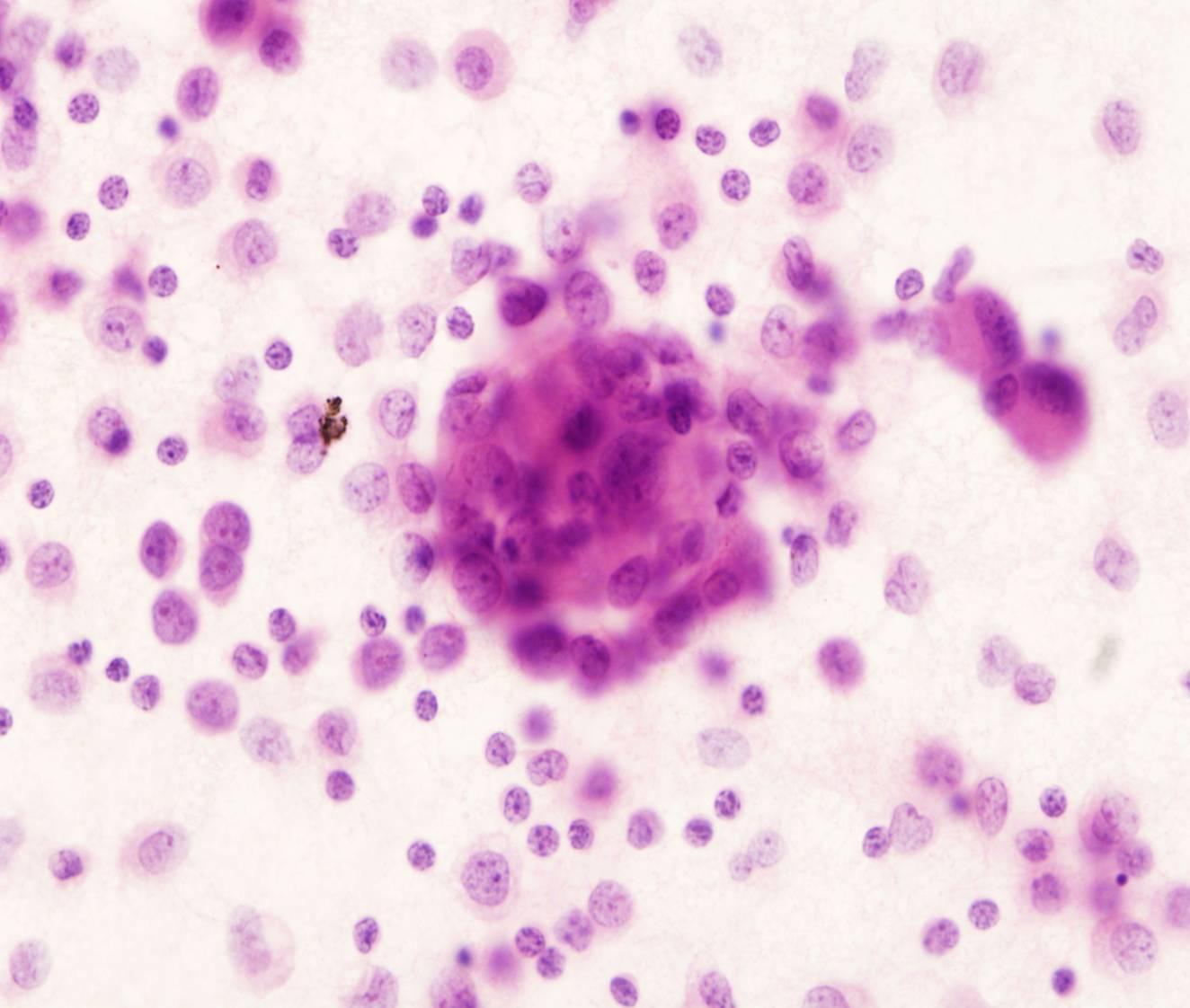
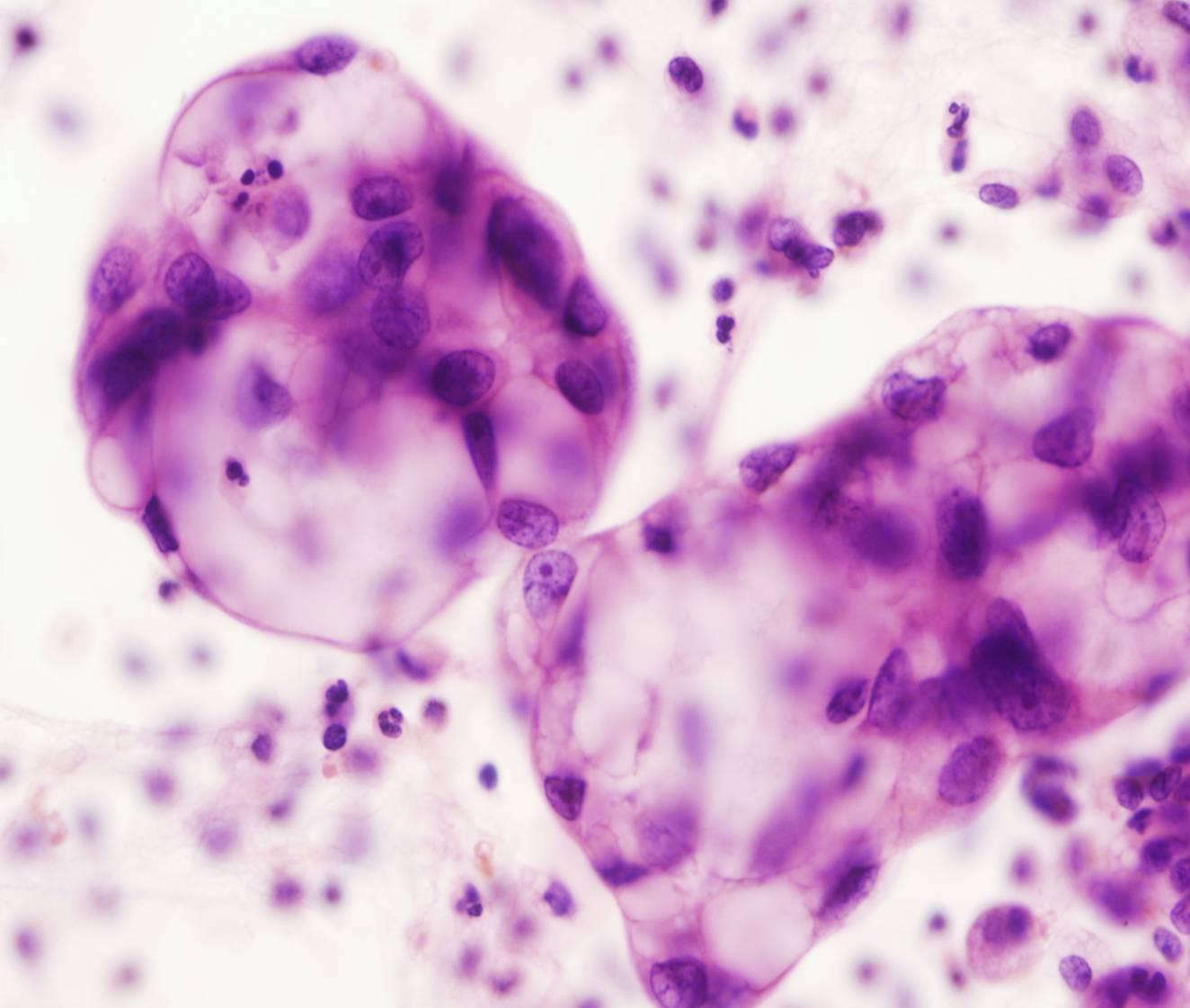
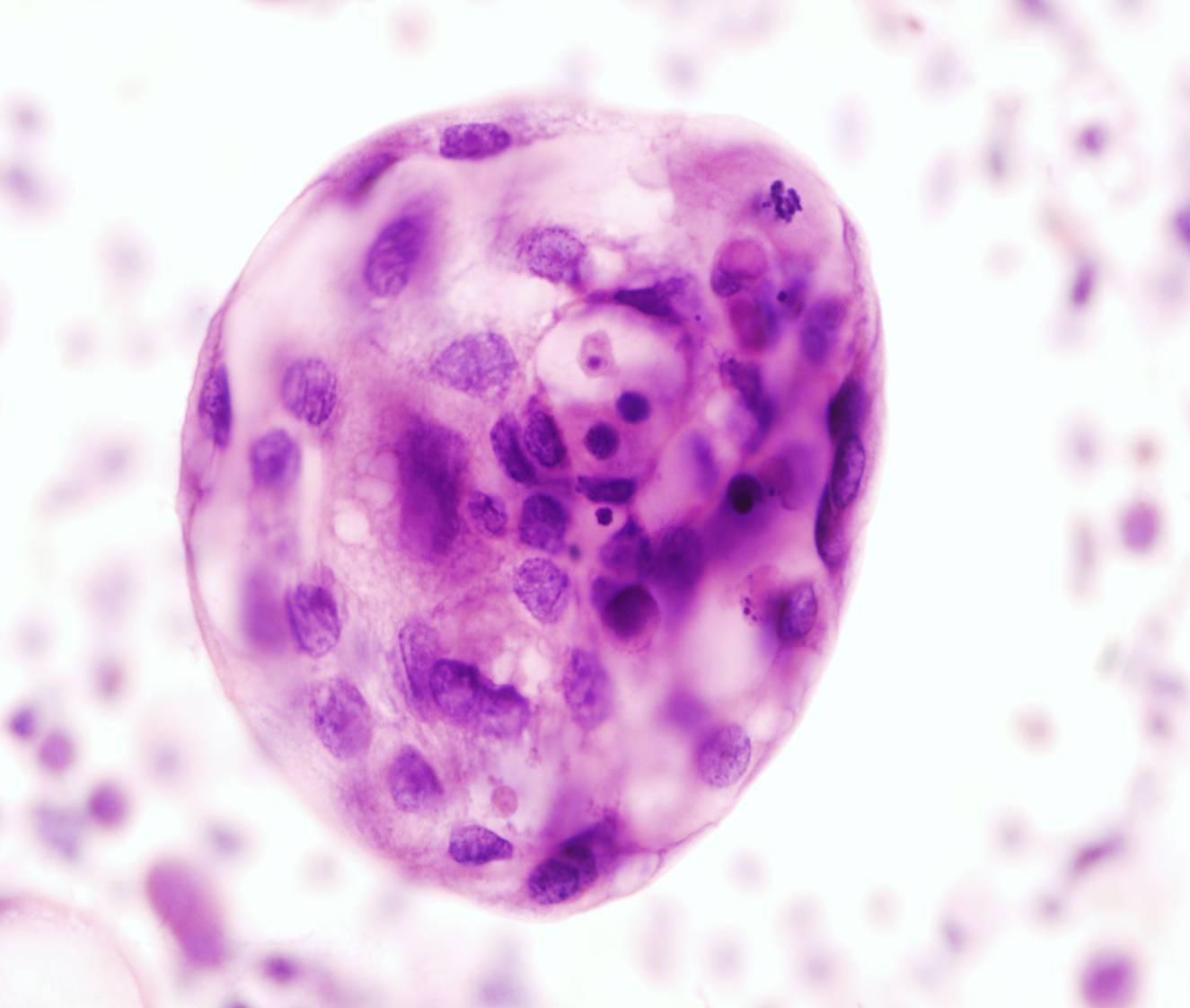
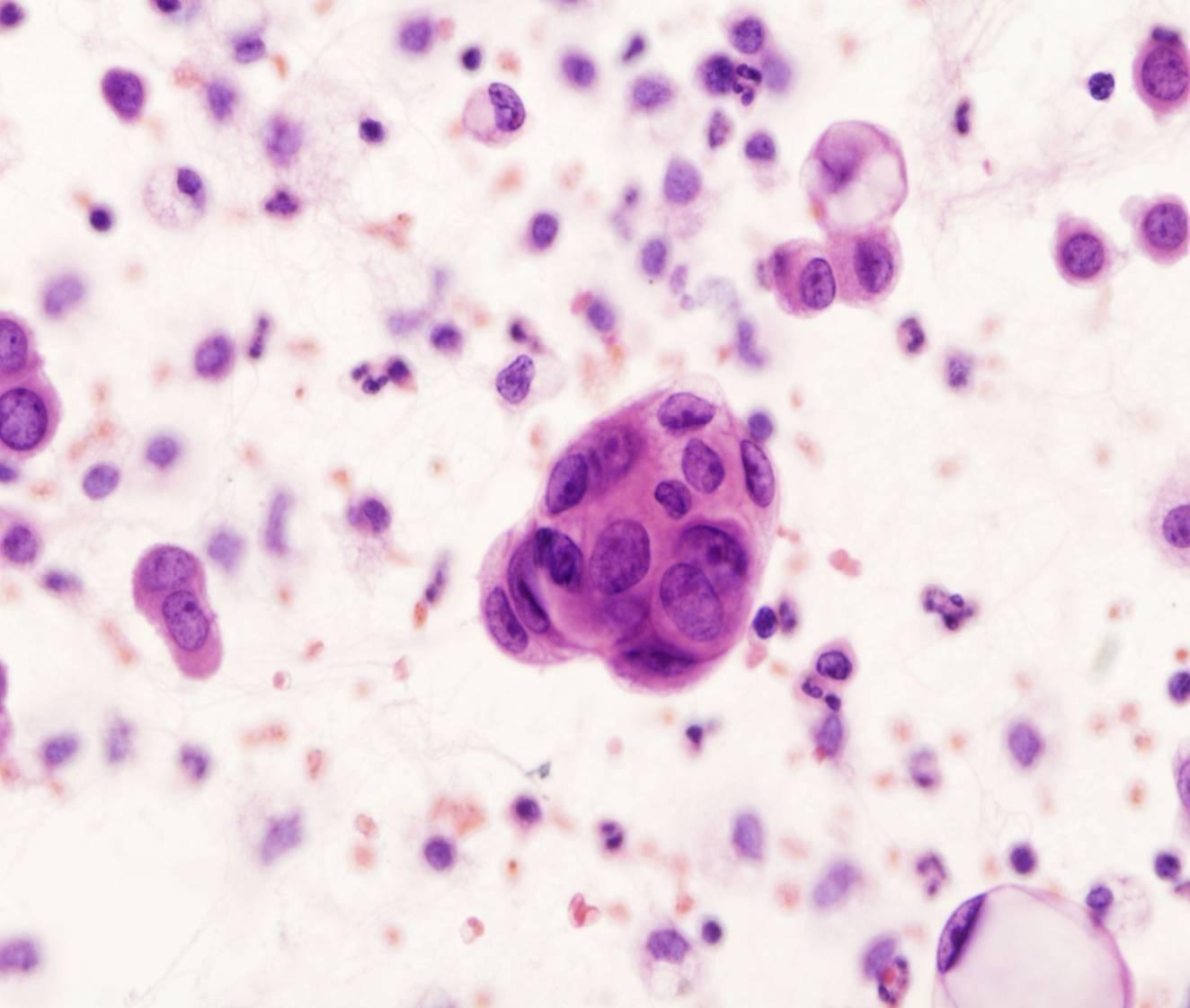
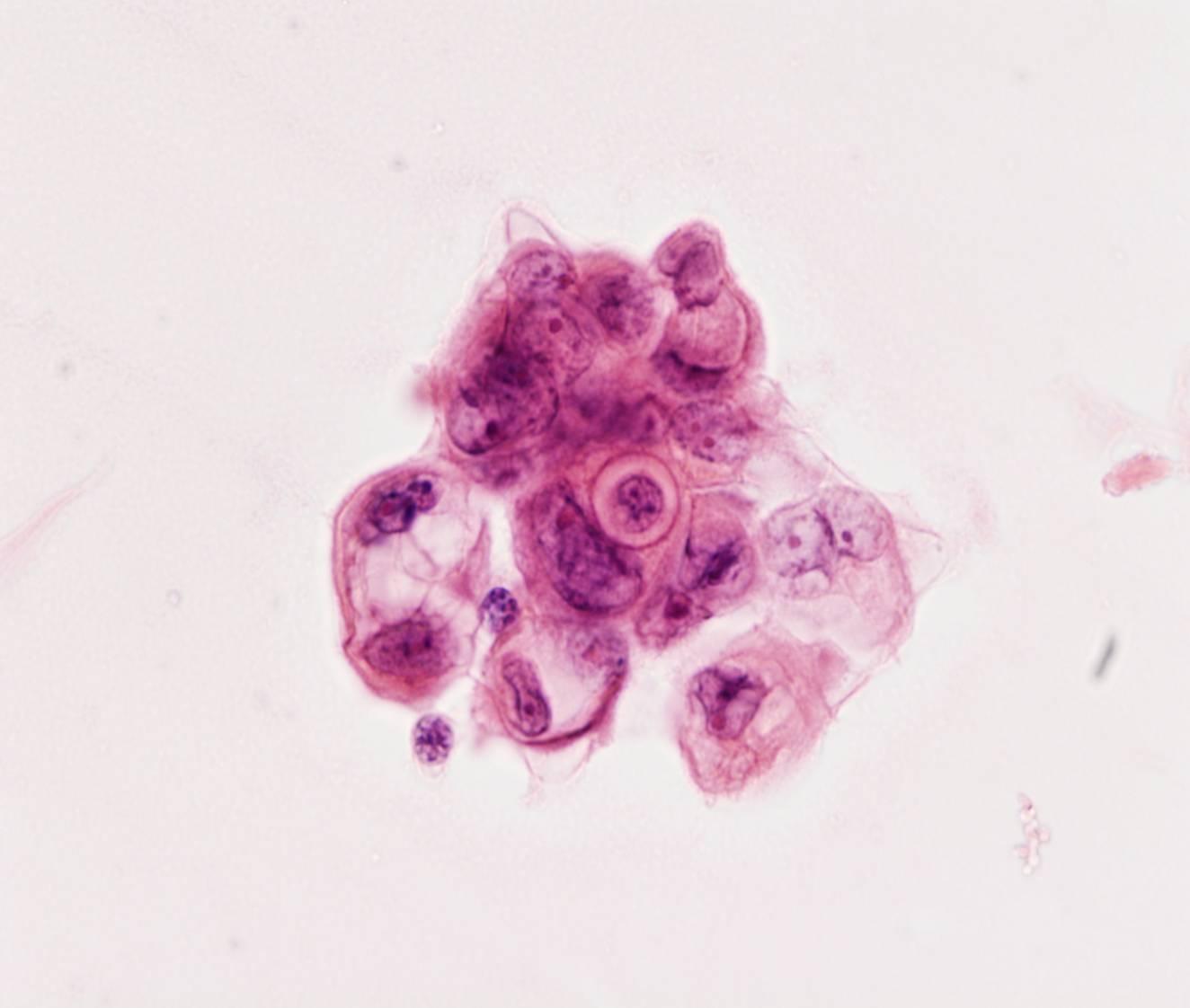
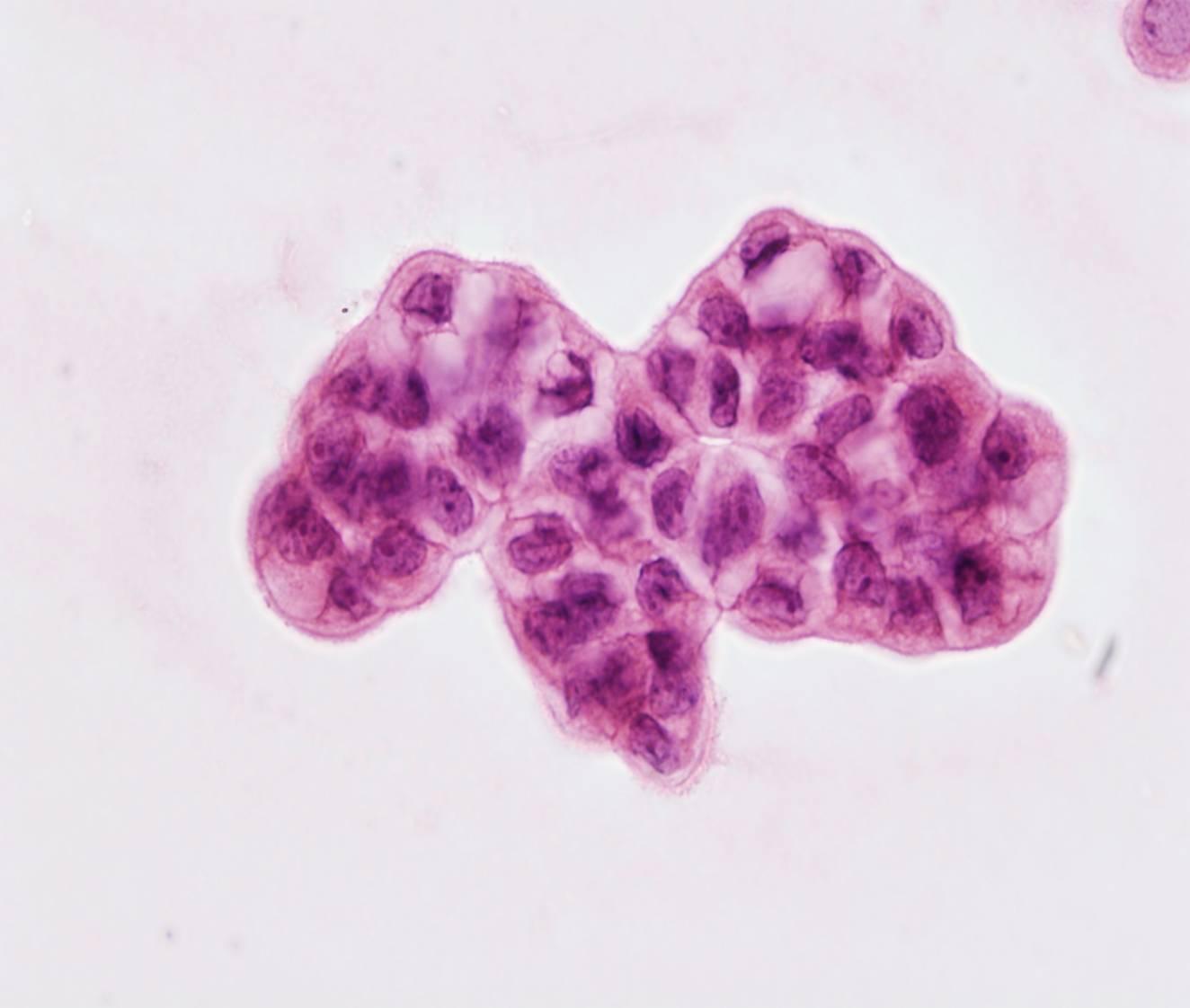
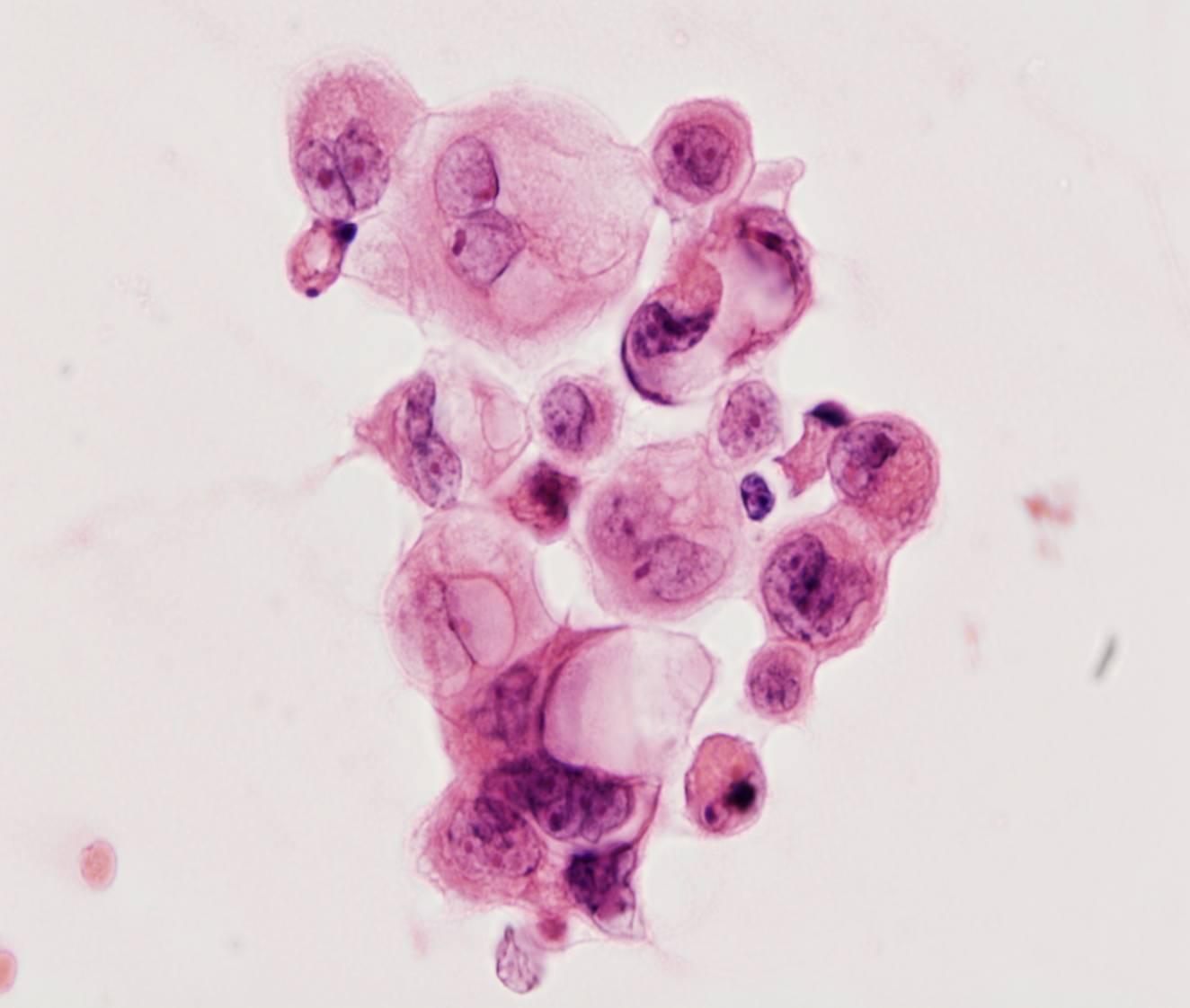
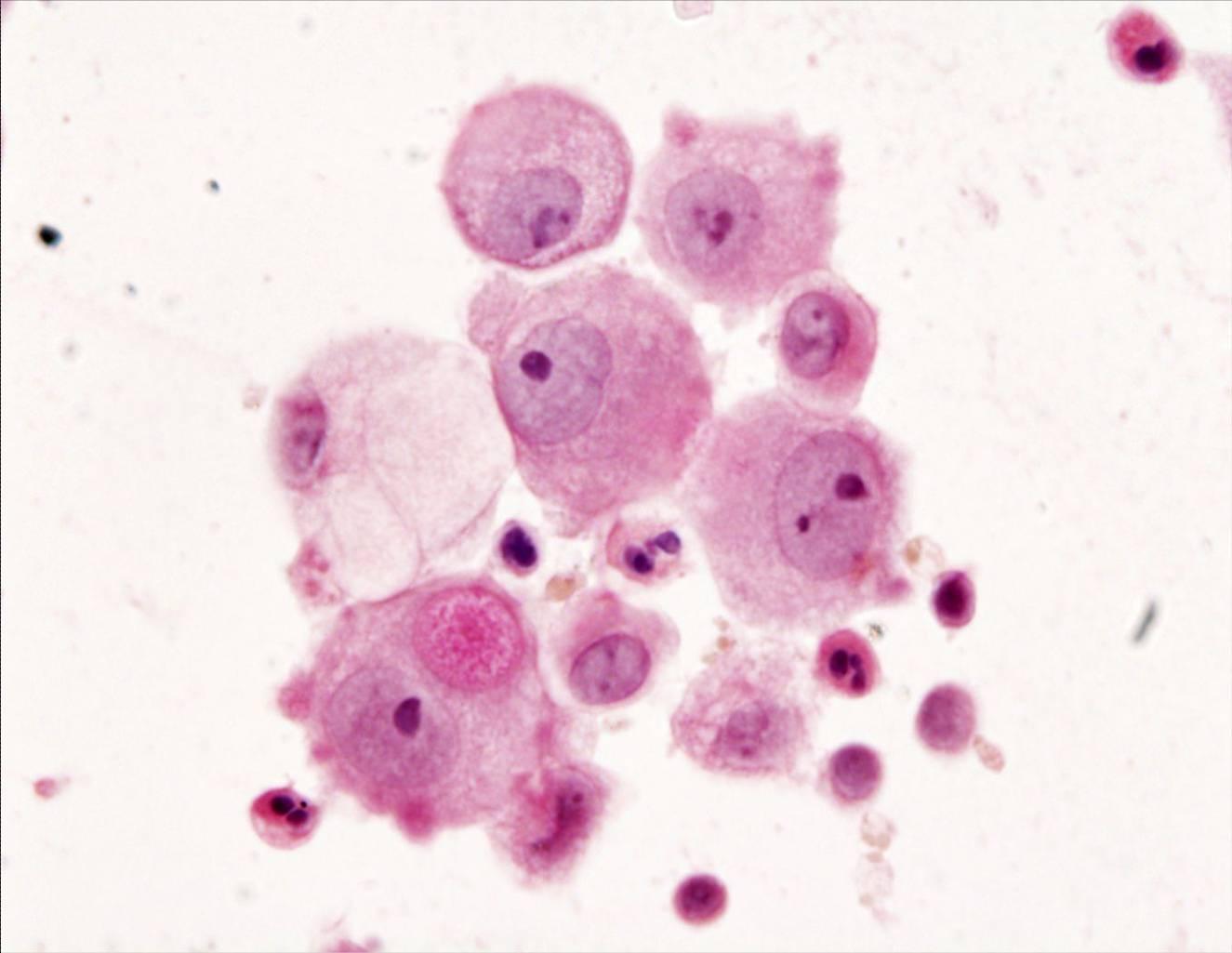
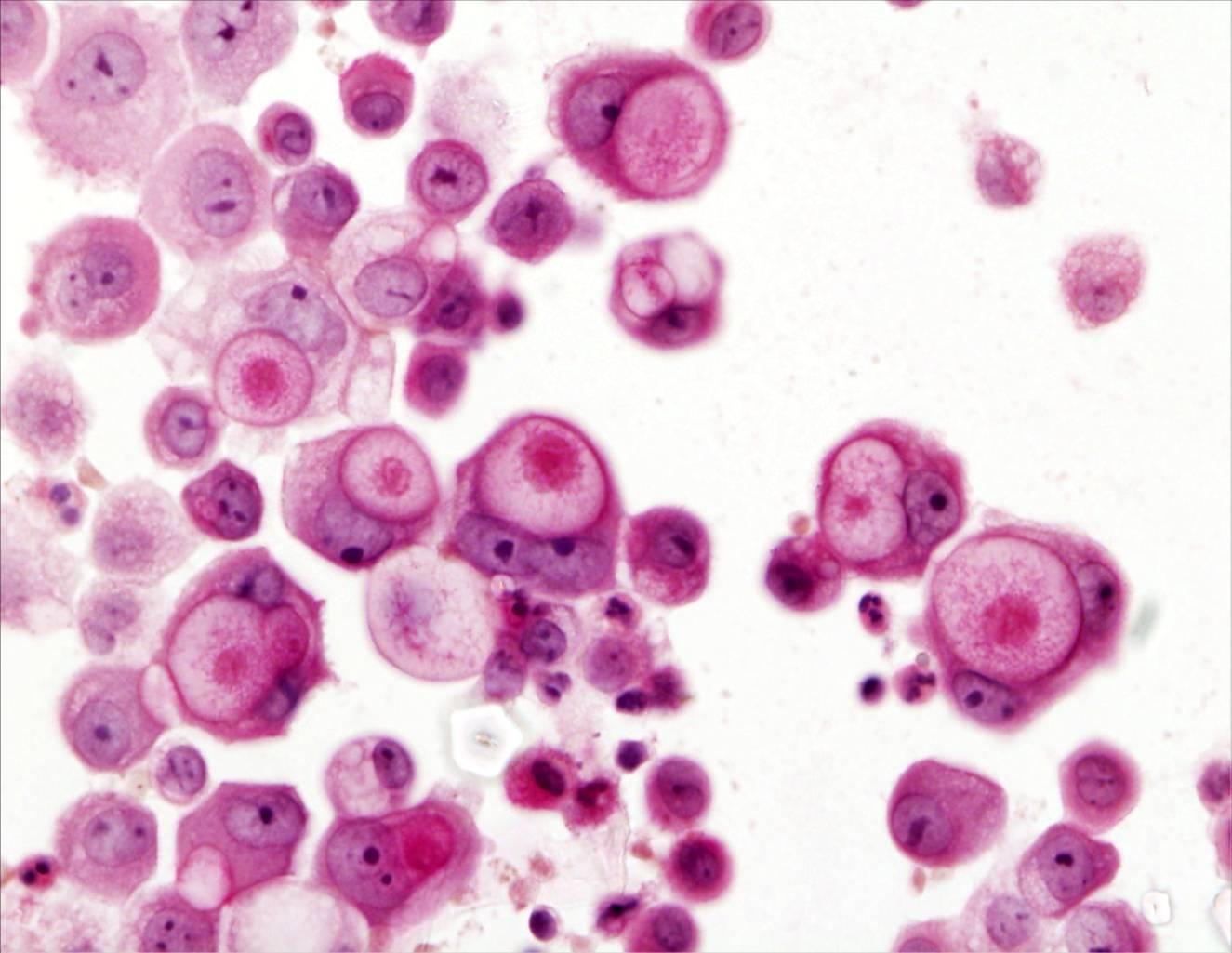
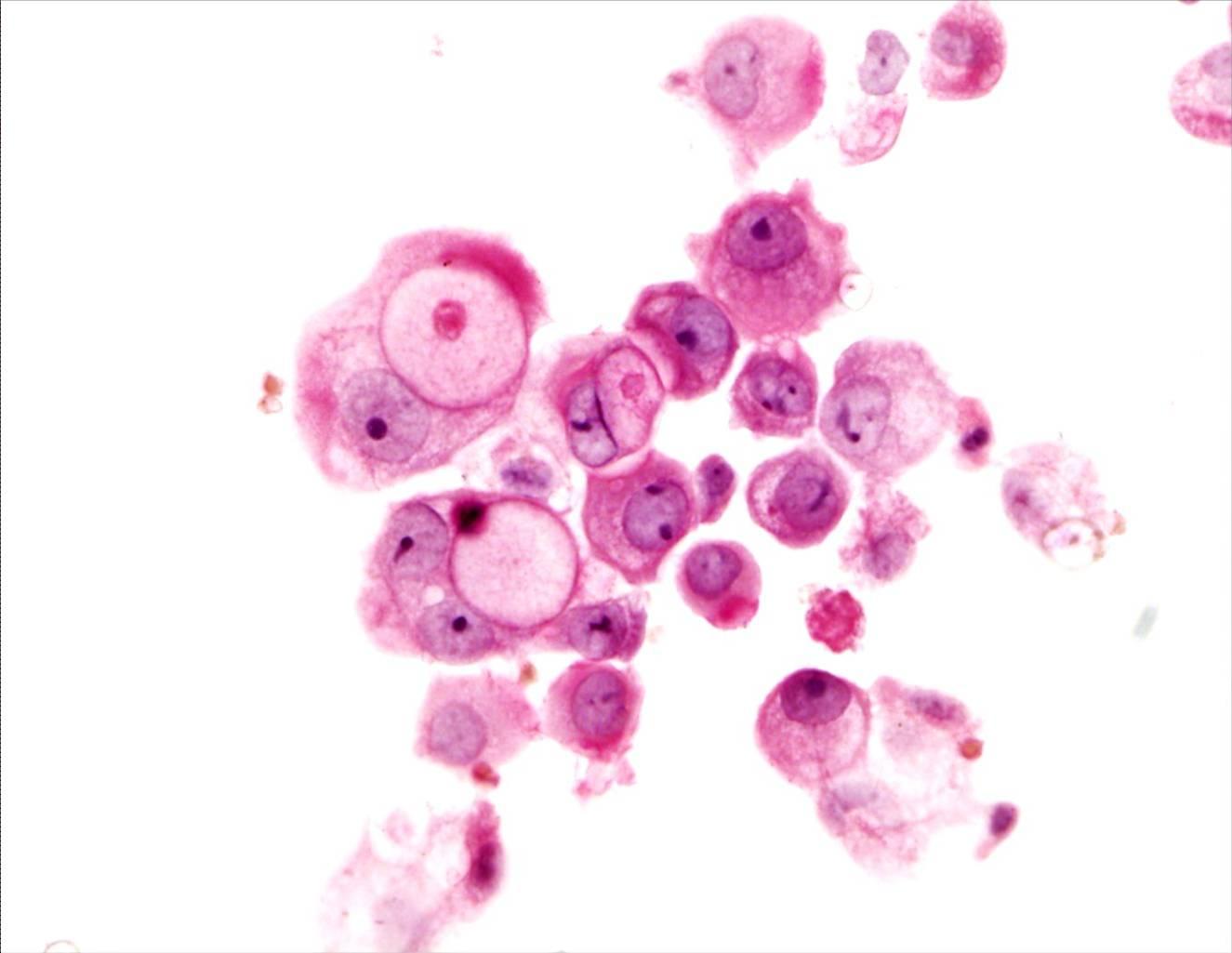
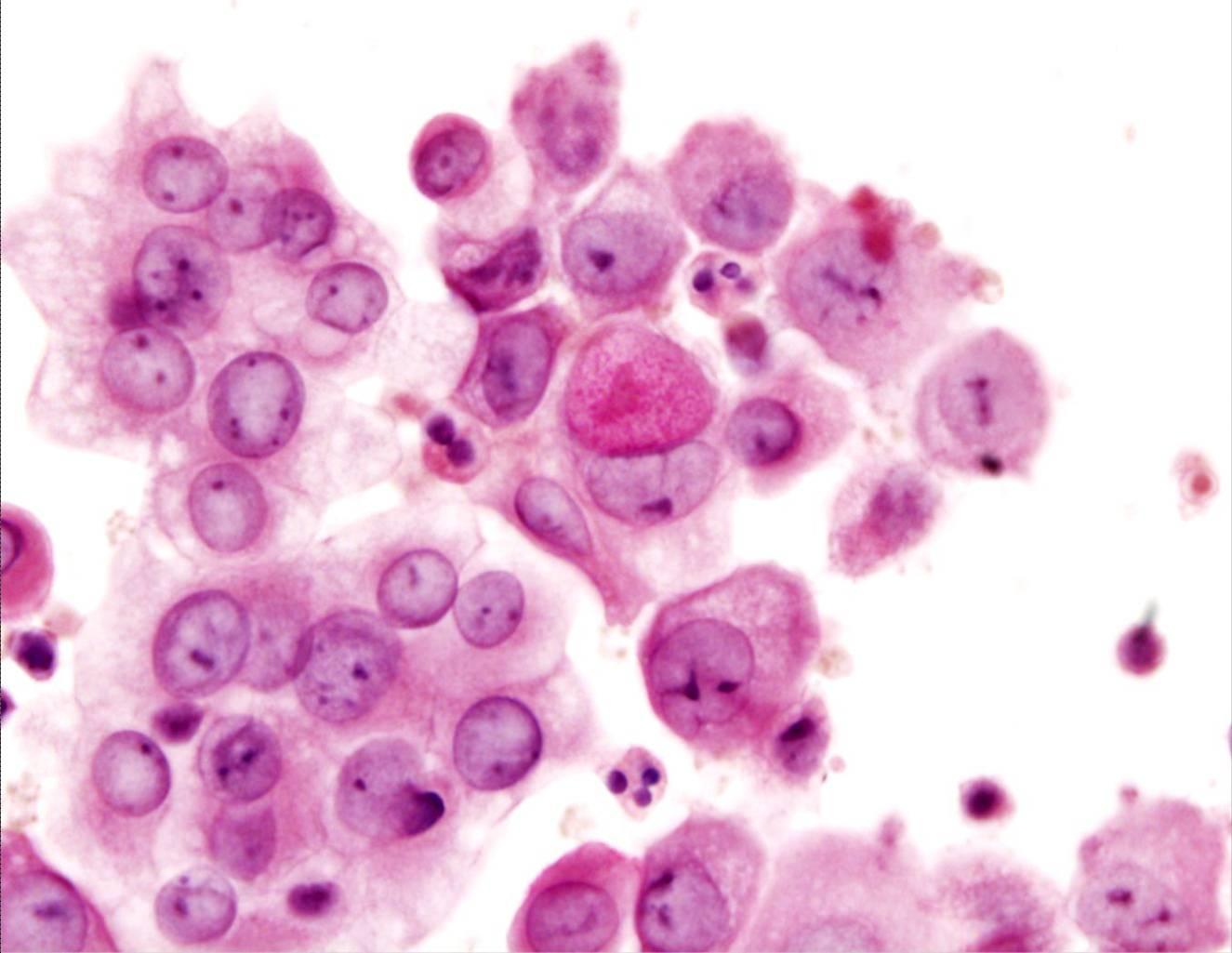
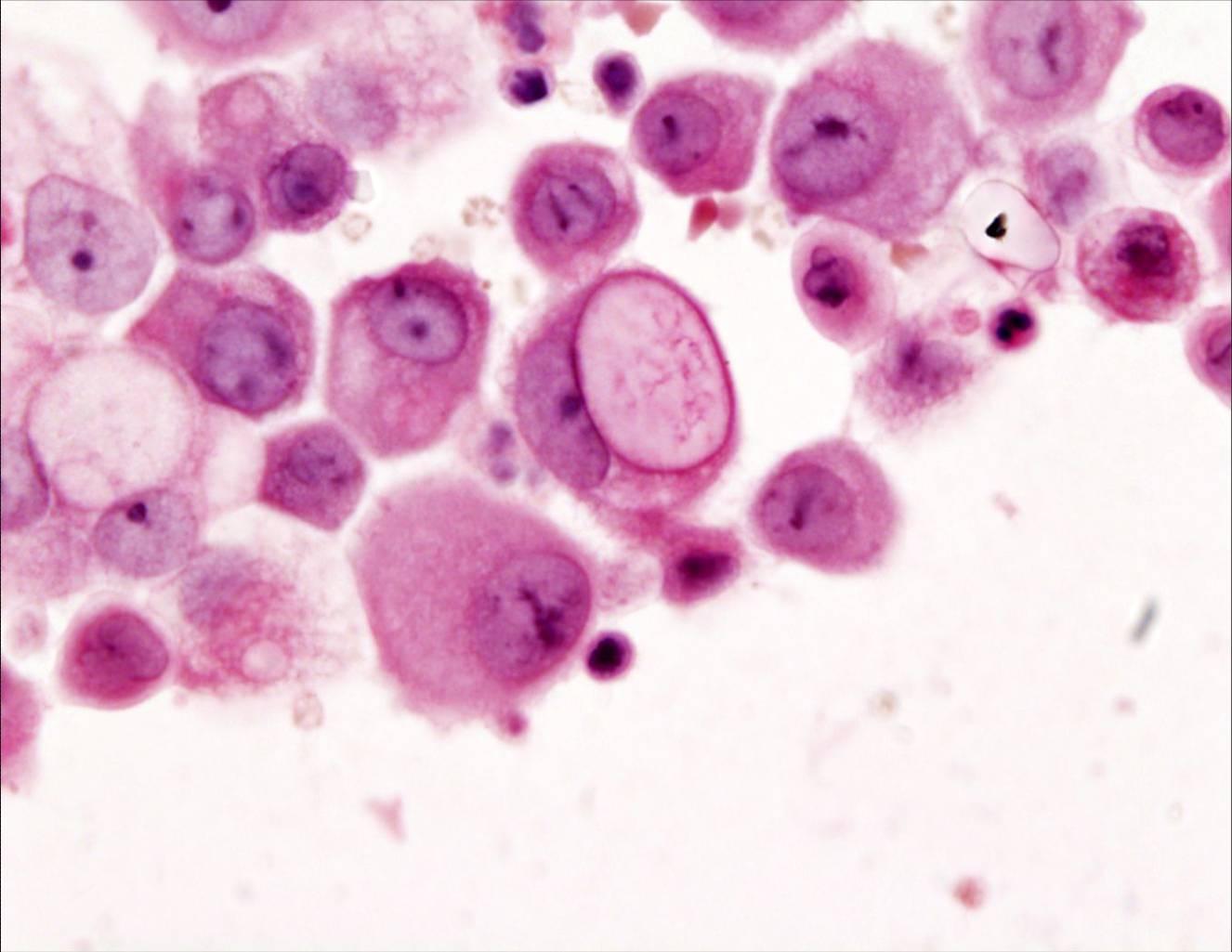
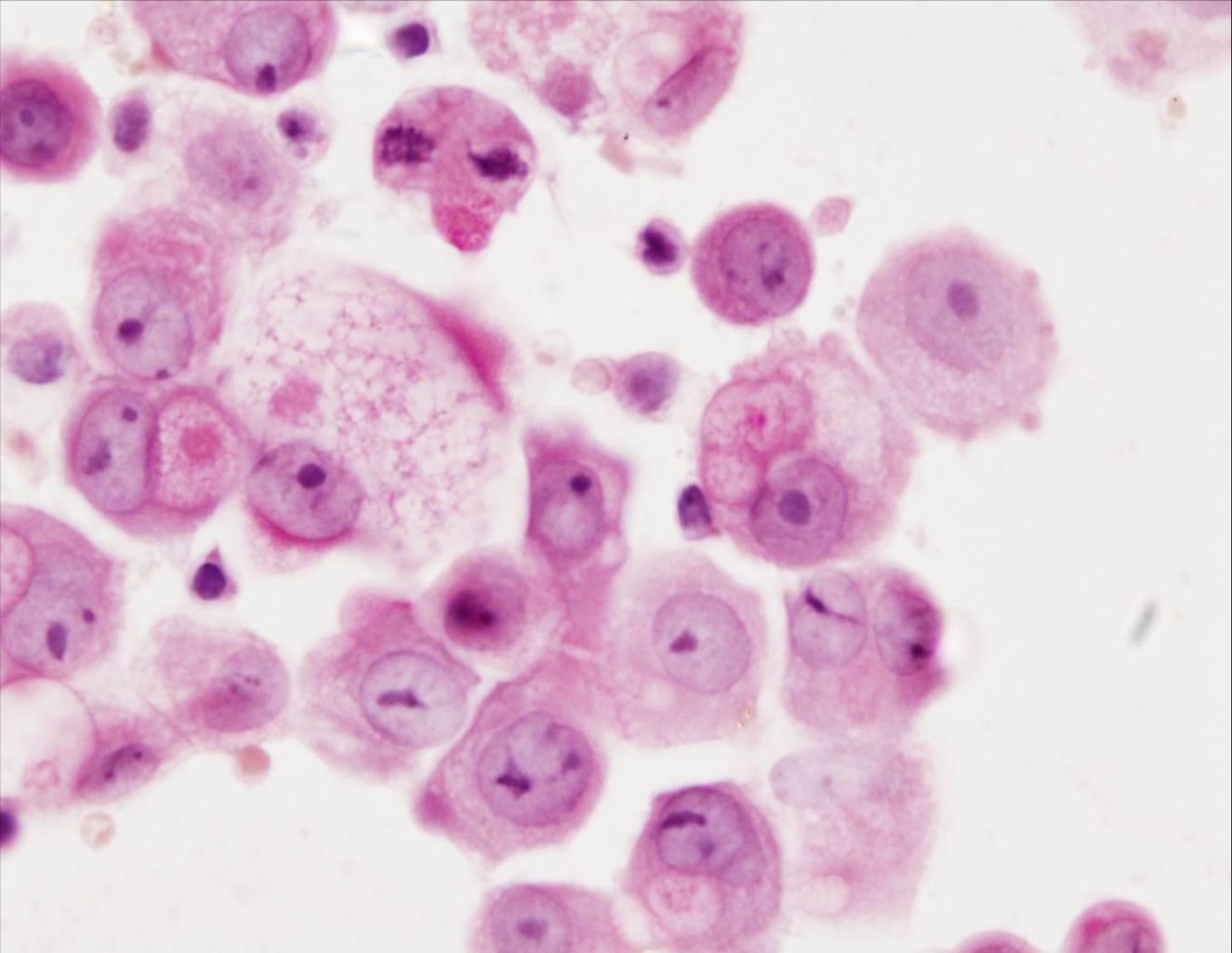
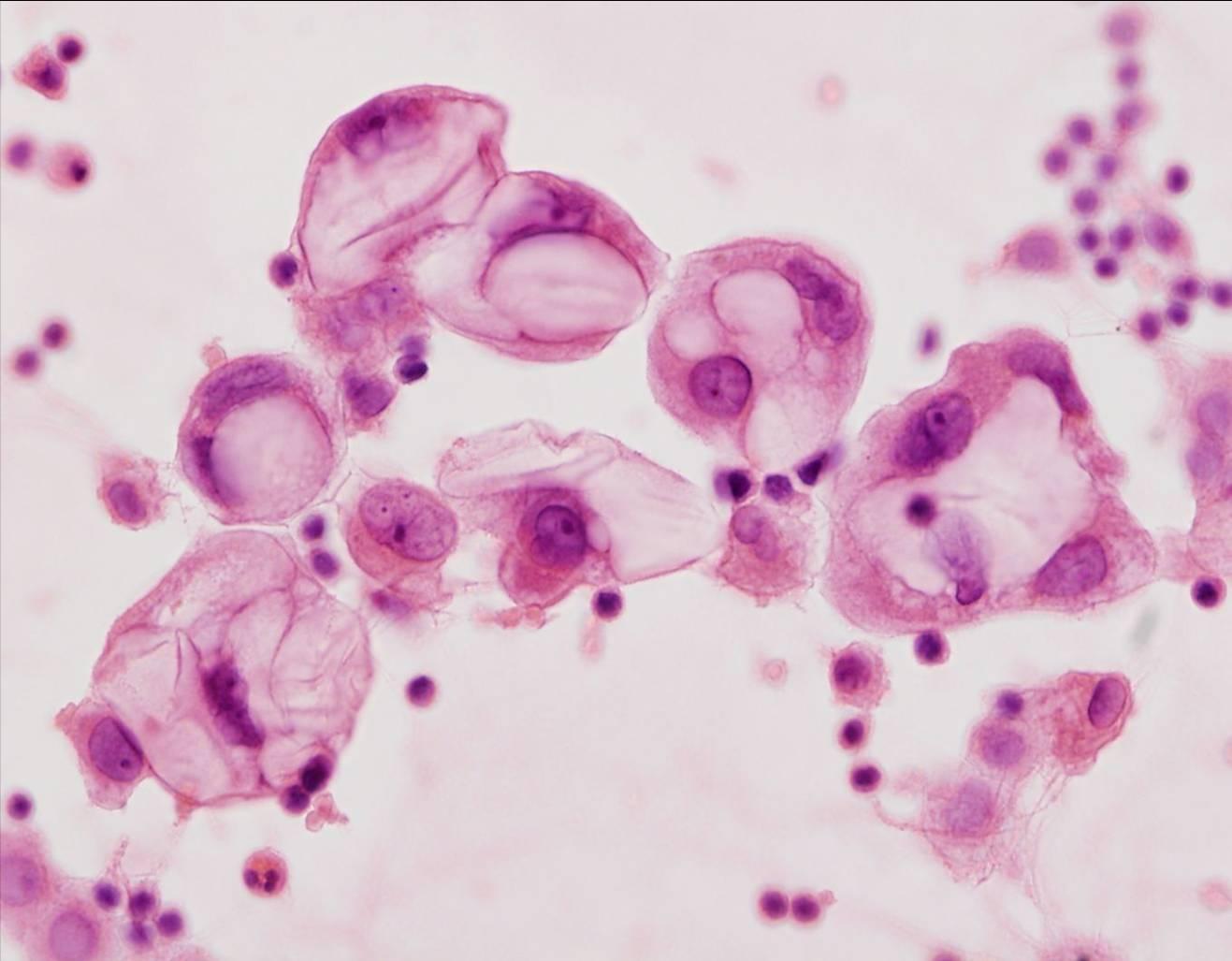
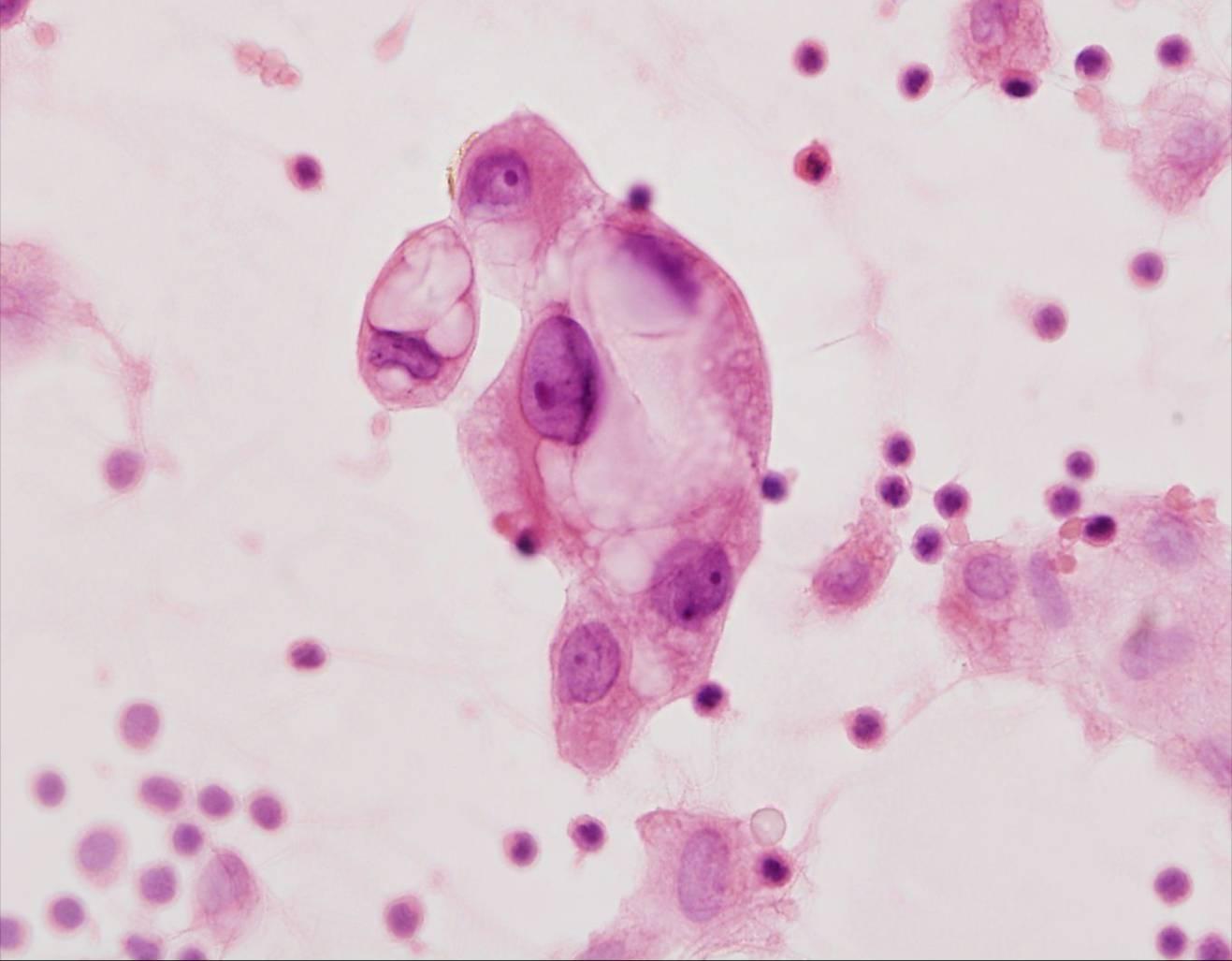
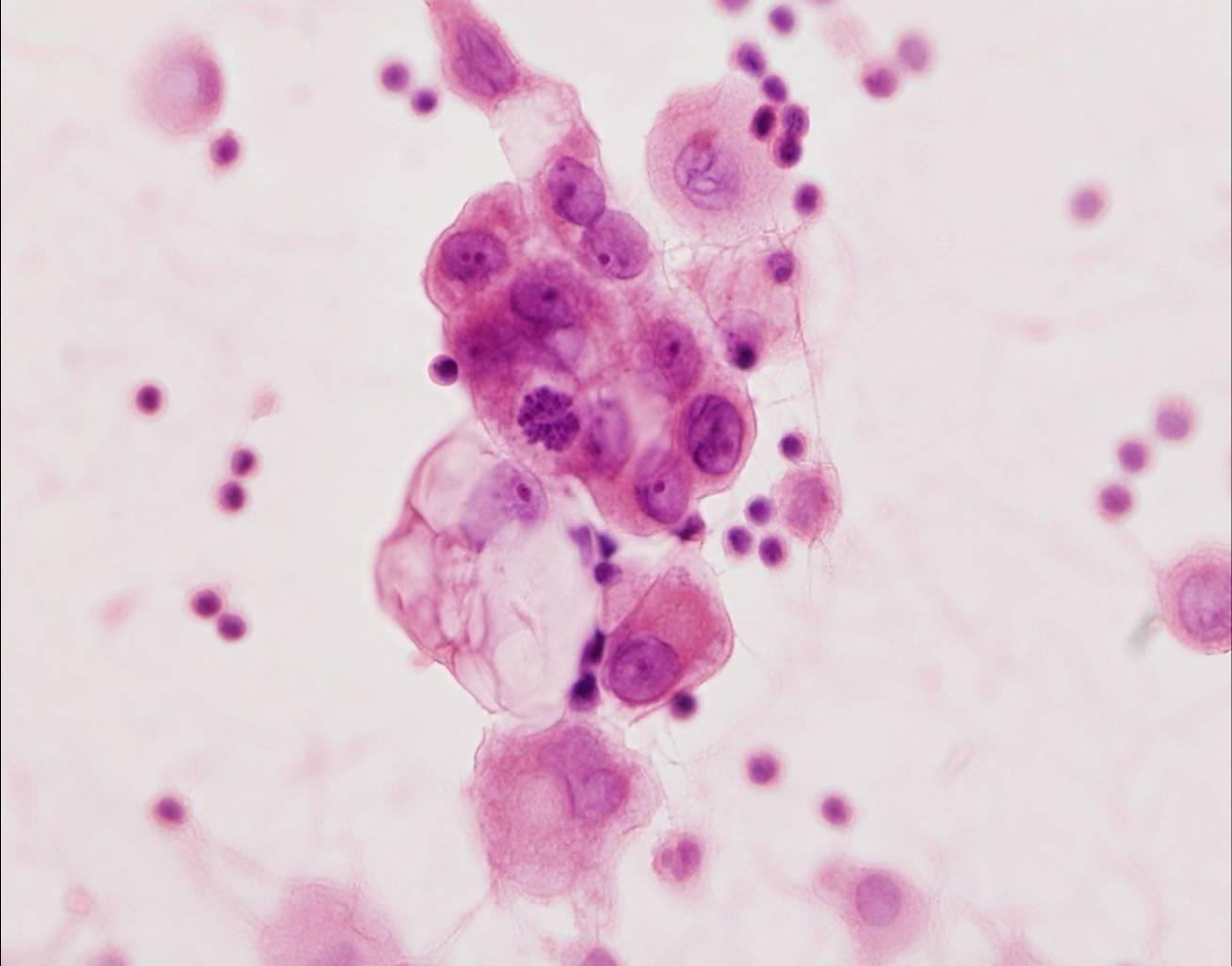
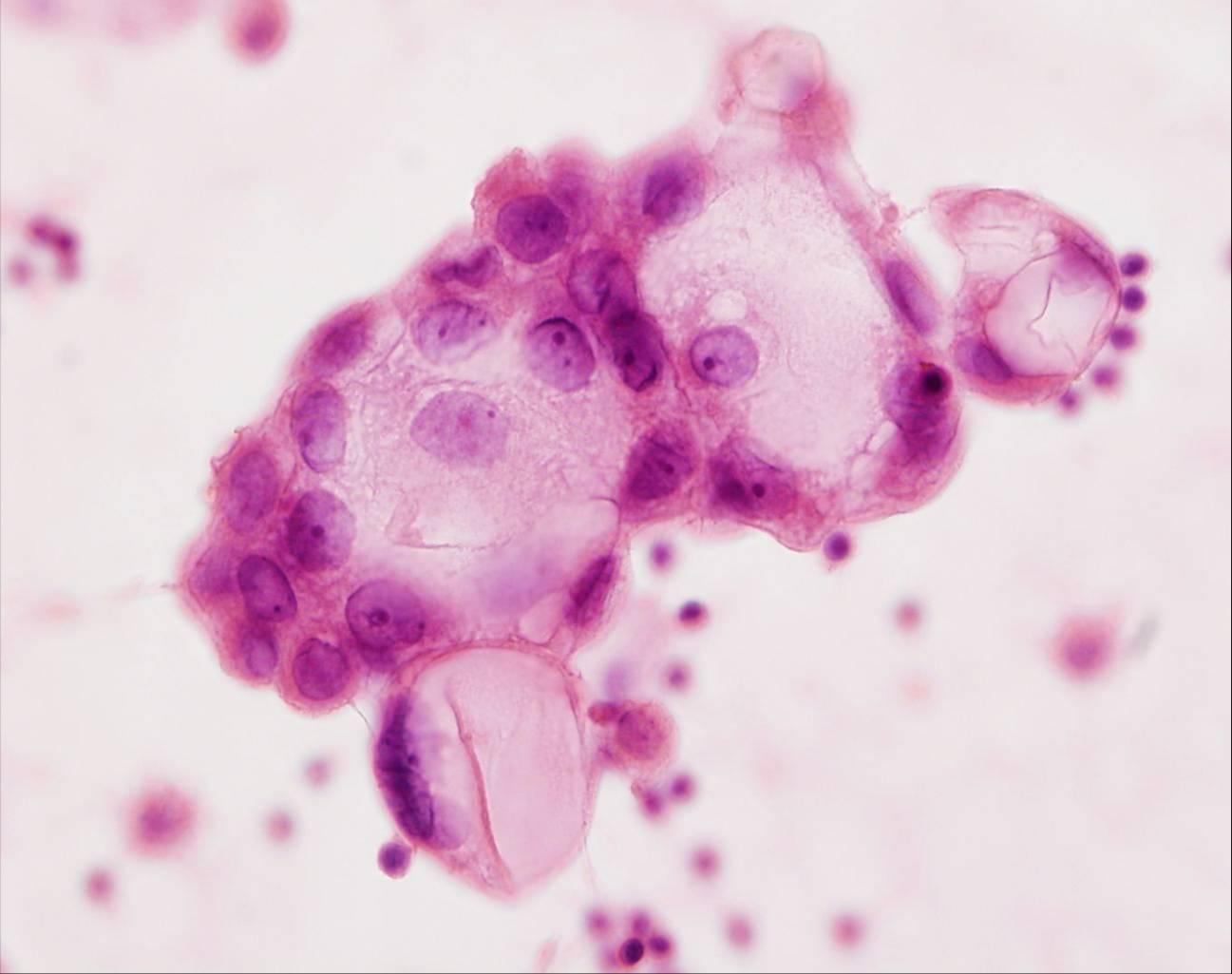
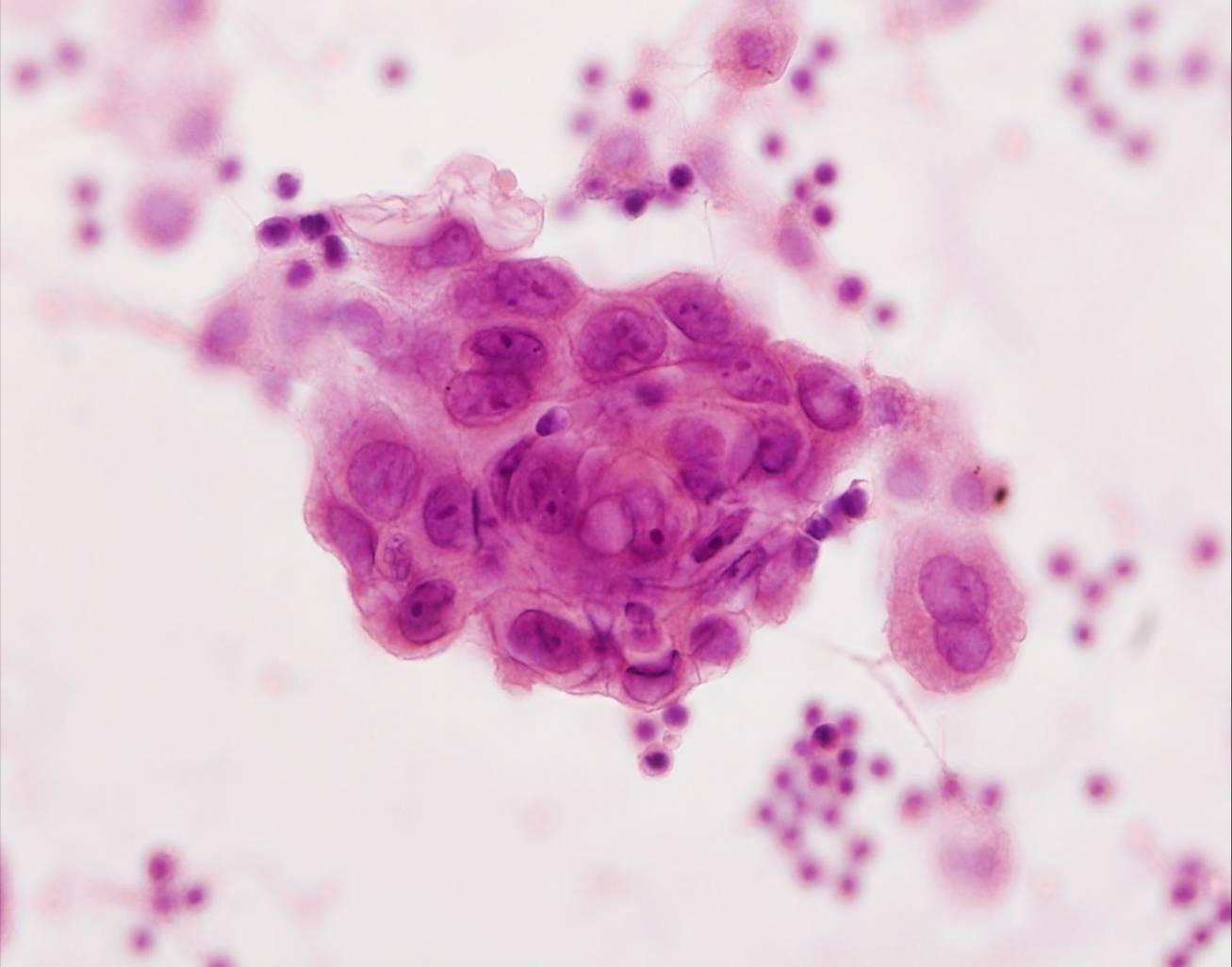
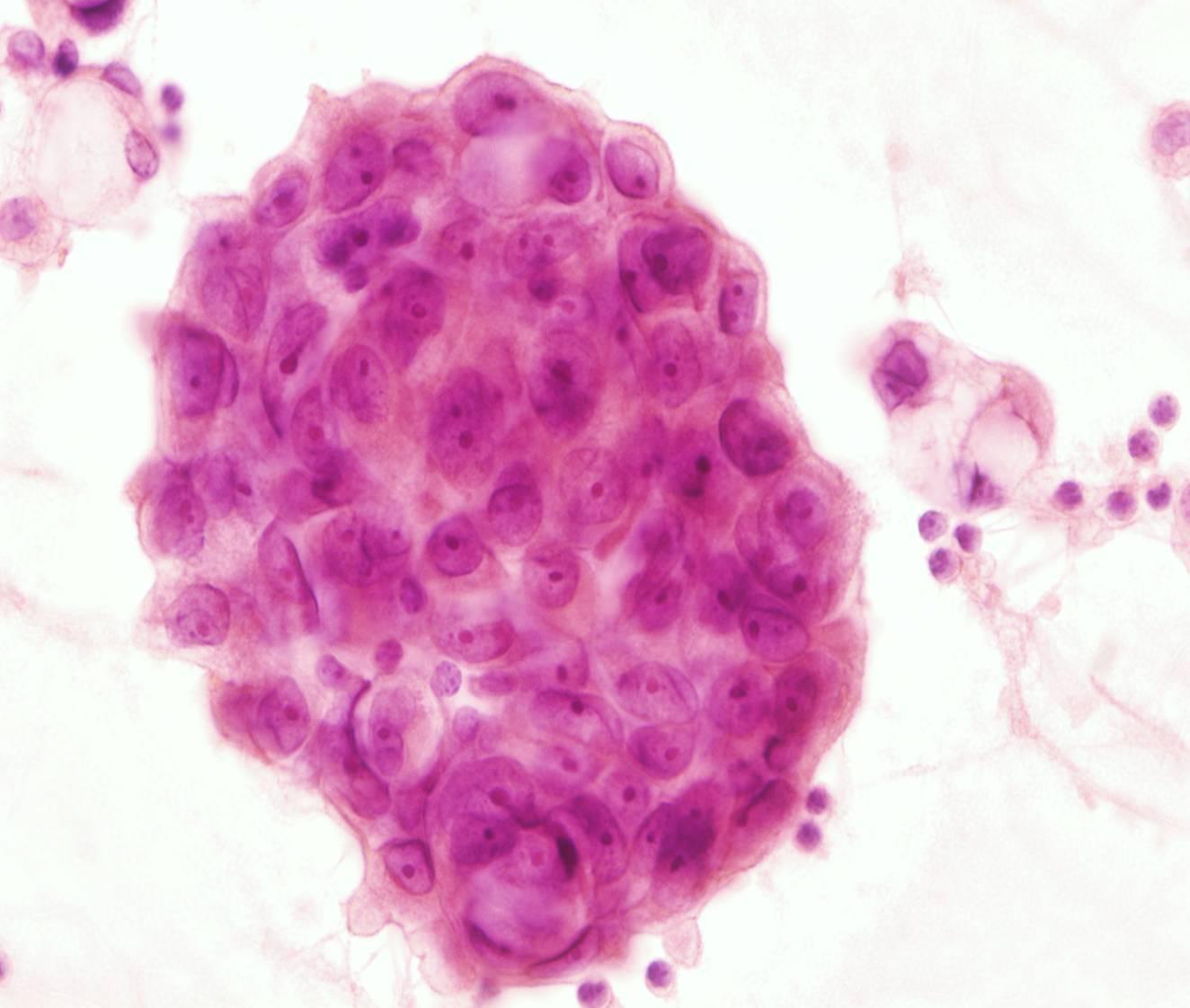
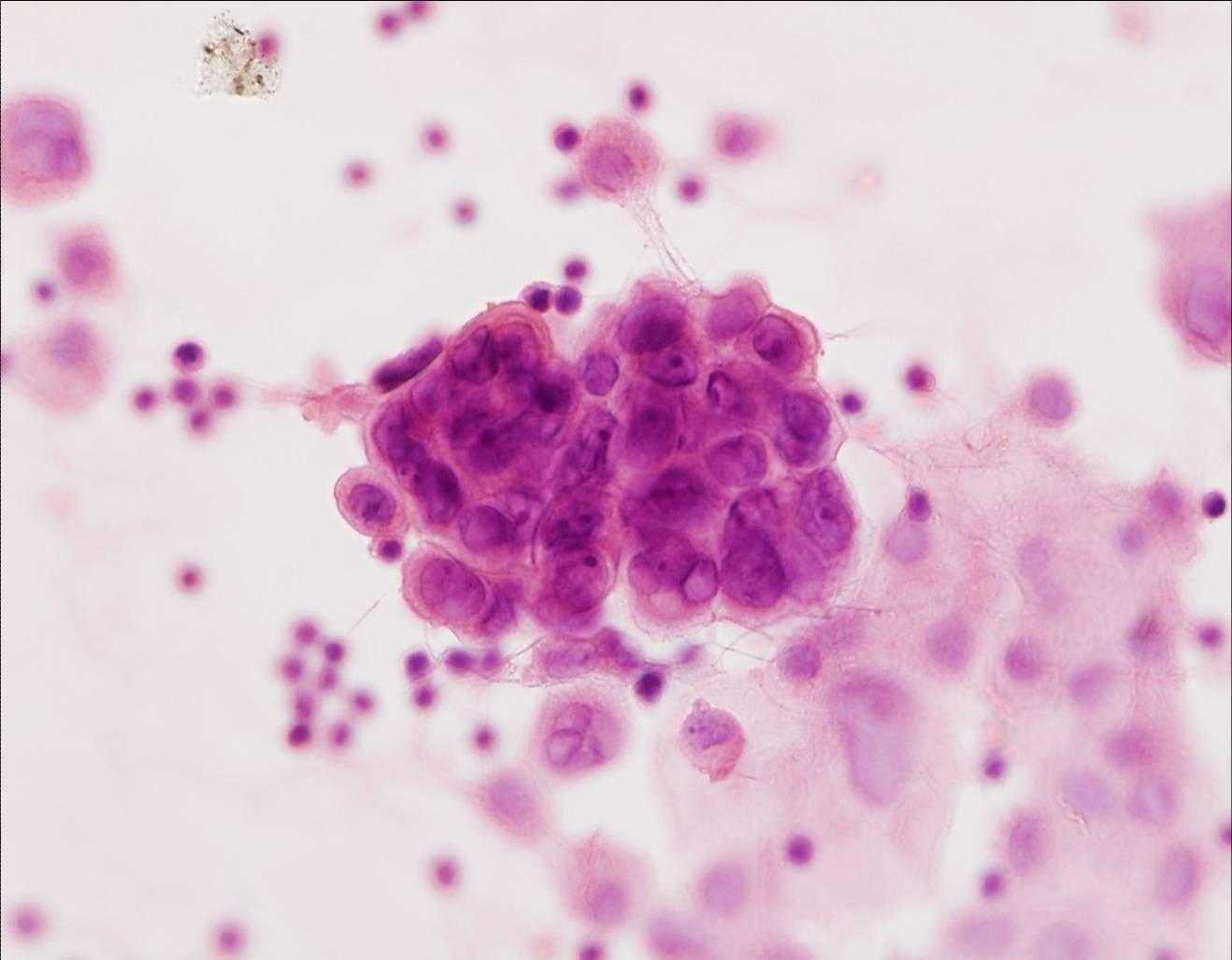
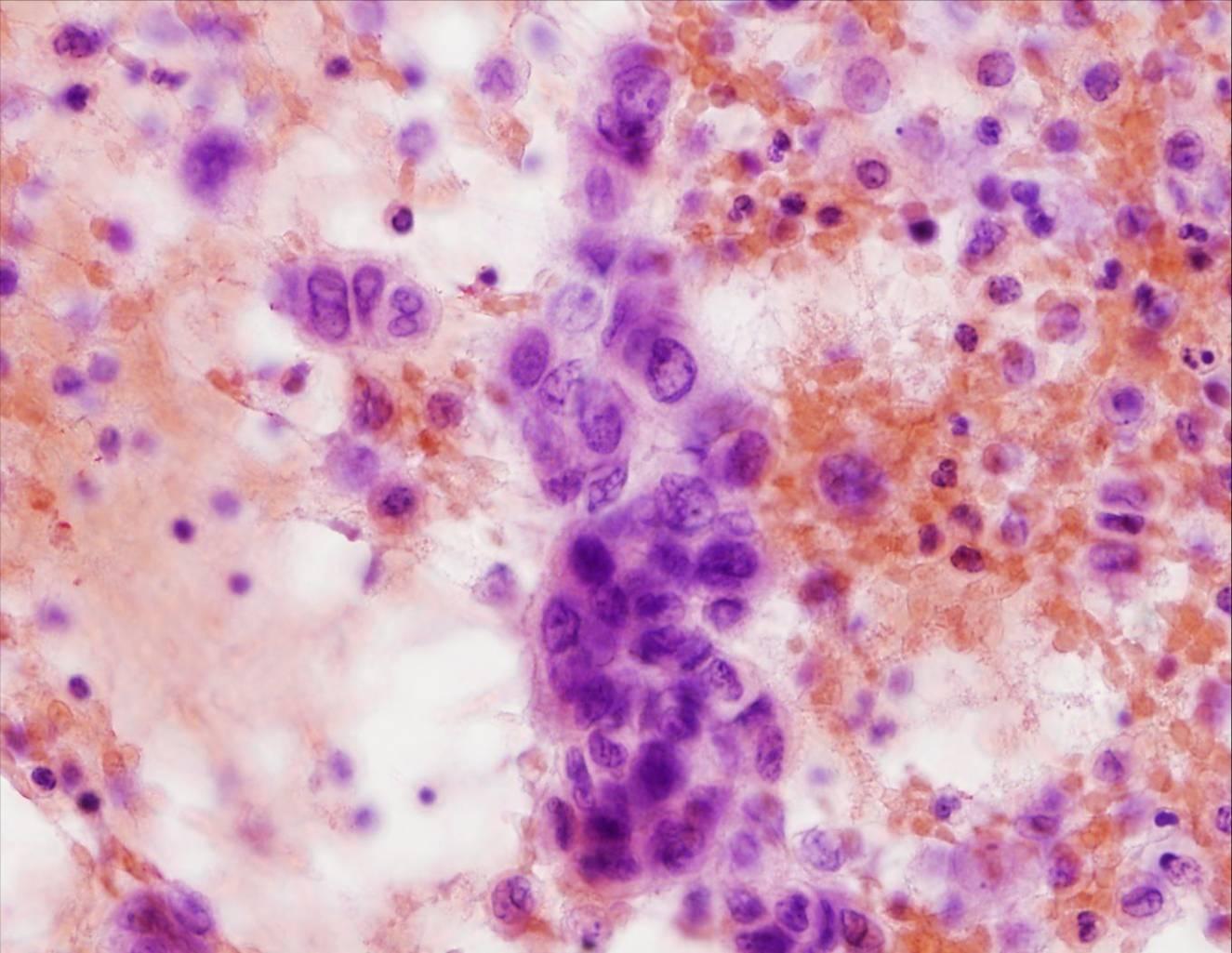
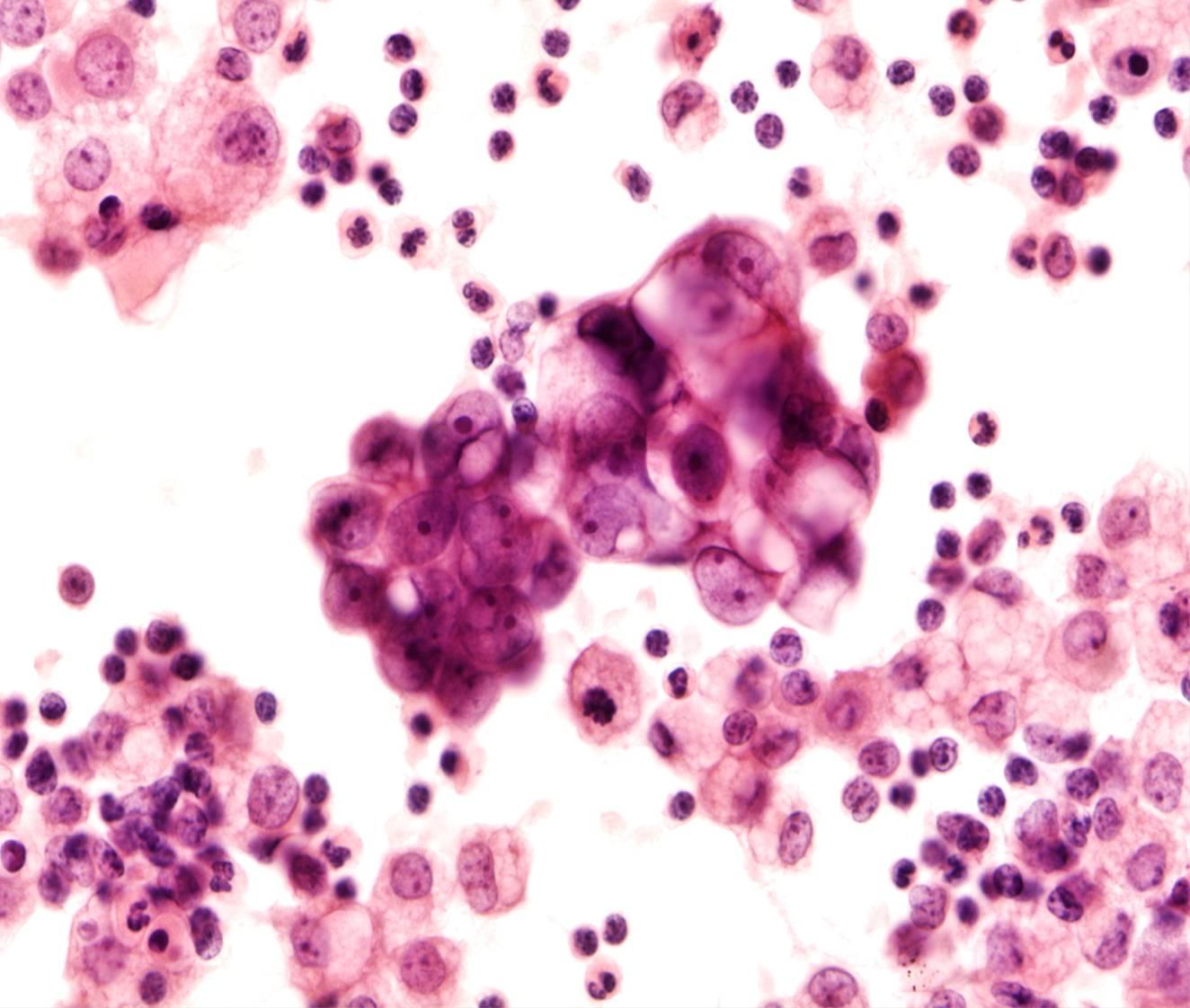
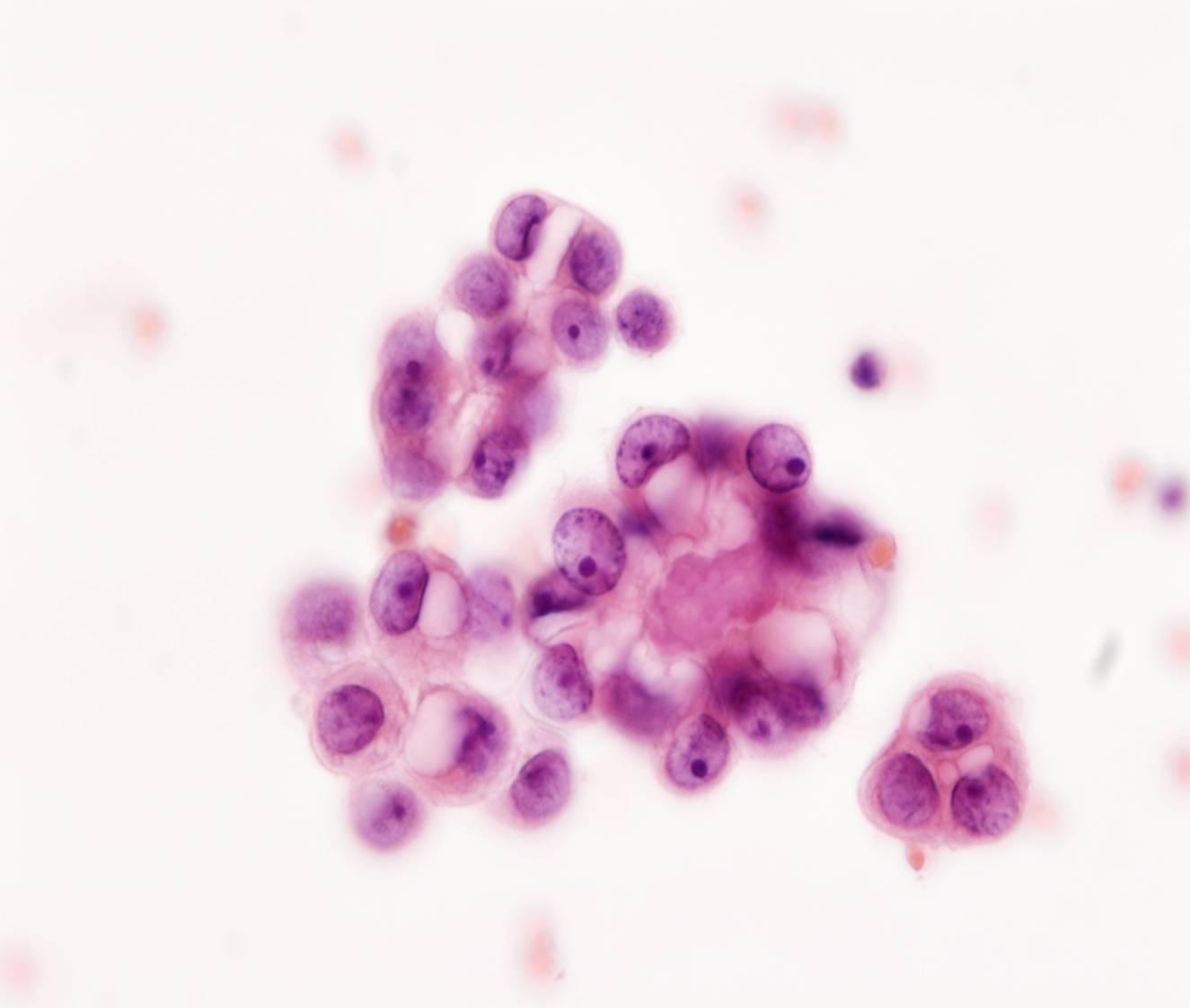
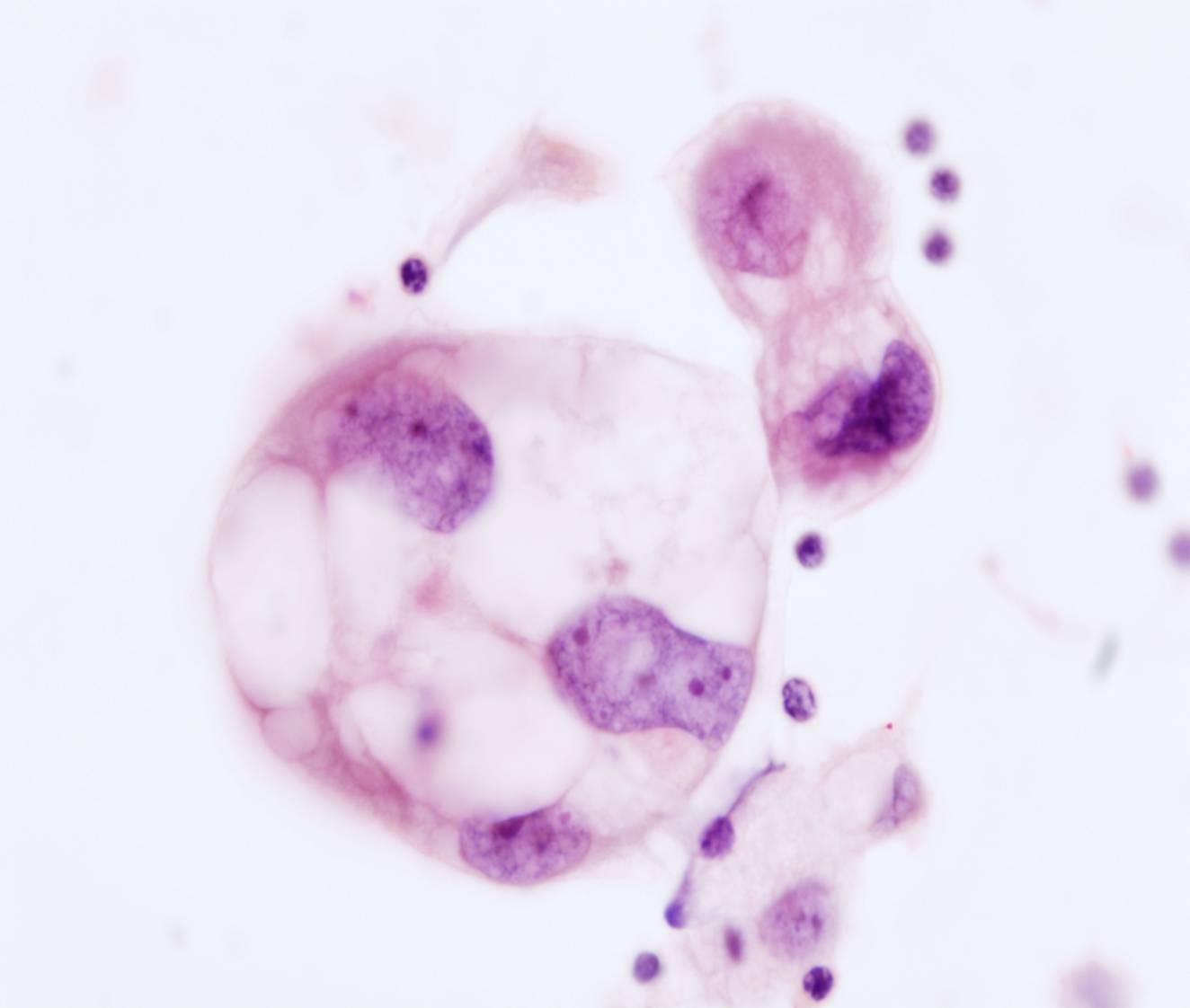
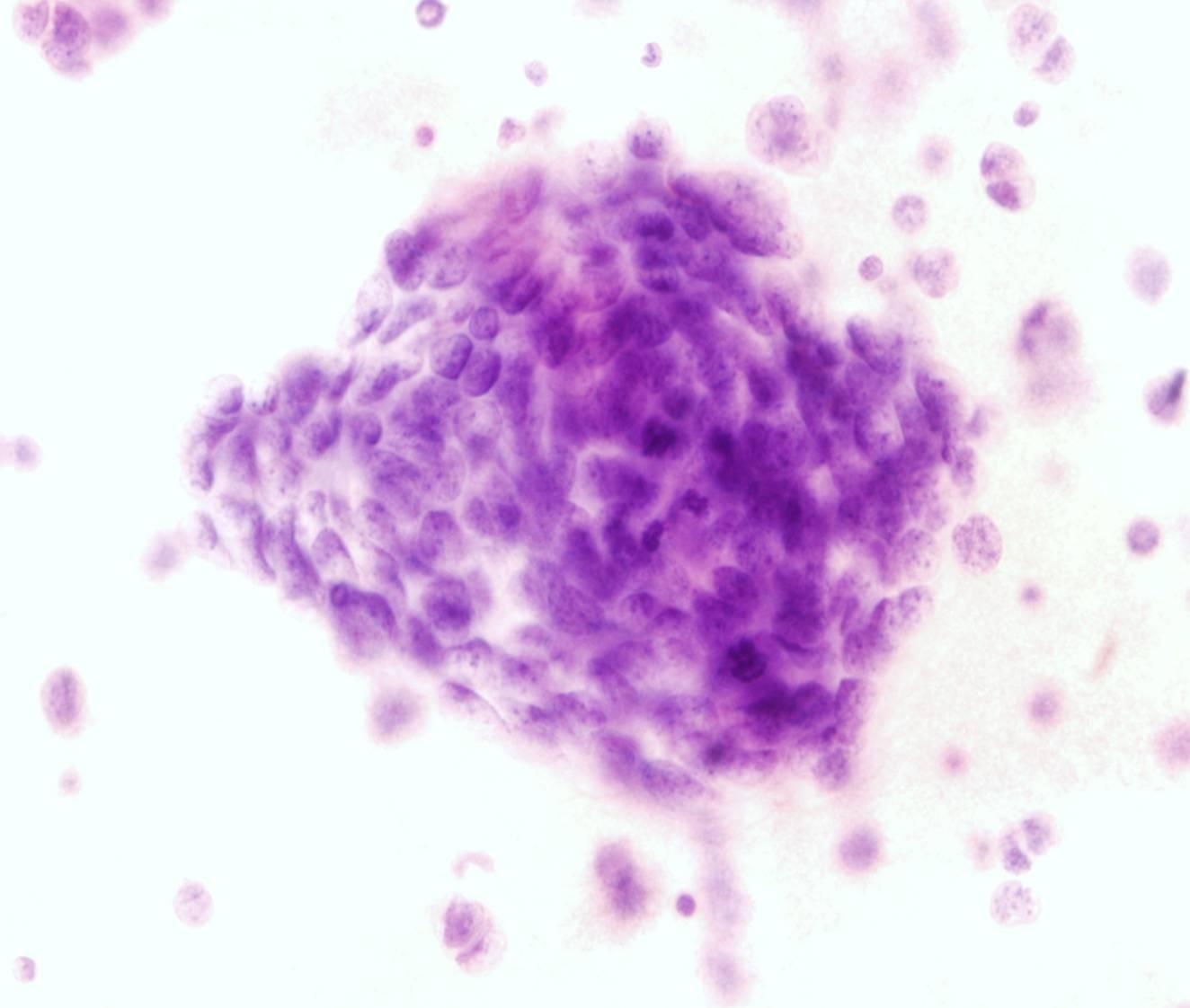
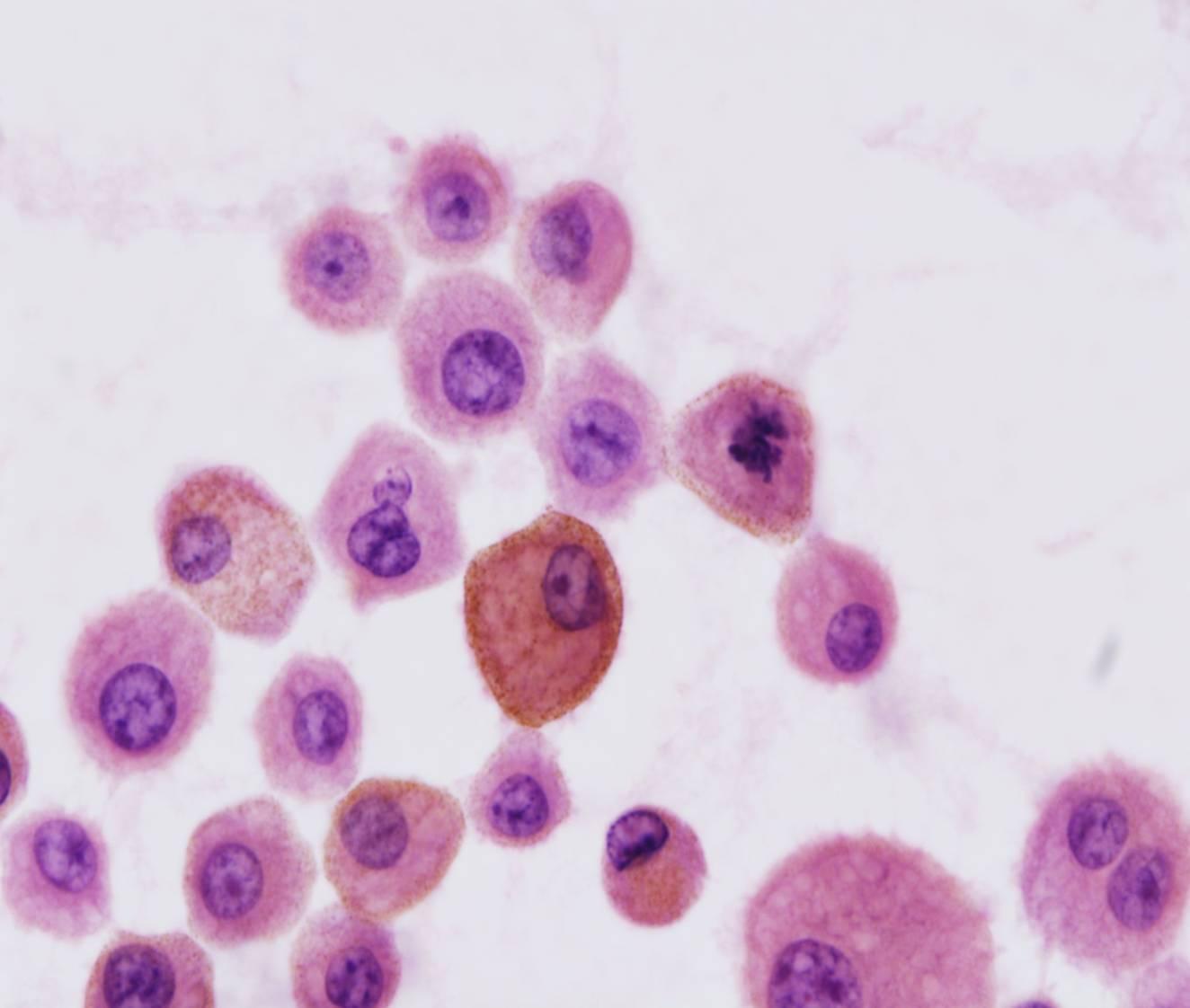
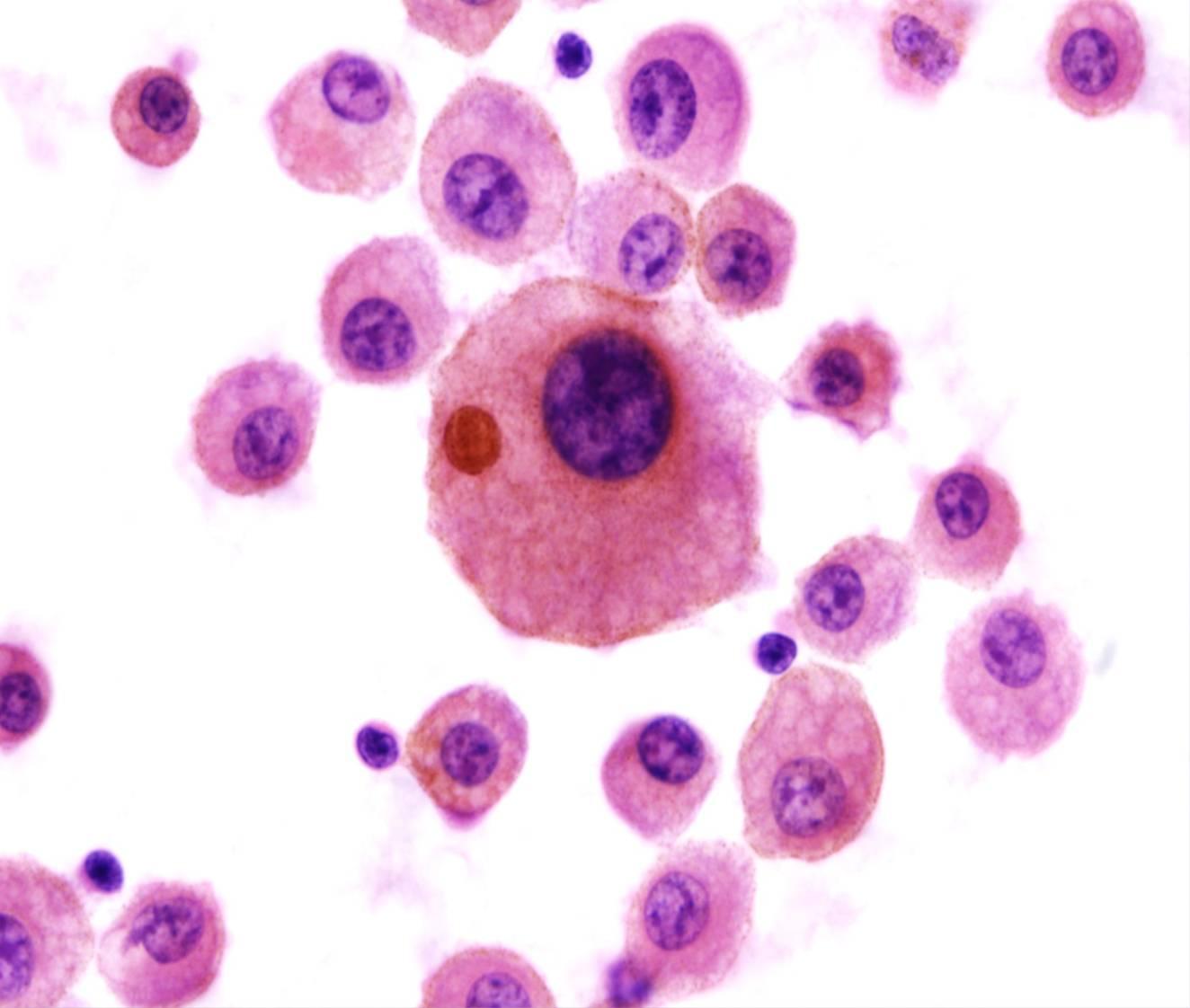
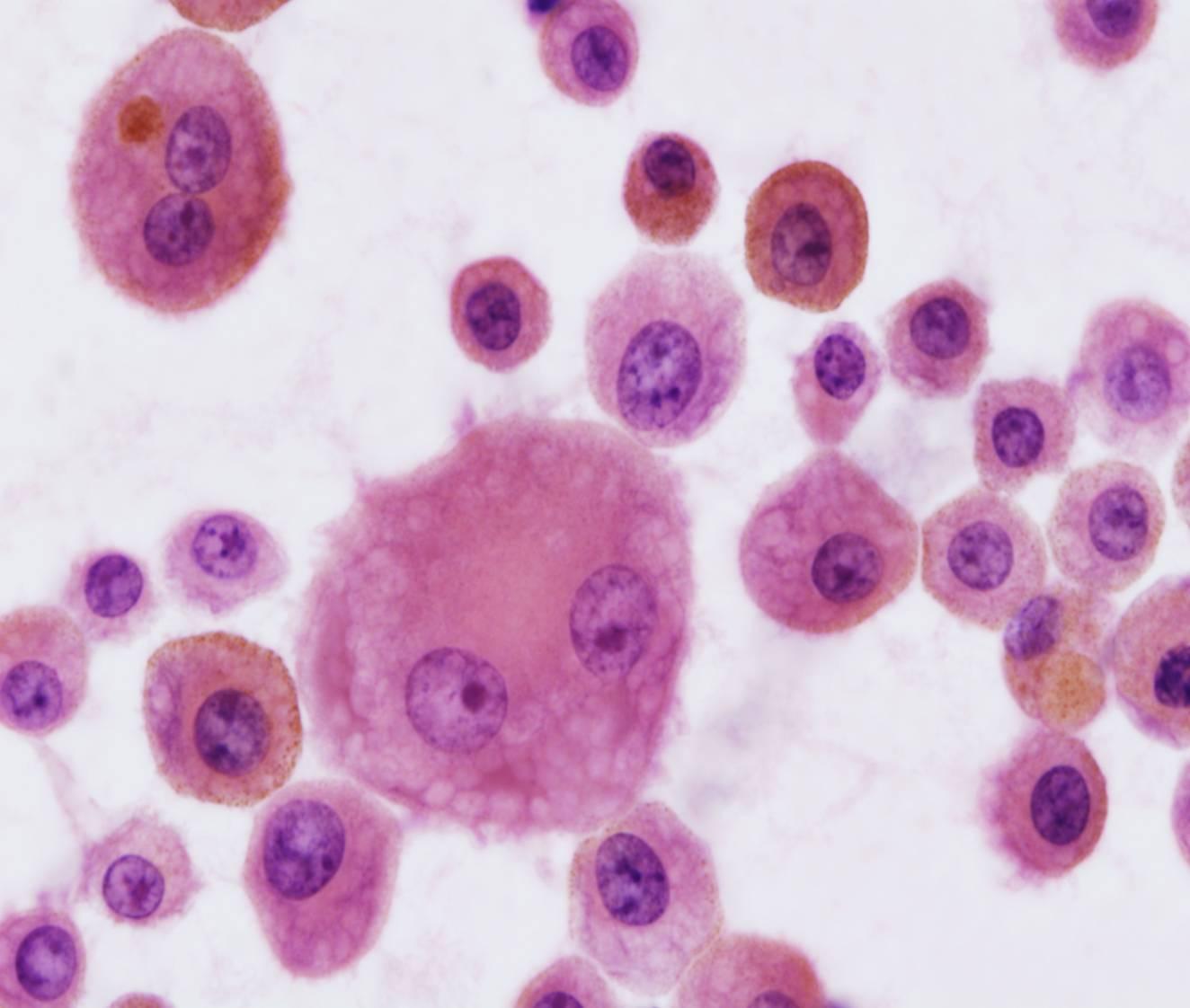
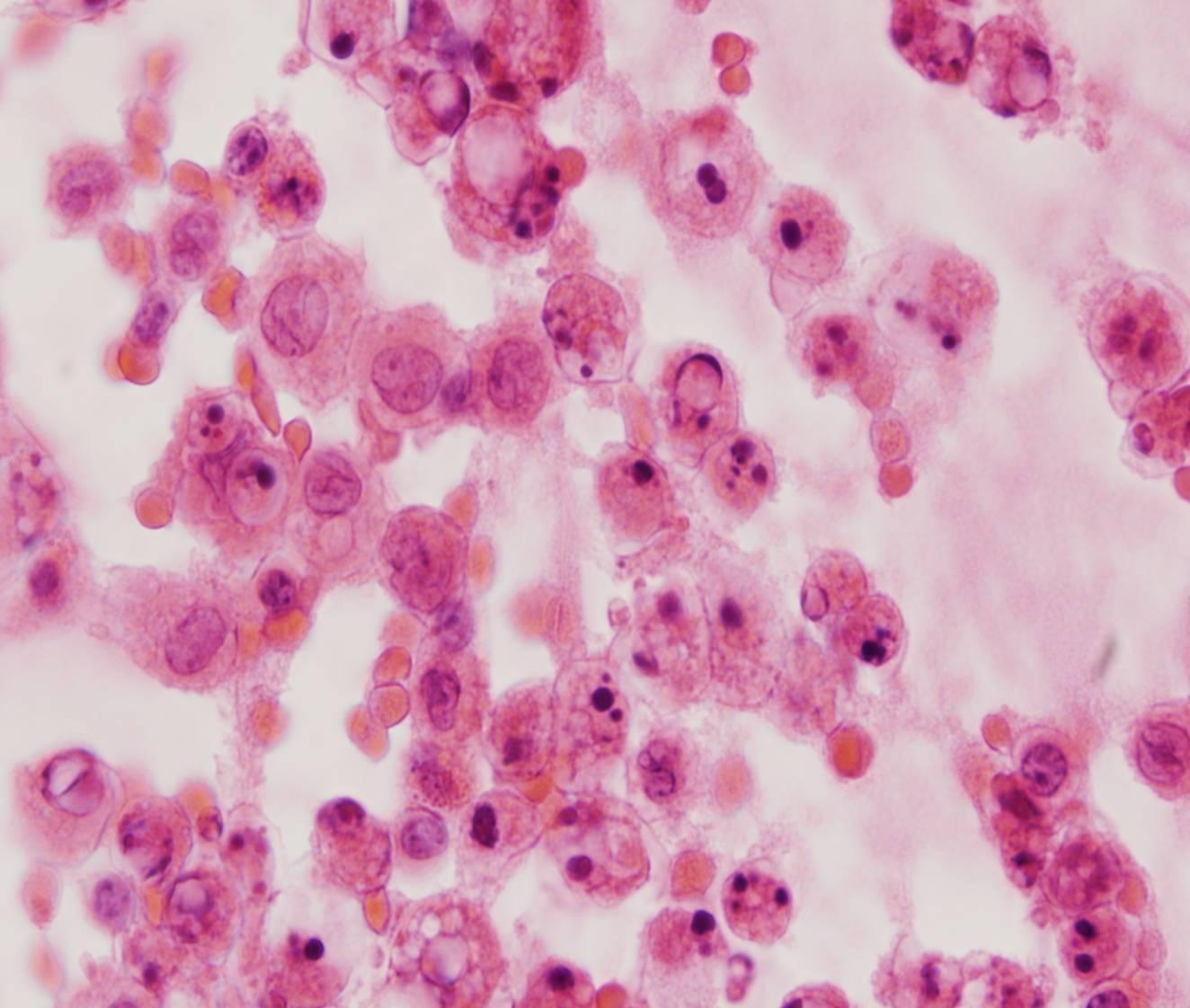
Adenocarcinoma
- Large spheres or single cells
- Cytoplasmic vacuolization
- Signet ring cells (gastric, breast)
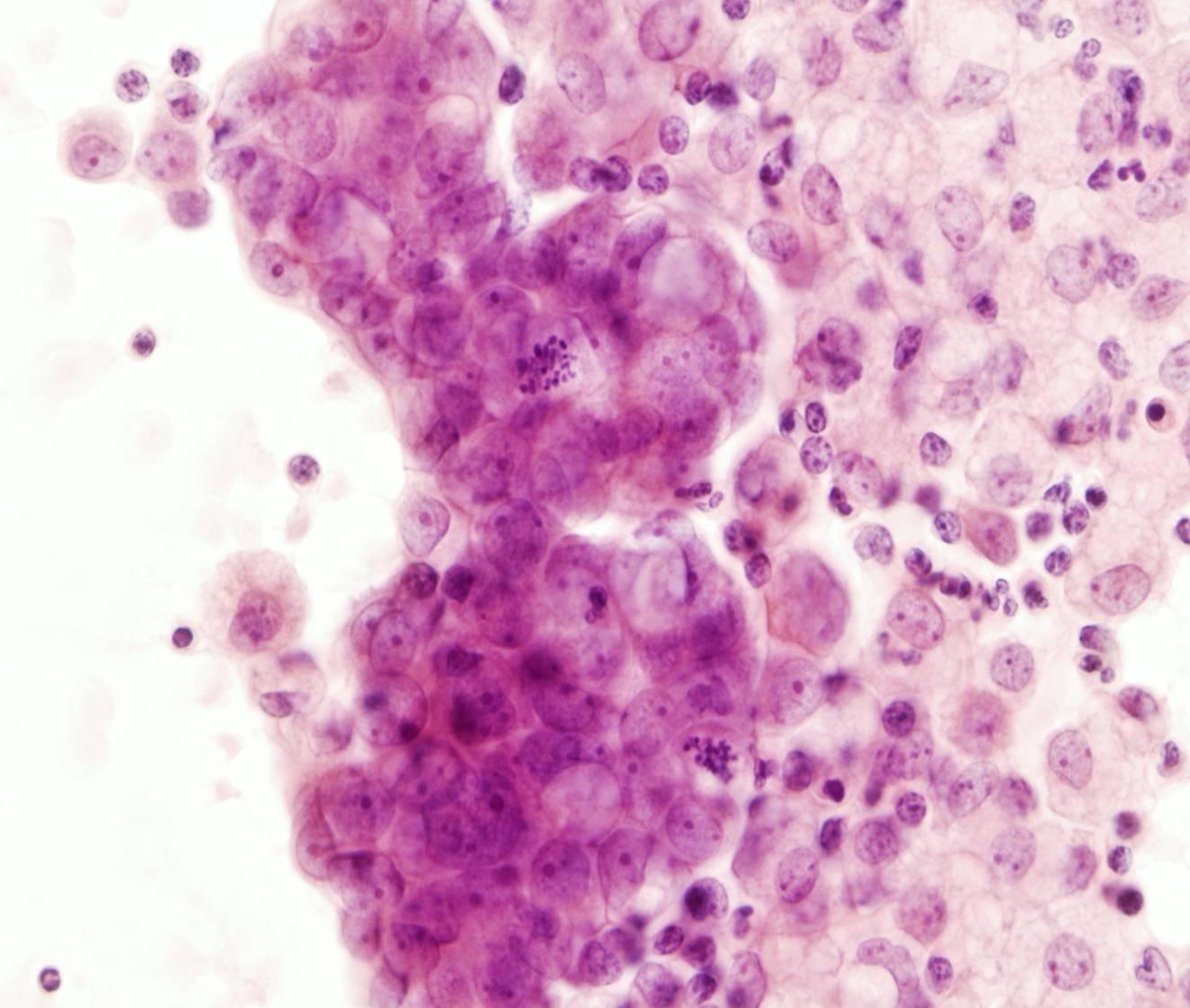
Breast, lung, ovary and stomach are the most common primary sites. Some morphologic features can point to the site of origin of an adenocarcinoma. For example, abundant hollow spheres (cannonball) are a common pattern in metastatic breast cancer (ductal carcinoma). Such ‘proliferation spheres’ may also be present in metastatic ovarian carcinoma as well as in small cell lung carcinoma. Signet ring cells are common in metastatic gastric carcinomas. Most colorectal cancers are composed of elongated cells with hyperchromatic nuclei arranged in acinar formations, often with individual cell necrosis. Large cells with prominent nucleoli and abundant lacy, vacuolated cytoplasm are typical of clear cell carcinomas of the kidney and the female genital tract. Psammoma bodies are observed in effusions caused by serous carcinomas of the ovary, fallopian tube and endometrium, papillary carcinoma of the thyroid, adenocarcinoma of the lung. They are also seen in mesothelioma and in some benign proliferations of the mesothelium. Groups of cells with cytoplasmic vacuolization are typical of metastatic ovarian carcinoma and lung adenocarcinoma. Mucinous tumours, particularly of the ovary and appendix, produce abundant extracellular mucin, which markedly distends the peritoneal cavity (pseudomyxoma peritonei). The fluid is gelatinous and composed predominantly of mucin, which stains blue-green or purple with the Papanicolaou stain. The specimens are often sparsely cellular, containing only vacuolated histiocytes; the tumor cells, columnar and hyperchromatic, are not seen in many cases.
It is usually easy to distinguish malignant cells from reactive mesothelial cells. In block sections malignant cells are often arranged in large clusters or situated in lacunae. In some cases, metastatic adenocarcinoma cells may be hard to recognize, when either a second population of benign mesothelial cells is absent or the tumour cells resemble mesothelial cells very closely. Lobular carcinoma of the breast can be particularly difficult to recognize. Special stains for mucin, CEA and Leu-M1 are useful: most adenocarcinomas are positive, whereas mesothelial cells are negative.
Immunohistochemical markers are also useful in patients with tumours of unknown primary.
A large panel is suggested including mesothelial markers Calretinin, WT1, CK5 and D2-40 and epithelial relatively organ specific markers like TTF1 and Napsin A (Lung), ER, PgR and HER2 (Breast), CK20 and CDX2 (GI), PSA, PAP and P504S (Prostate), CD10 and Vimentin (Kidney) WT1 and ER (Ovary).



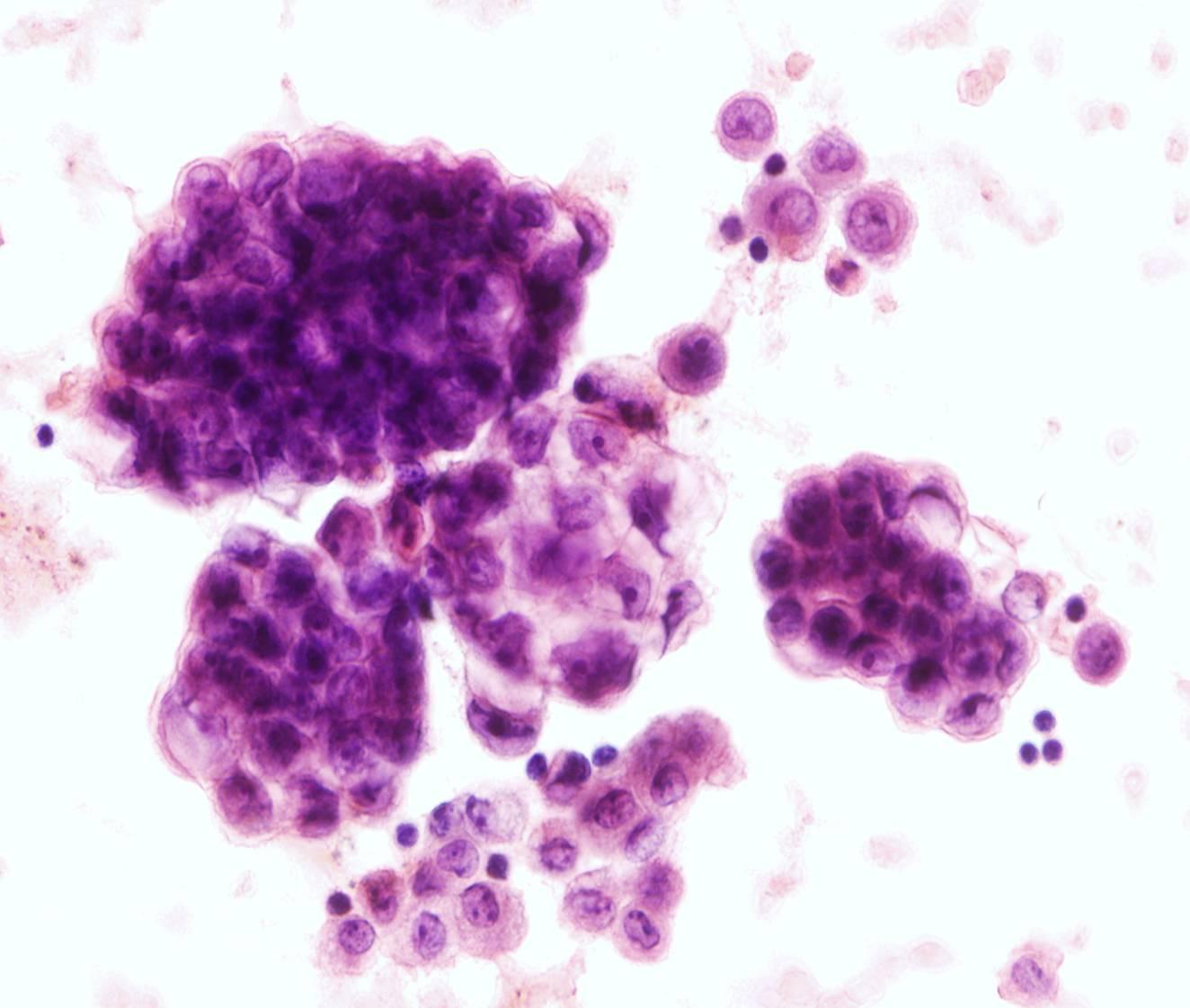
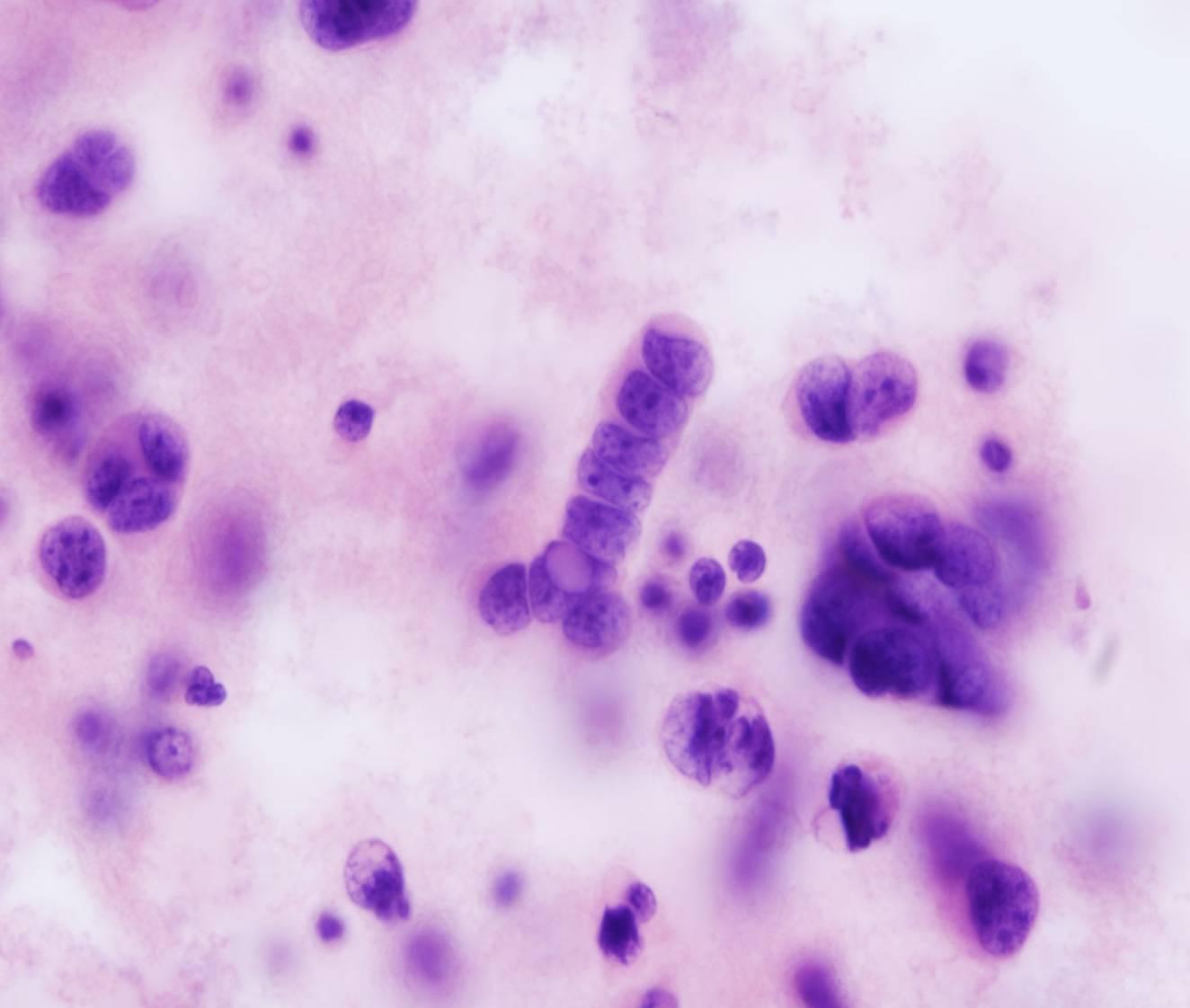
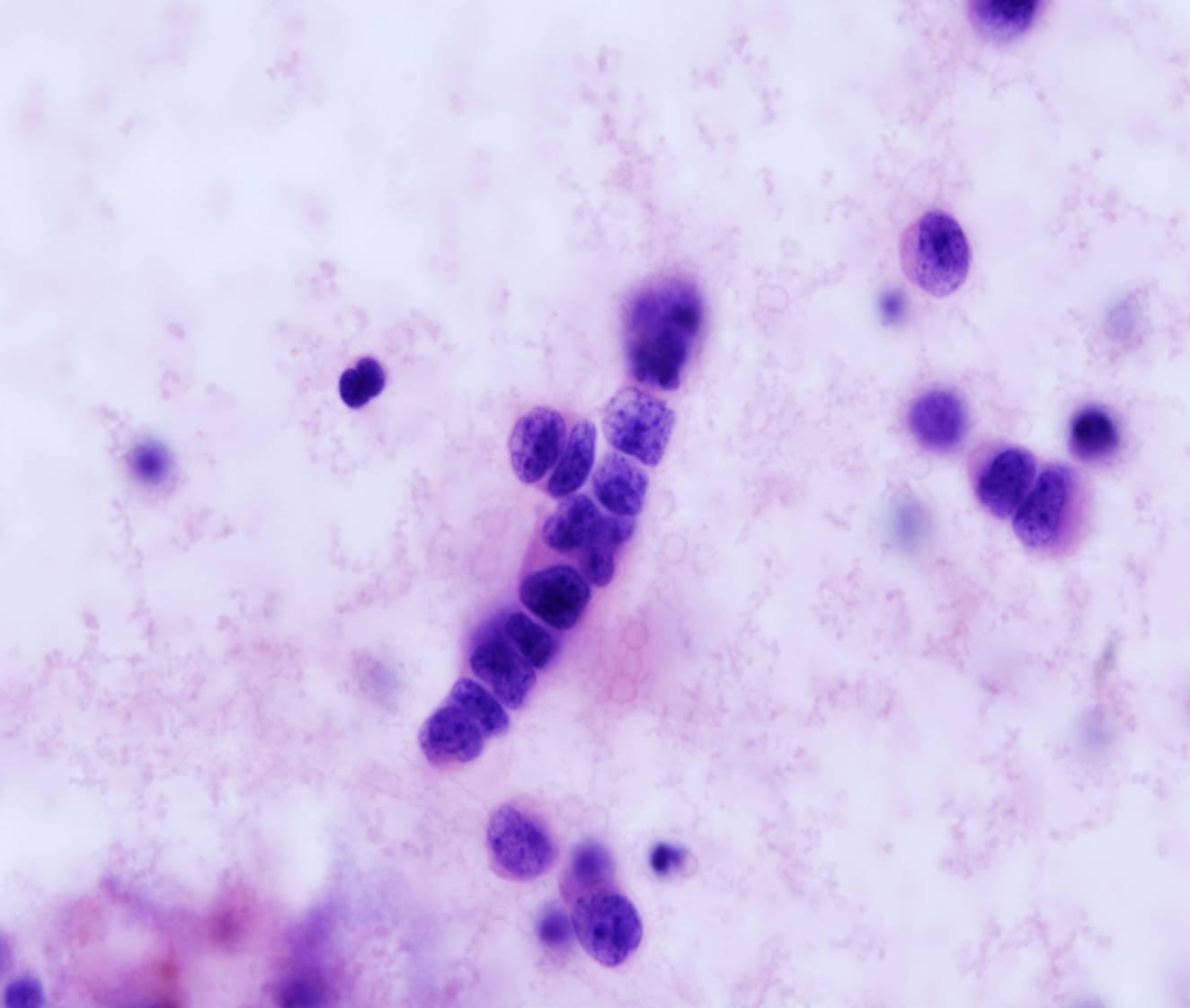
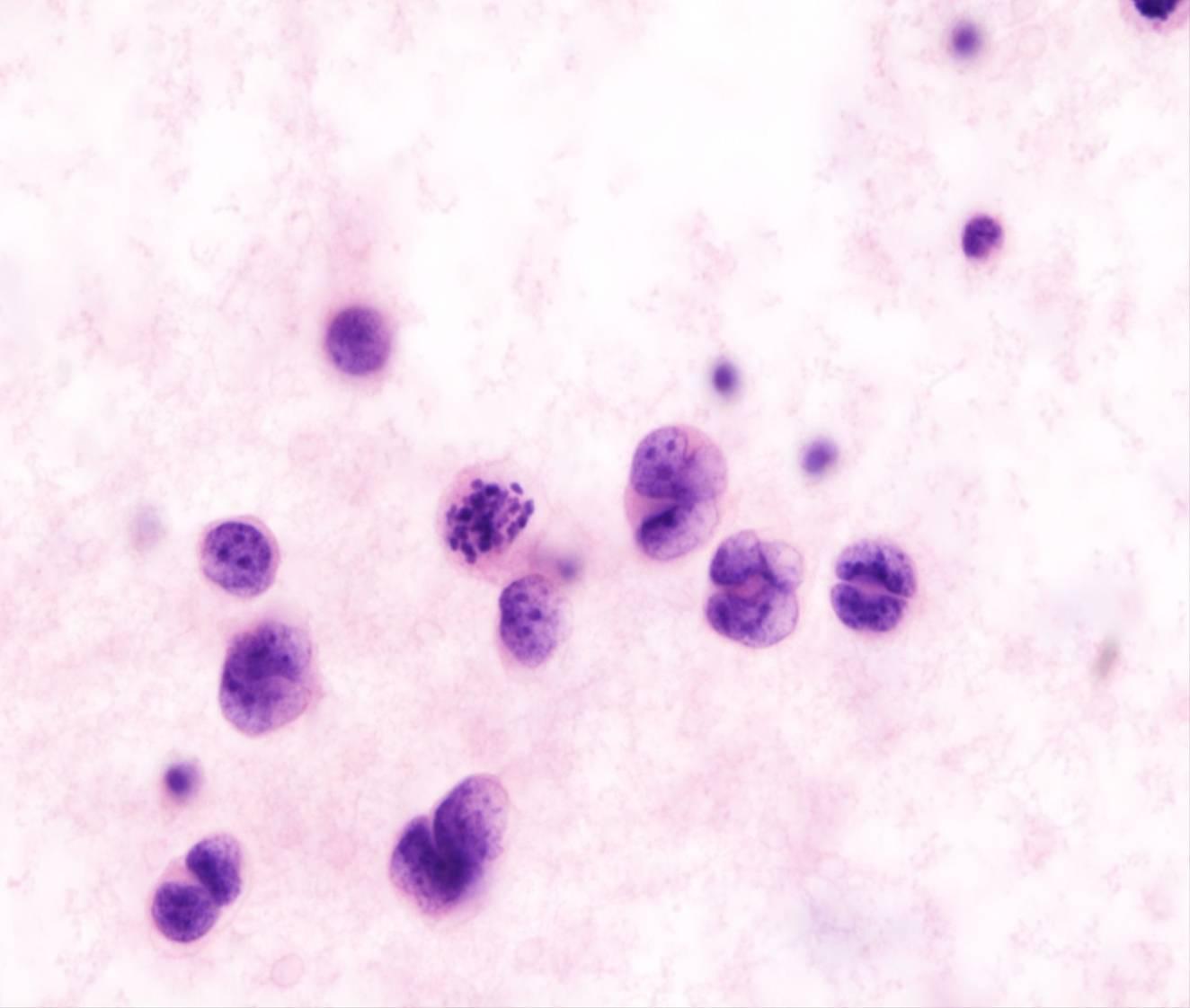
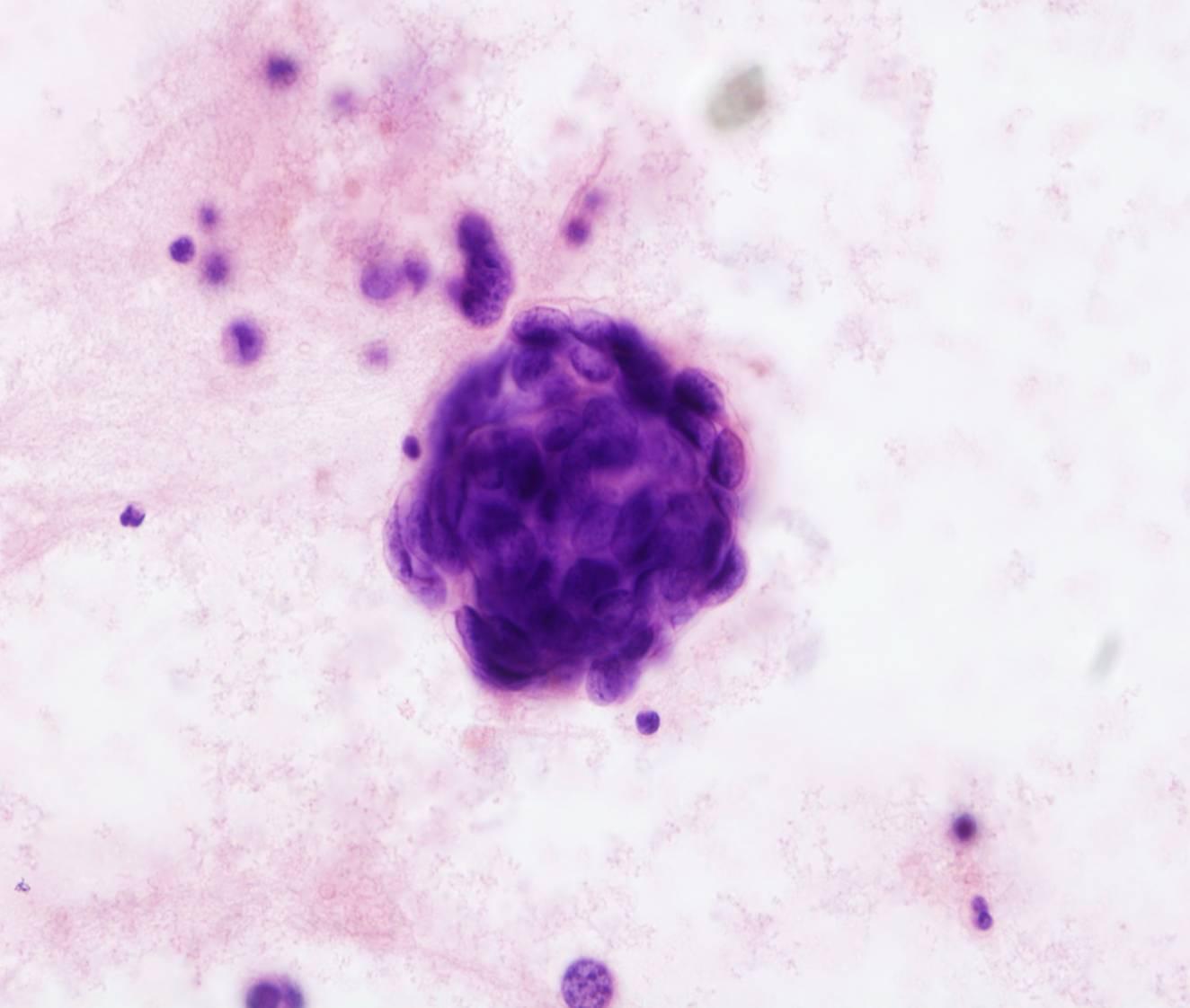
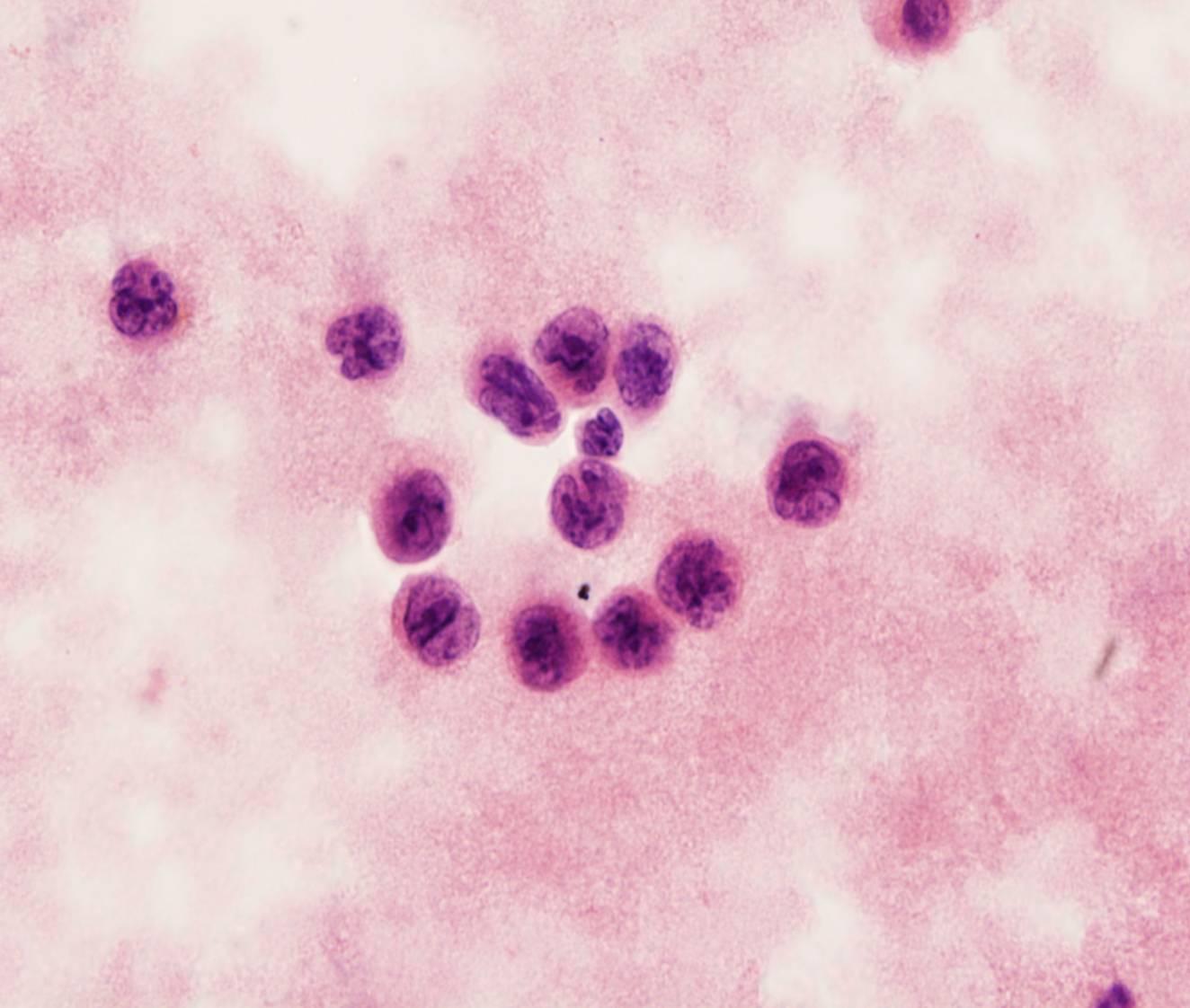
Small cell carcinoma
- Isolated cells and cohesive clusters
- Chains of tumour cells with side arms coming off at various angles
- Nuclear moulding
- Scanty cytoplasm
- Mitoses
This cytologic appearance is characteristic of small cell carcinomas of the lung as well as of other small cell malignancies (such as Merkel cell carcinoma and neuroblastoma). The cells are small, approximately 2-3 times the diameter of small lymphocytes. The nuclei are dark, with finely granular chromatin texture. The cells of small cell carcinoma are distinguished from those of lymphoma by their tendency to form clusters.
Immunostains for CK Cam 5.2, CD56, Synaptophysin, PGP9.35 and TTF1 may be helpful.
CD45 and mesothelial markers should be also included in the panel. Please note that positivity for TTF1 in small cell carcinoma is not synonymous of lung origin.
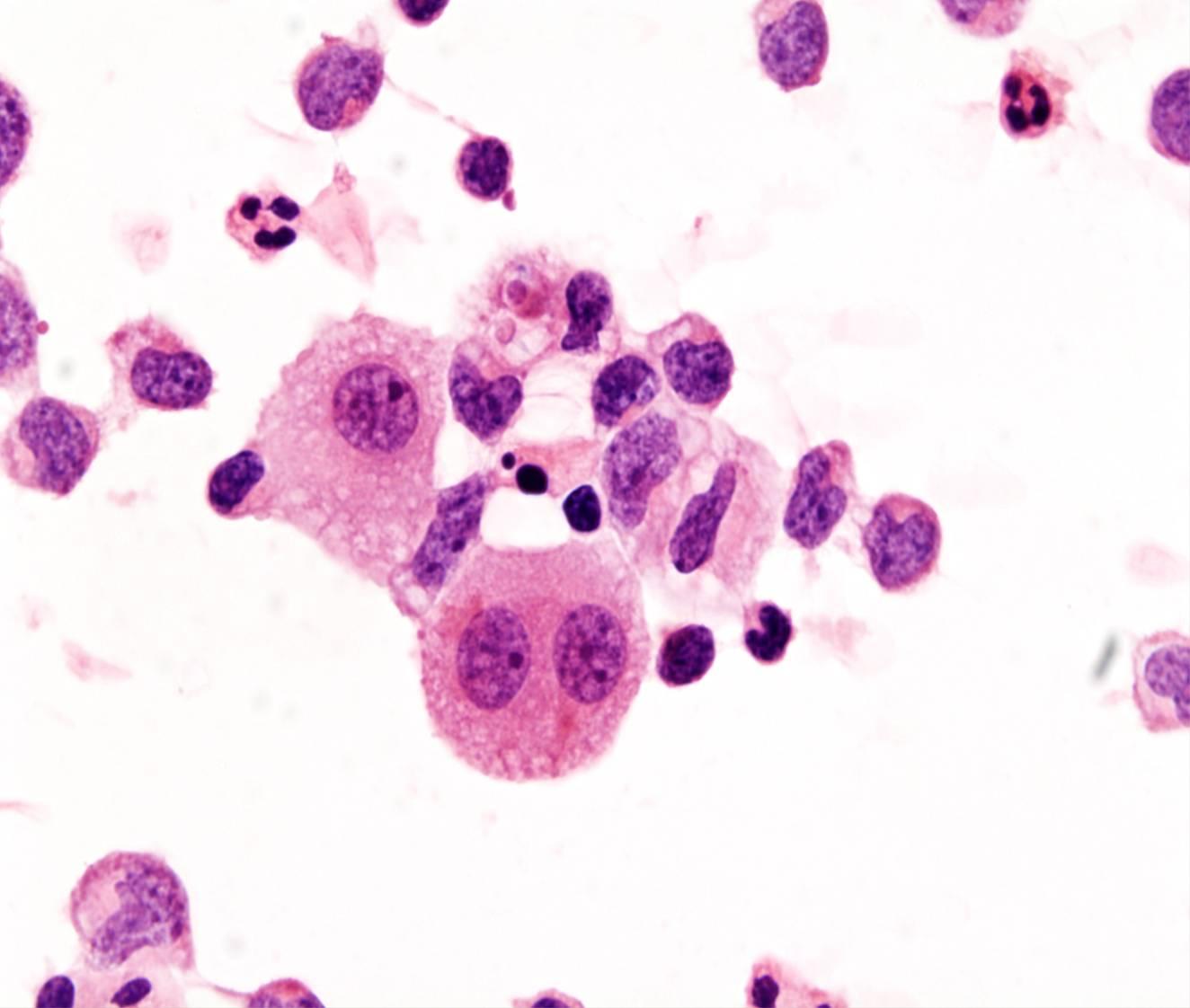
Squamous cell carcinoma
- Large clusters or isolated cells
- Dense cytoplasm
- Non-keratinising (mostly) or keratinising
Squamous cell carcinomas rarely metastasize to the serosal membranes, most commonly from lung, larynx or female genital tract (cervix). The cytologic appearance depends on the degree of differentiation. Nuclei are enlarged and hyperchromatic, nucleoli are usually not prominent. Anucleate squames can be present. Cytoplasmic vacuoles may be present in up to 30% of cases (differential diagnosis with adenocarcinoma)
Immunostain for CK5 and p40 may be helpful to confirm the squamous origin of tumour cells.
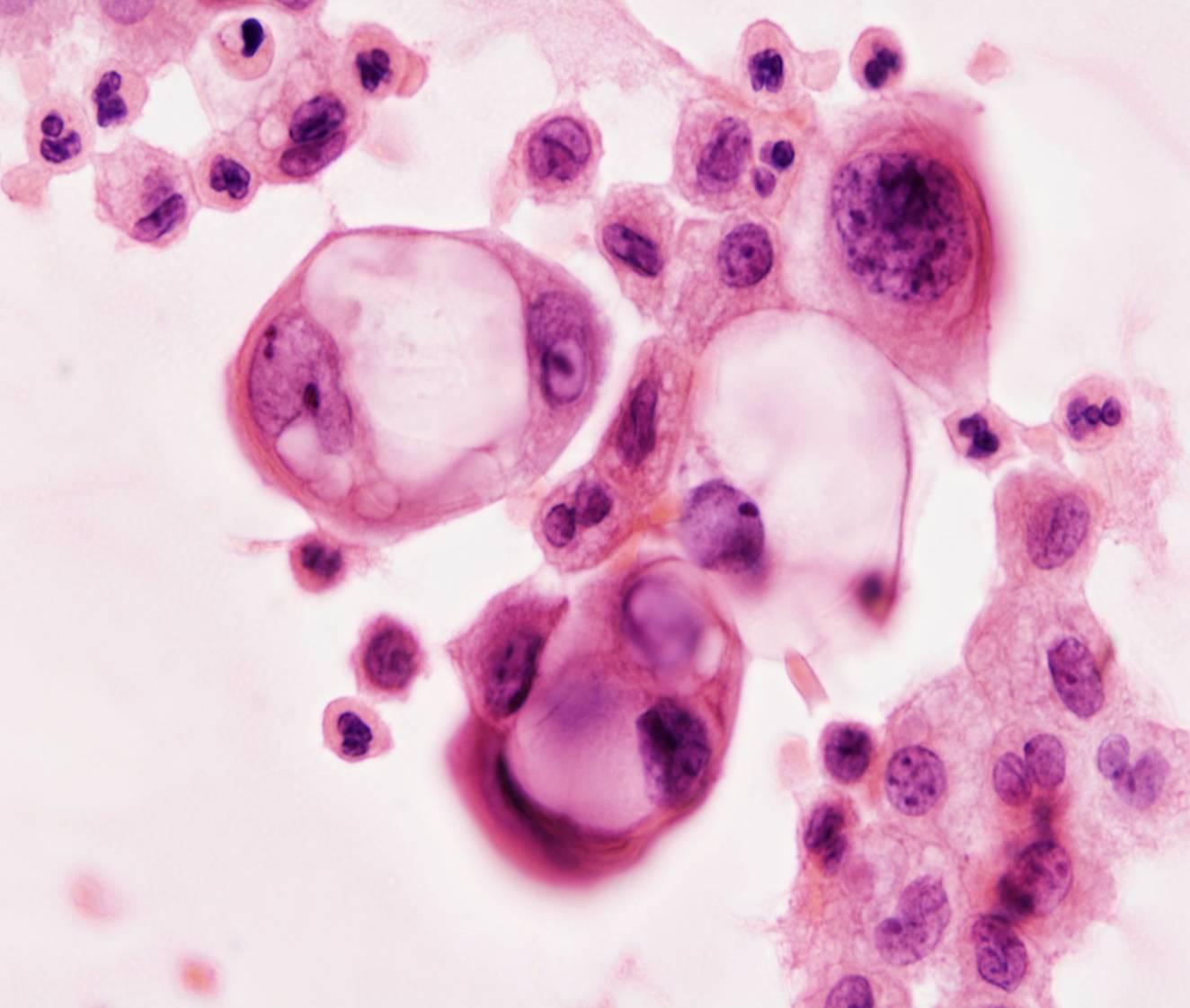
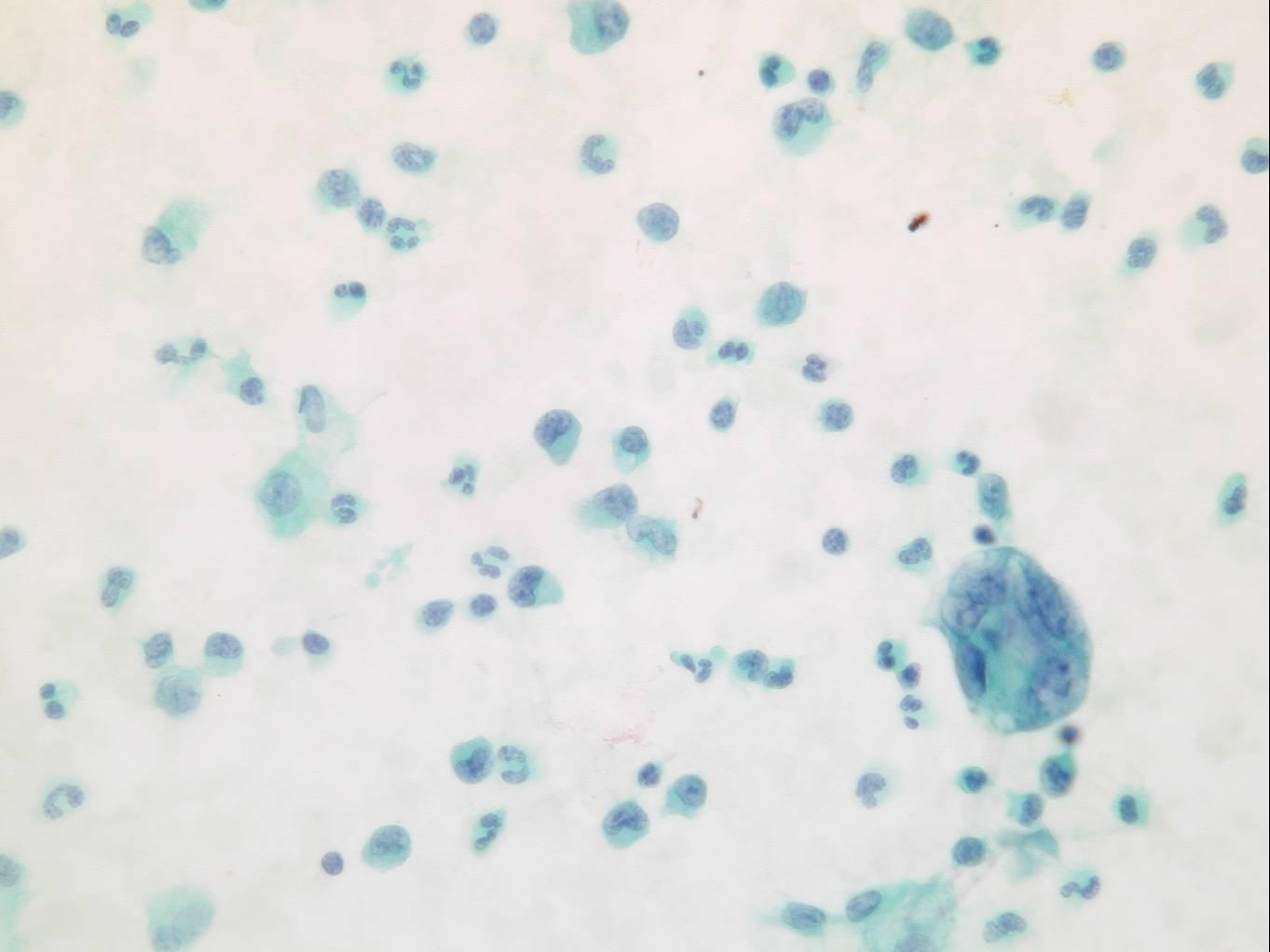
Malignant melanoma
- Dispersed tumour cells
- Brown melanin pigment
- Binucleated (mirror image)
In effusions the malignant cells of metastatic melanoma resemble mesothelial cells: they are often dispersed as isolated round cells with prominent nucleoli. In some cases, they show a fine brown cytoplasmic pigmentation and intranuclear inclusions. Cell clusters are uncommon.
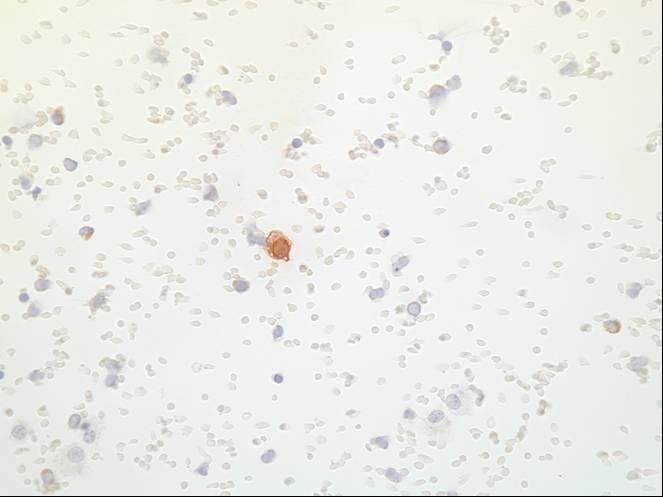
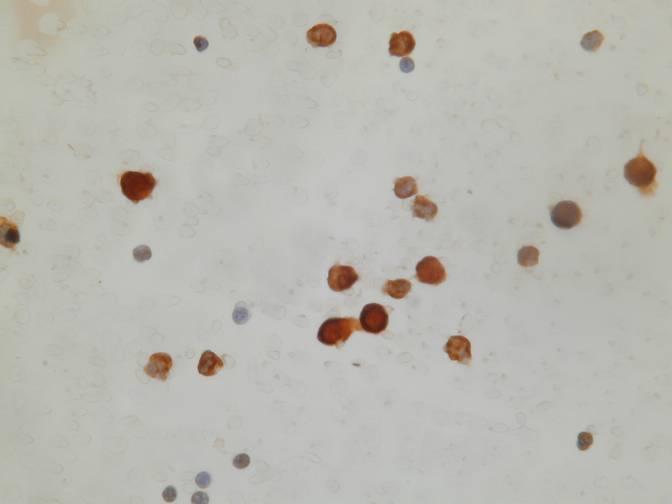
Immunocytochemistry is helpful when the distinction from reactive mesothelial cells is difficult: melanomas are positive for S-100 protein, Melan A and HMB-45 and negative for keratin markers.
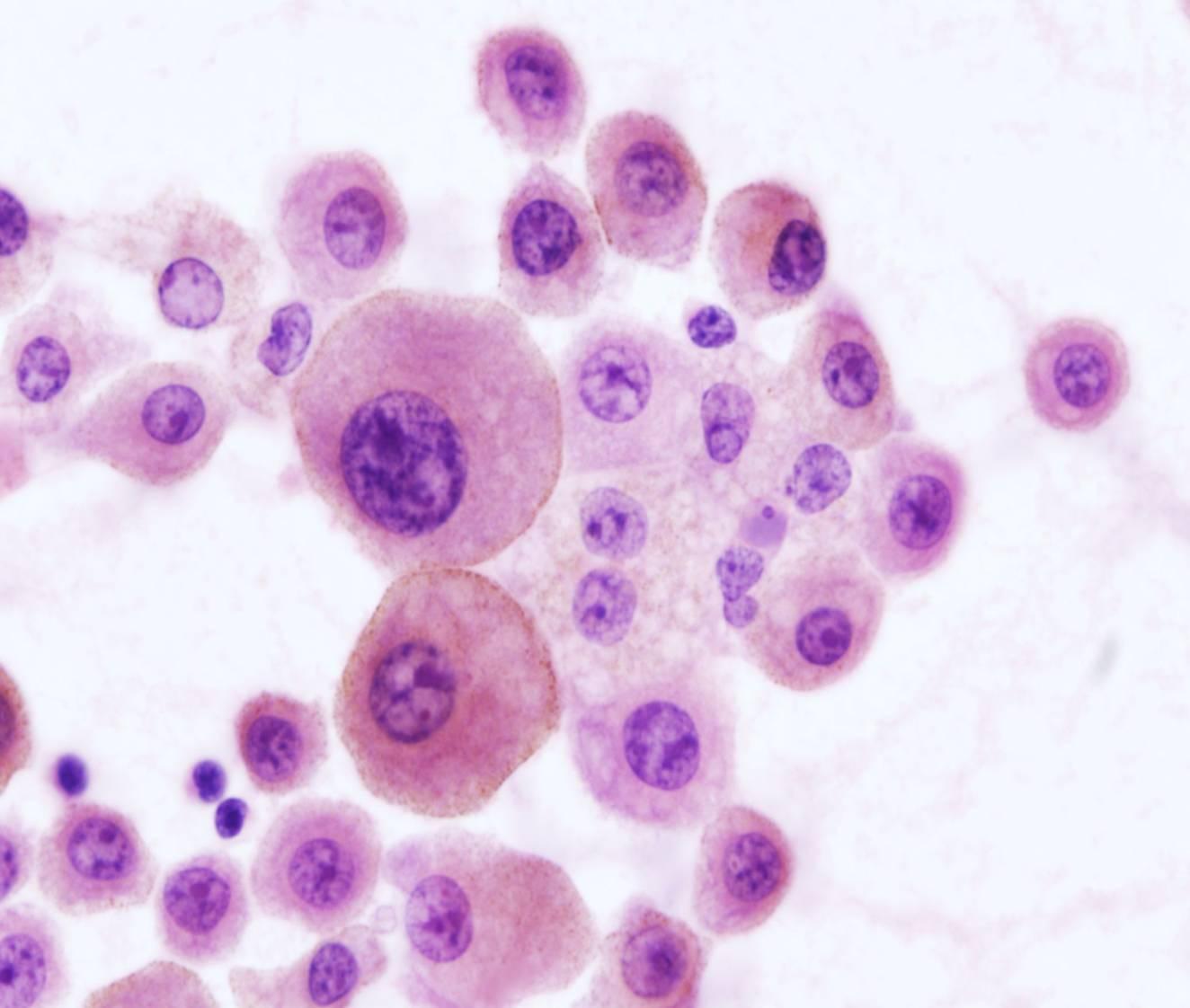
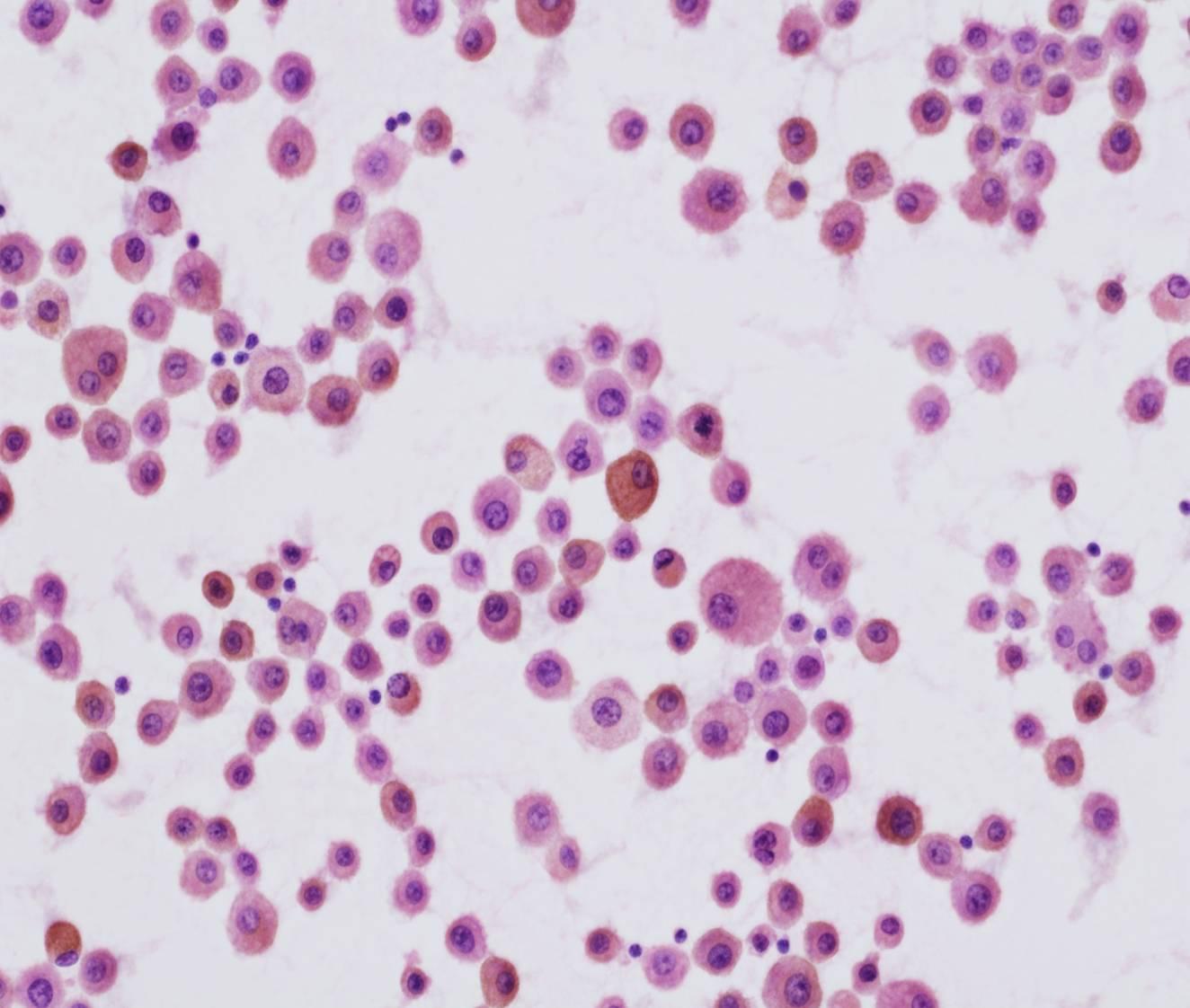
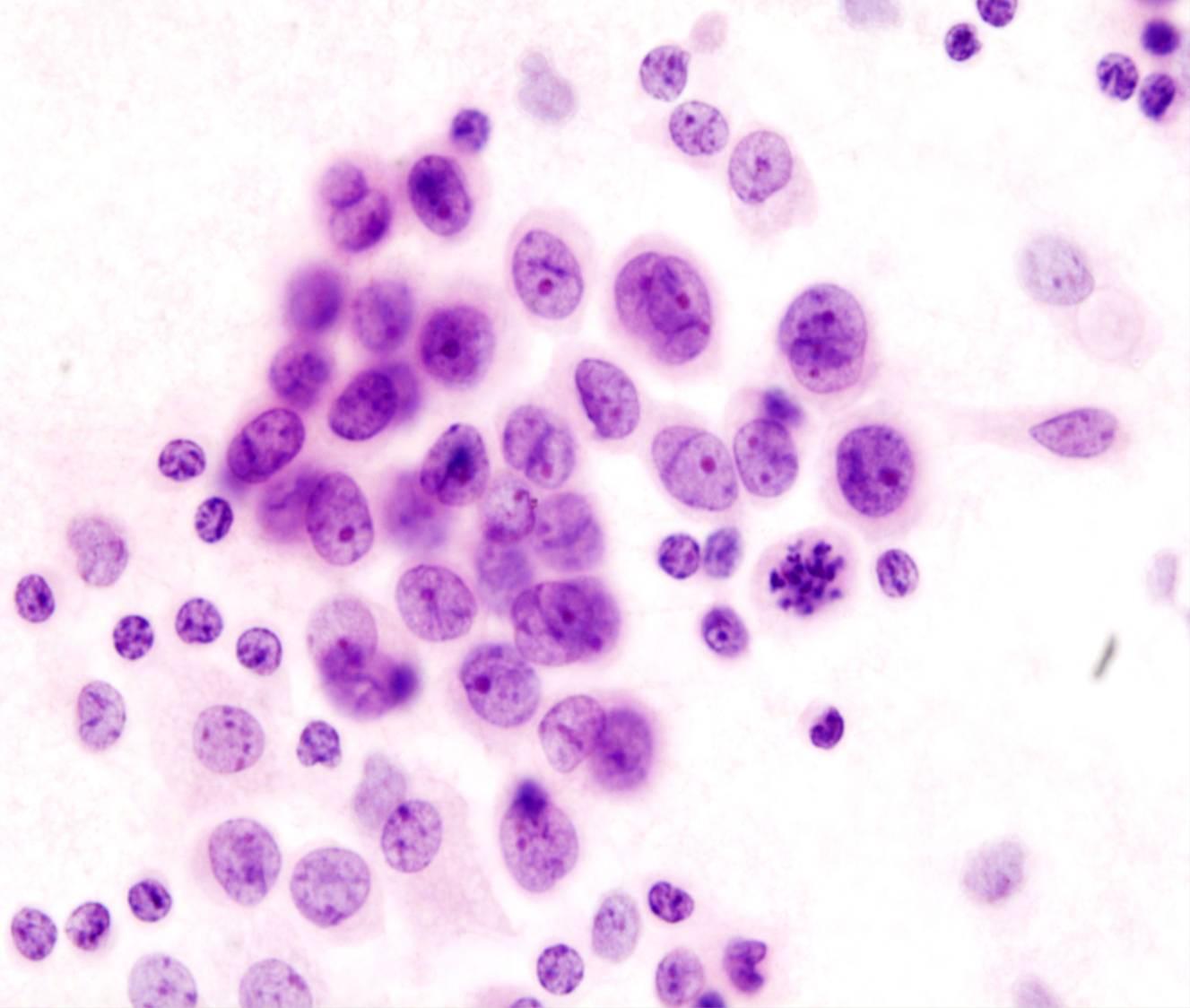
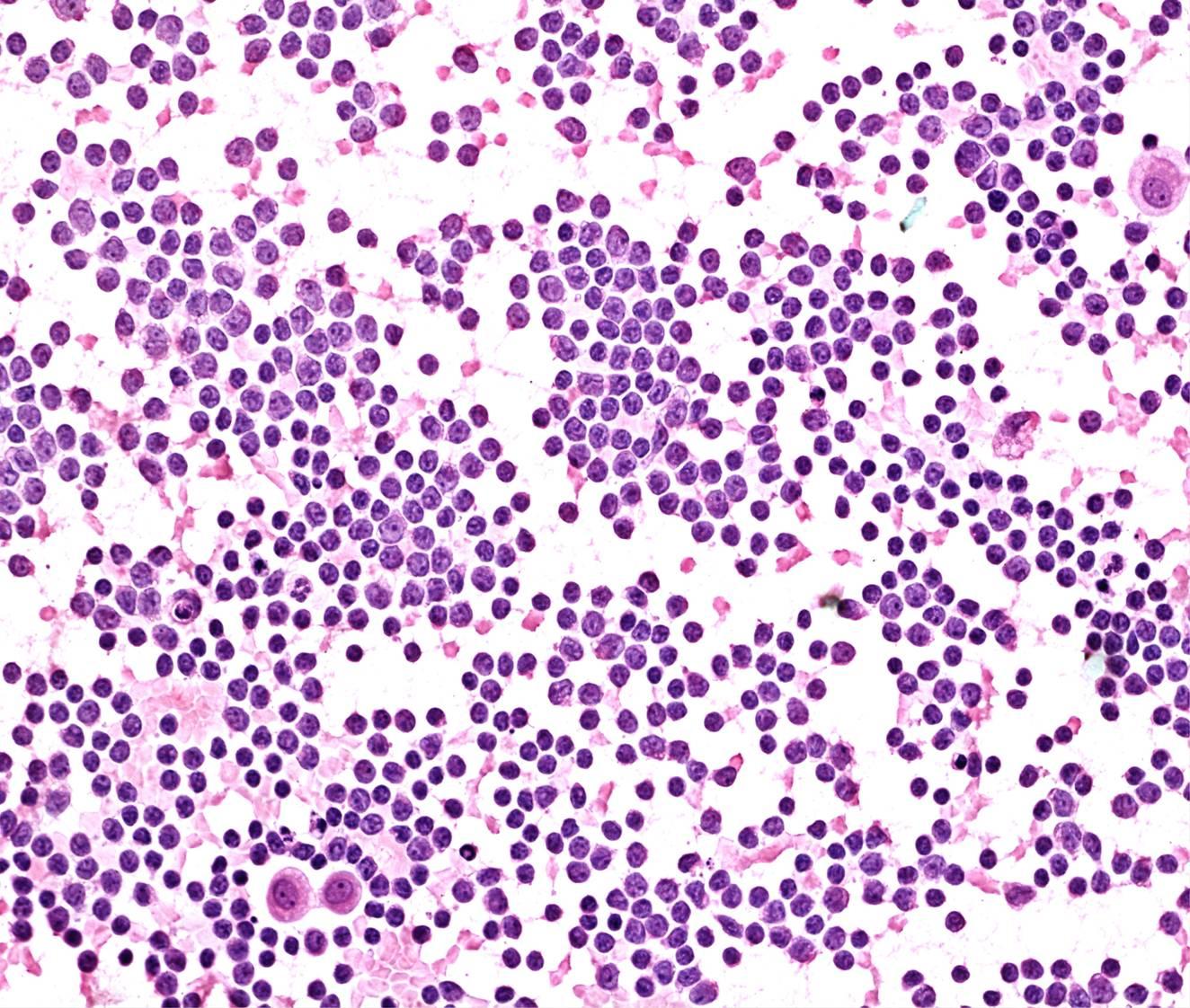
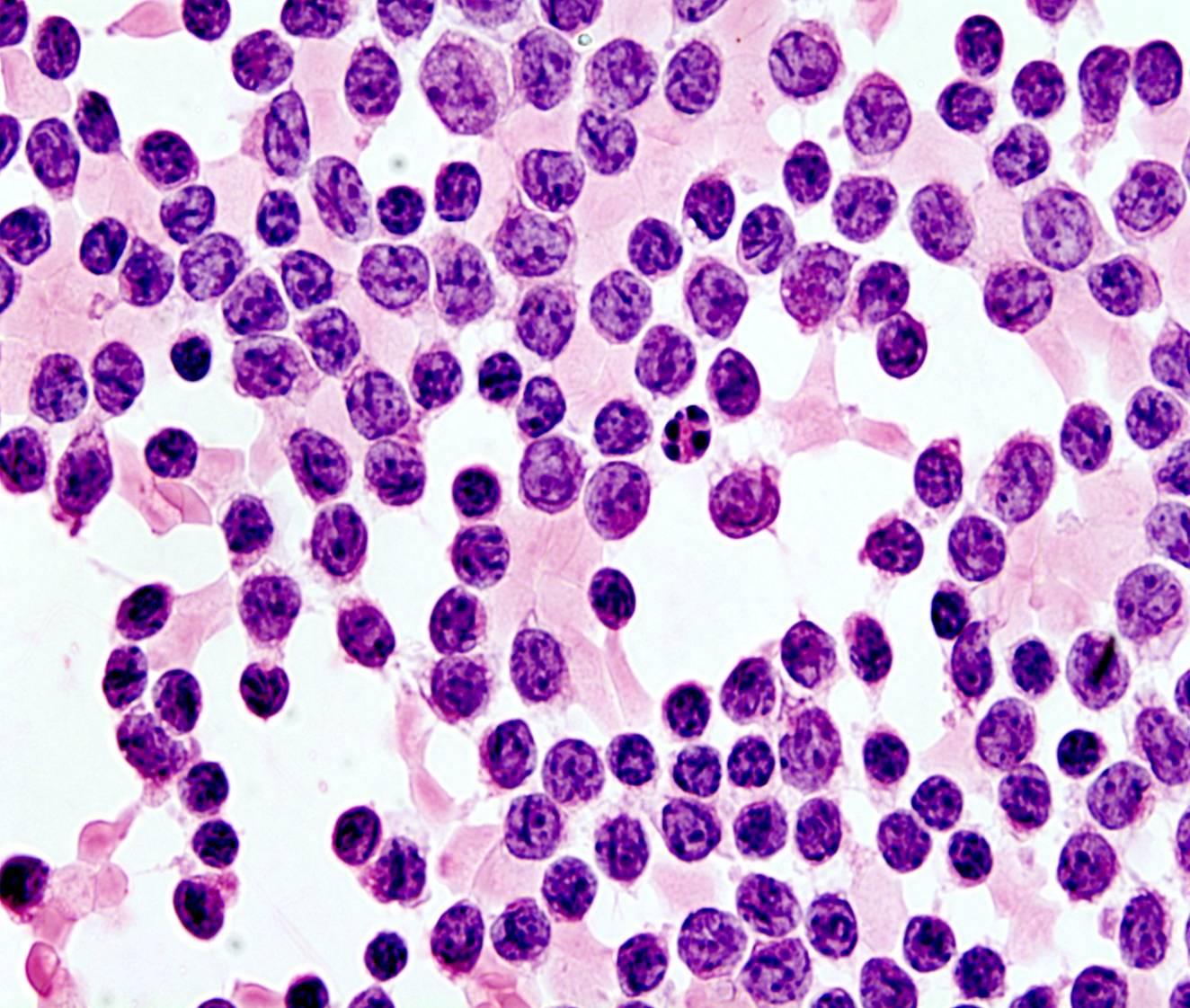
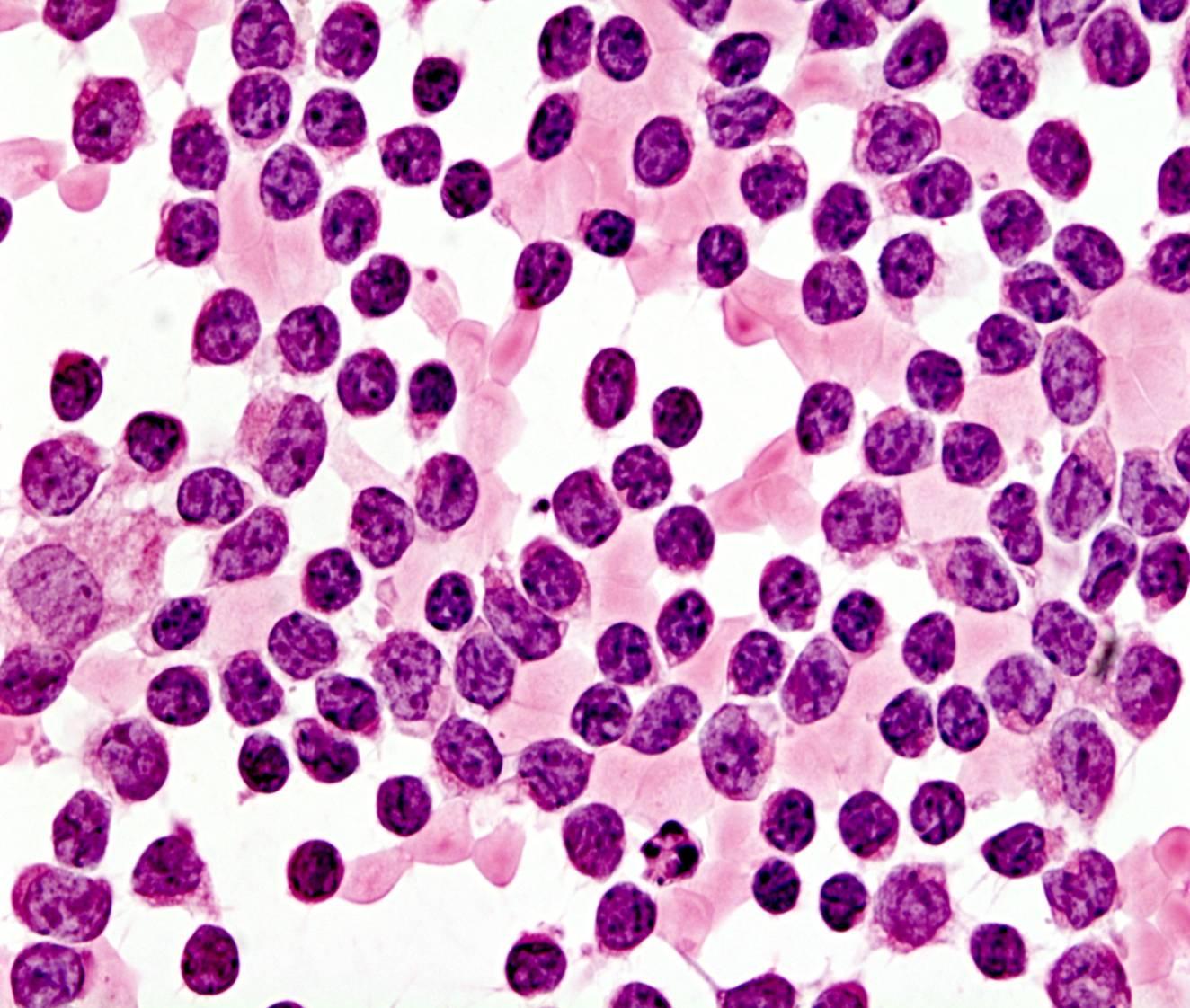
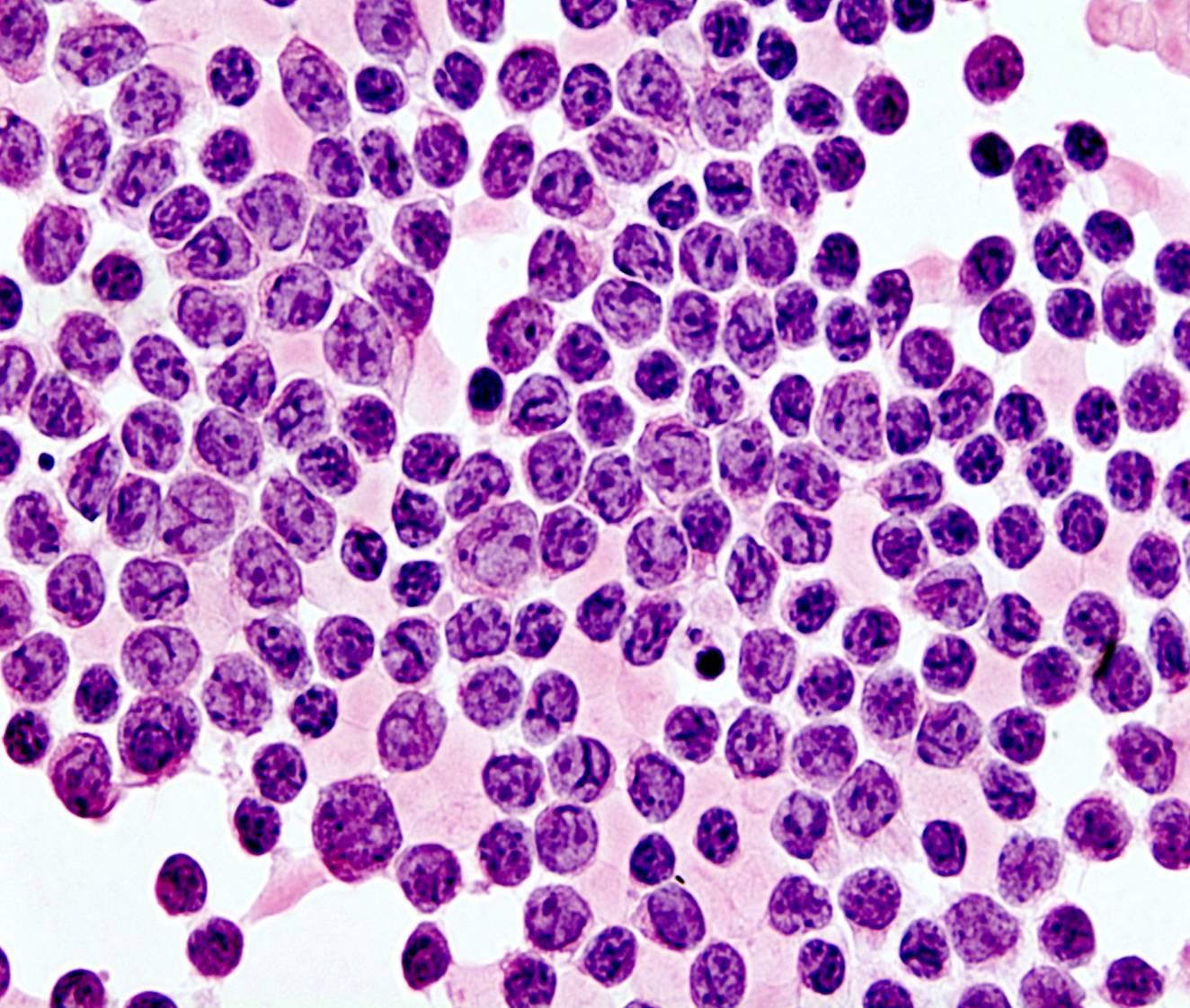
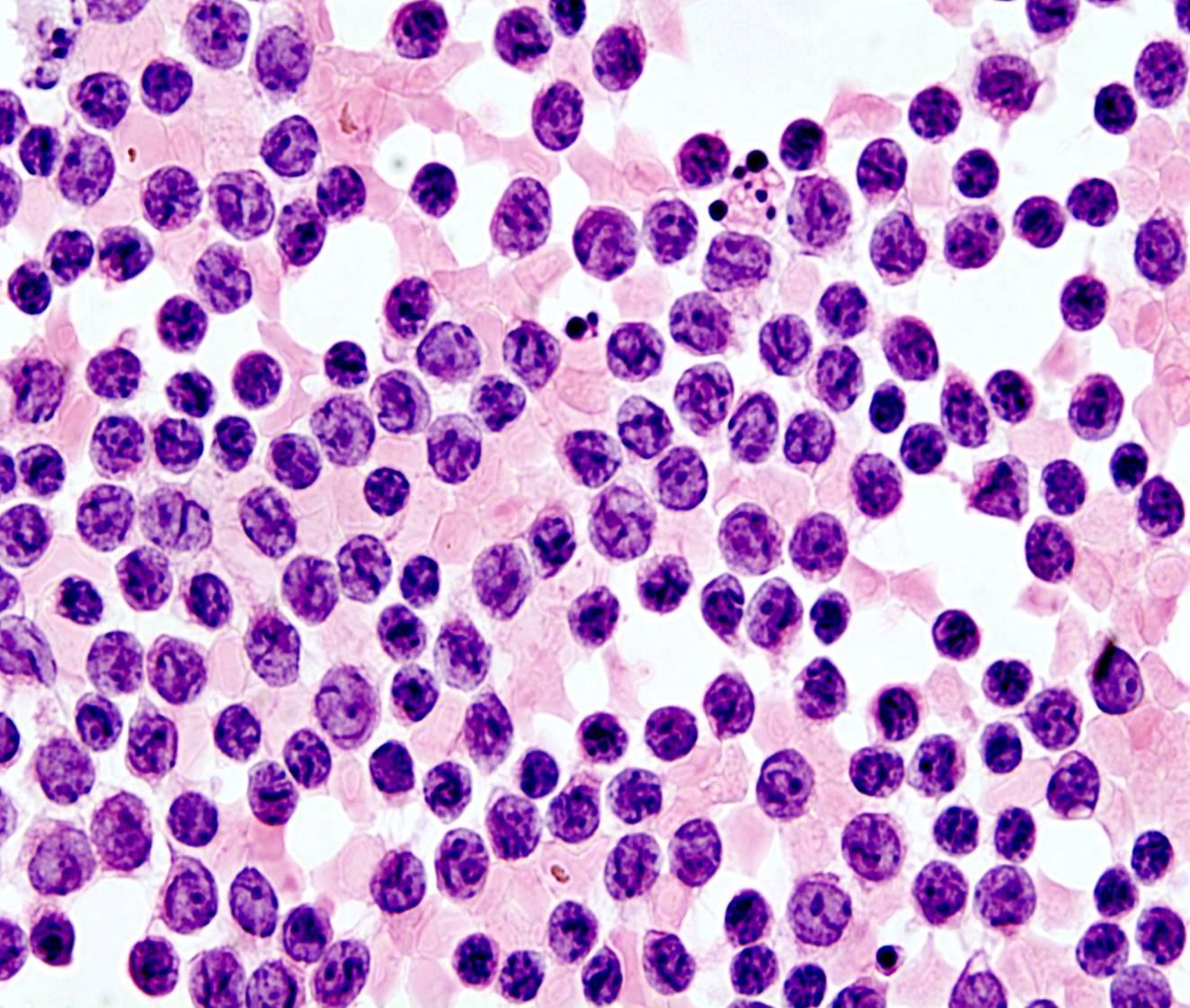
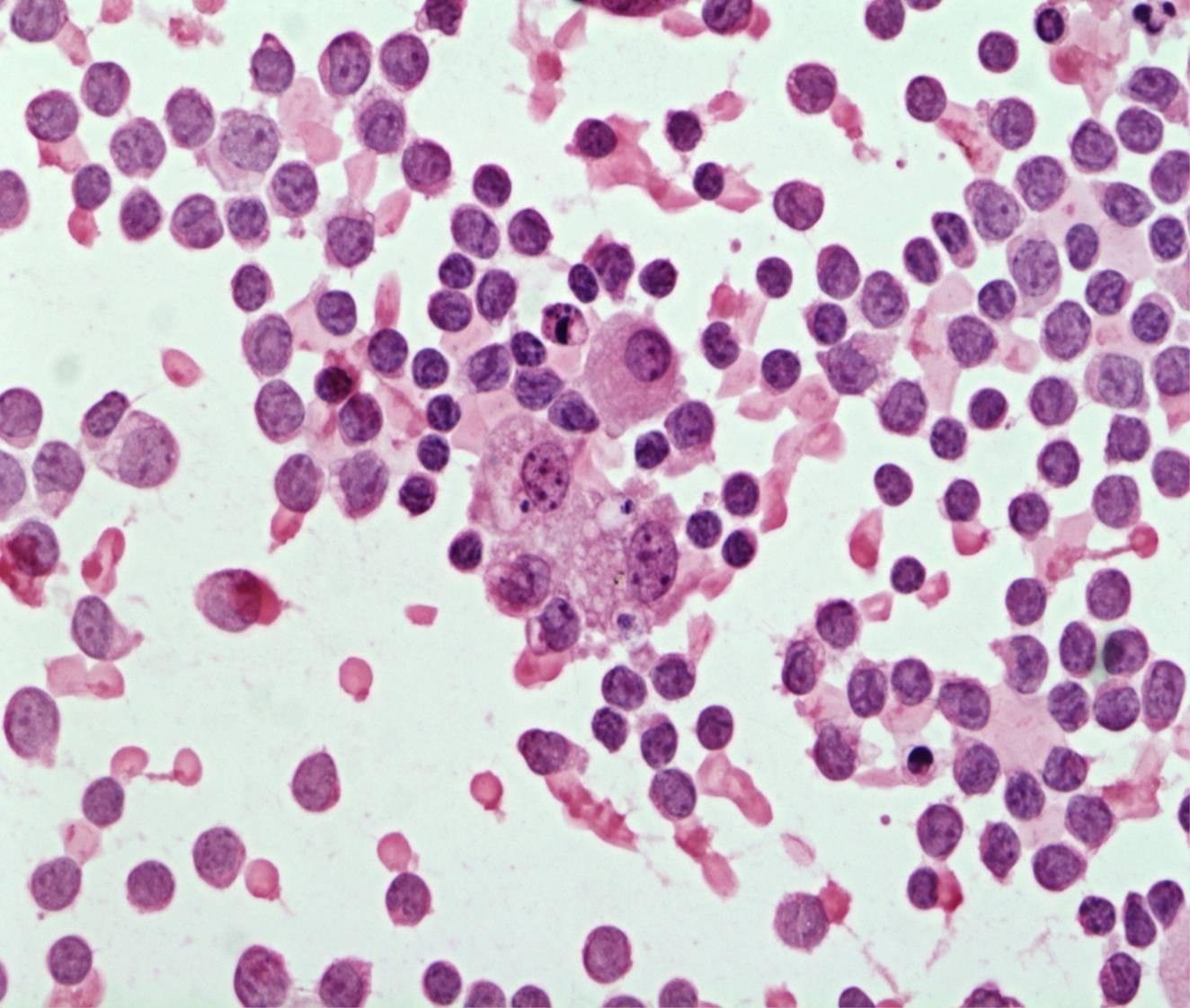
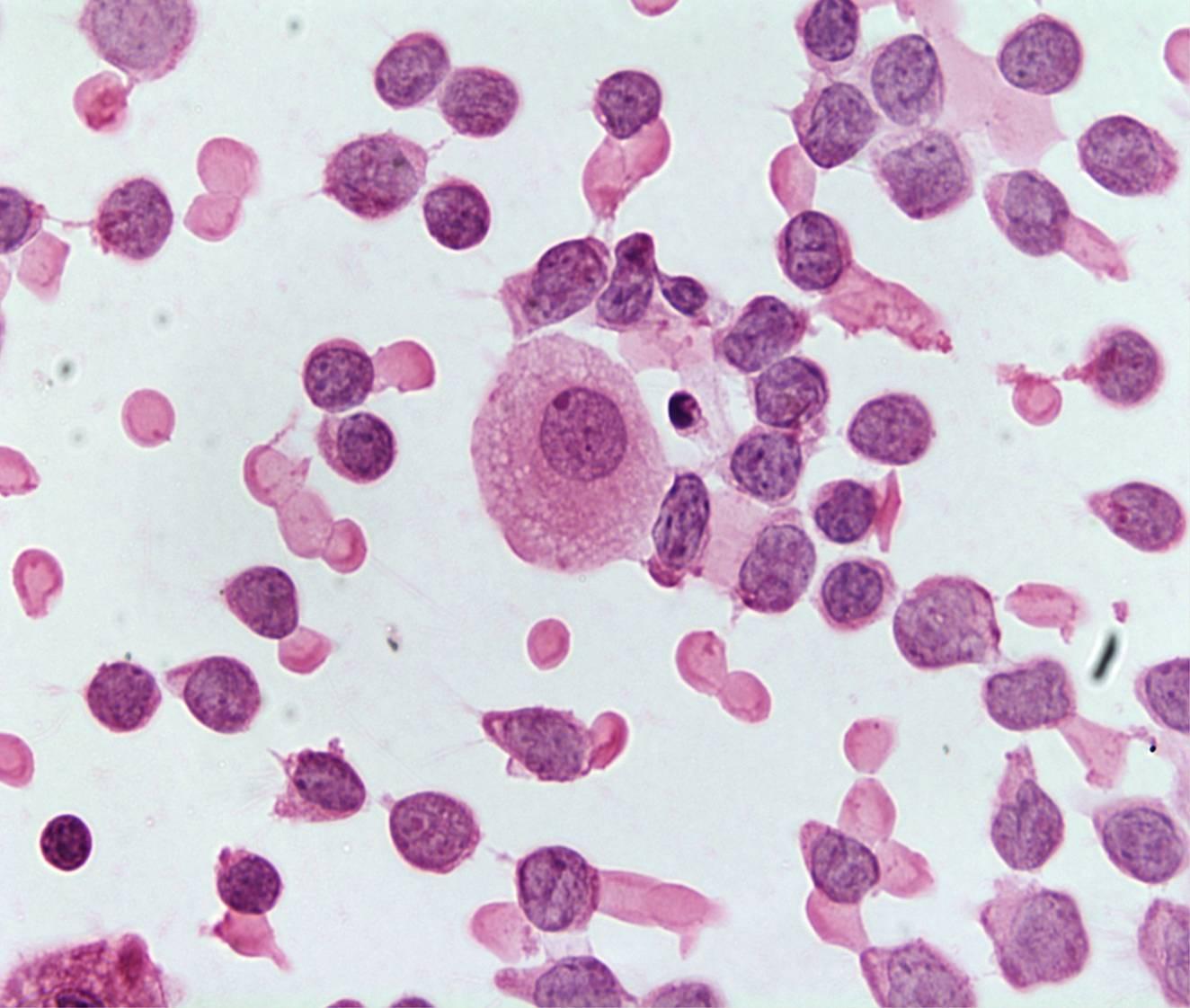
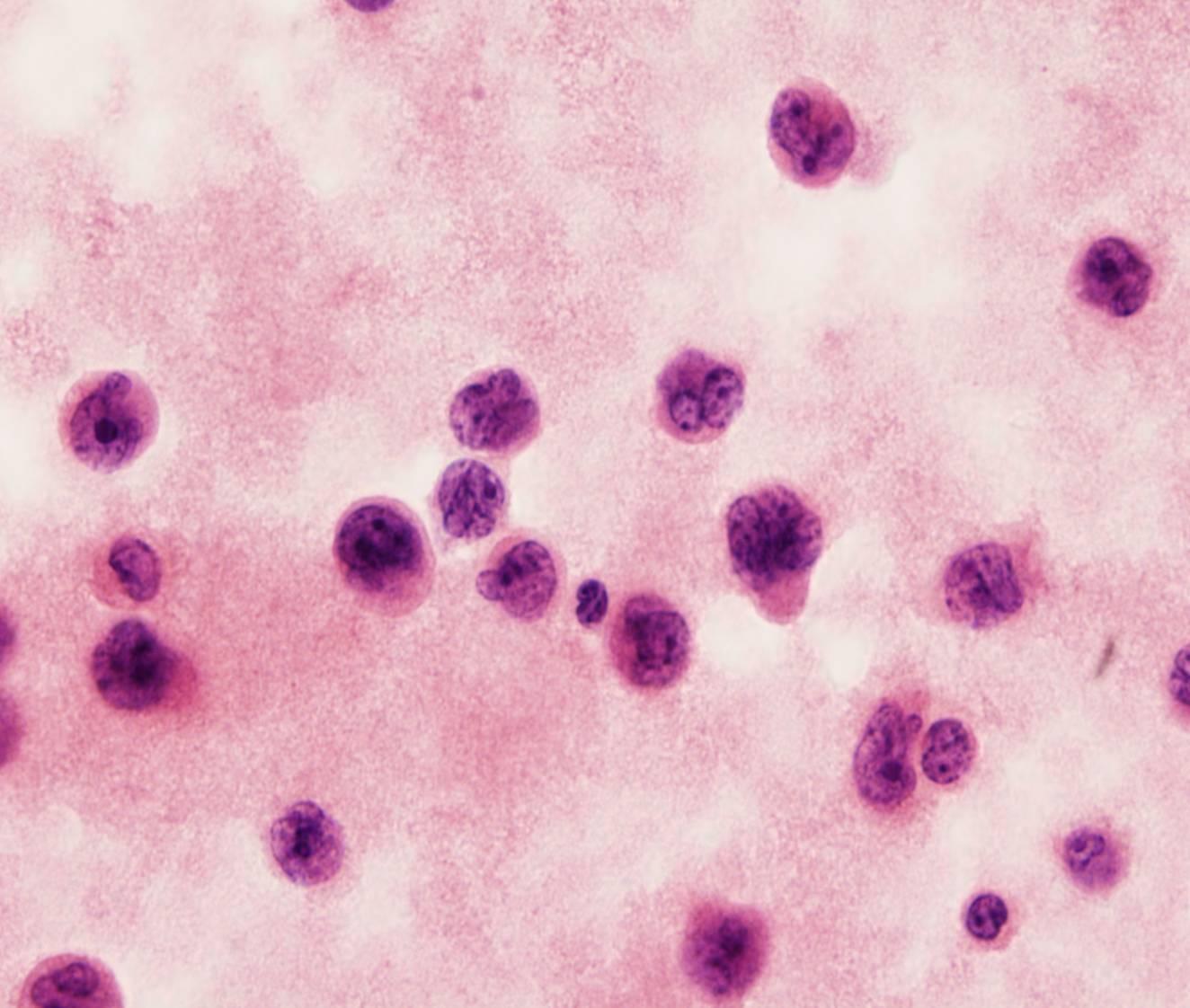
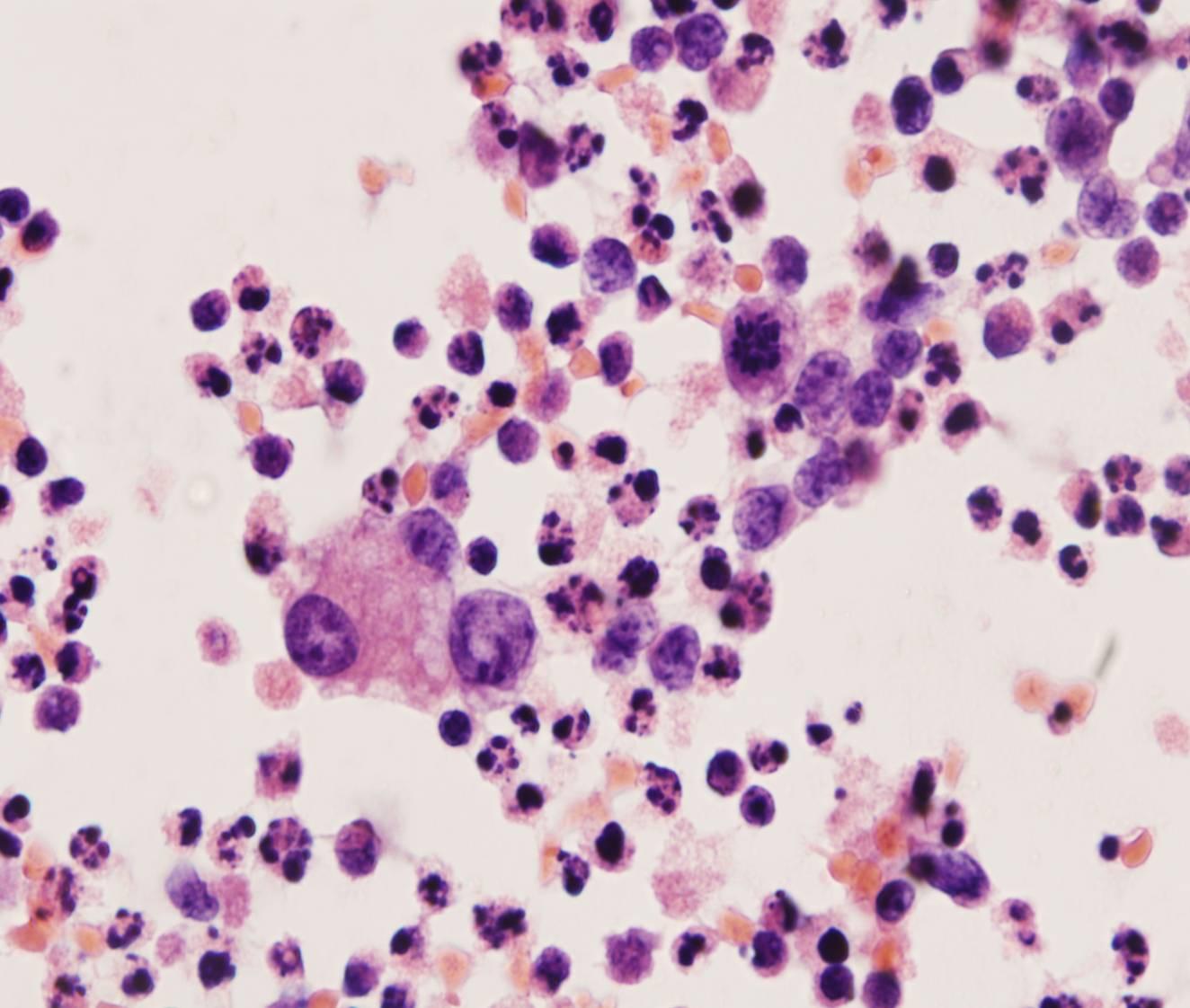
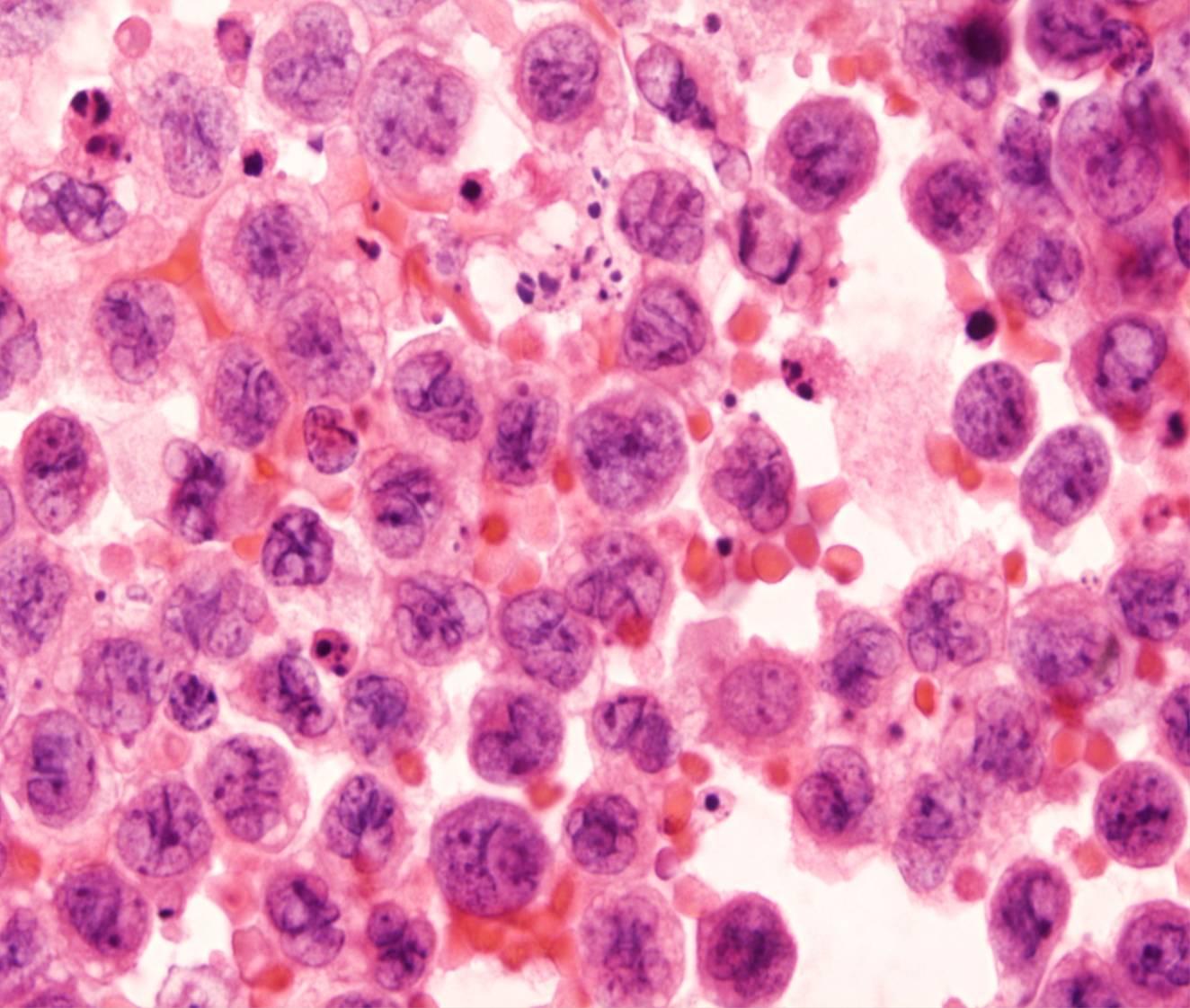
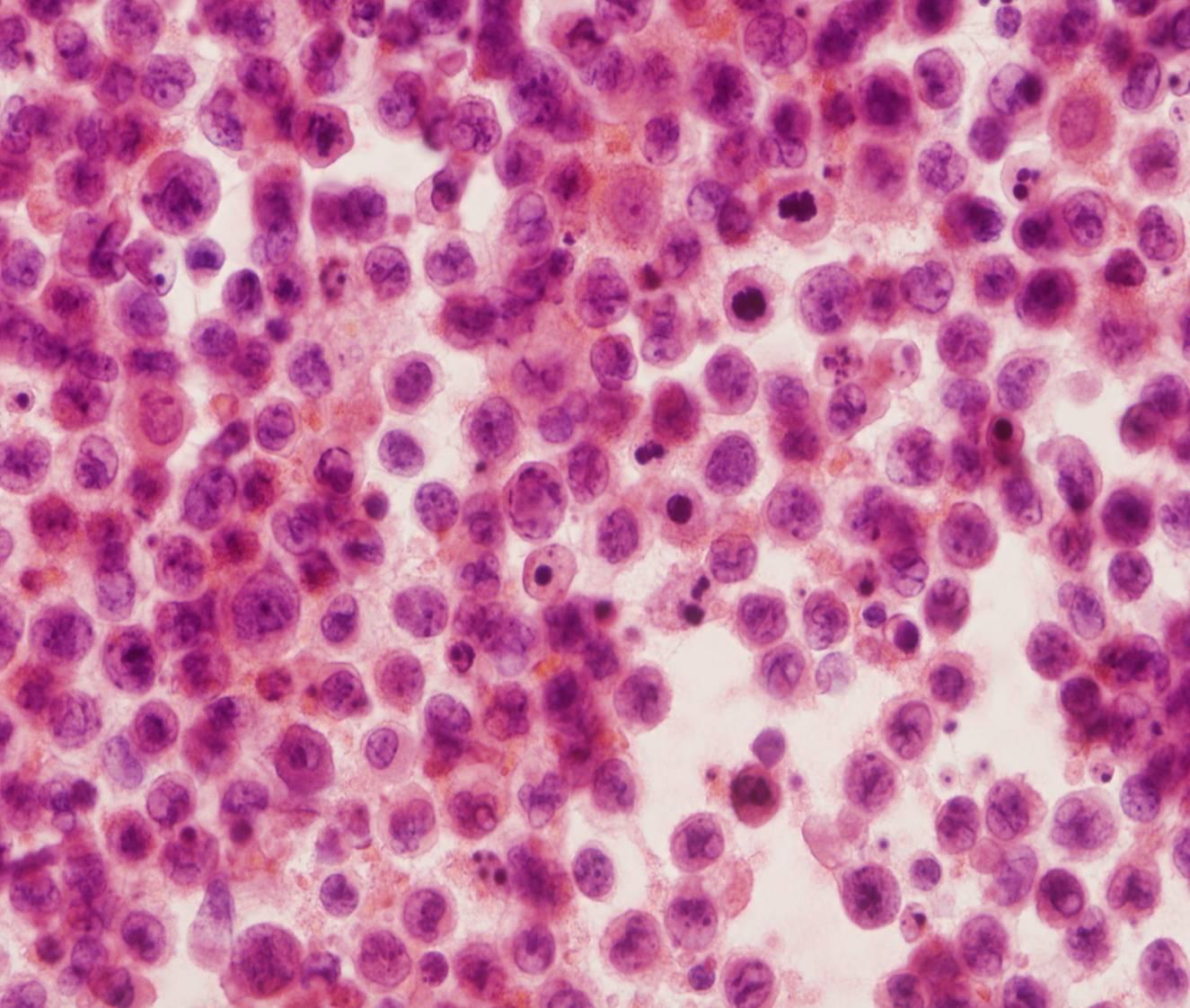
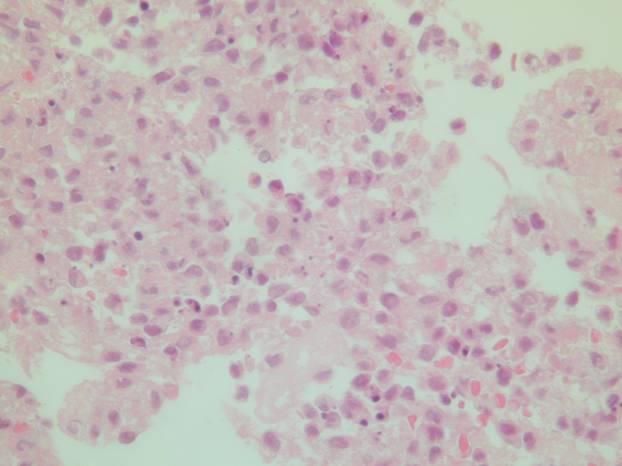
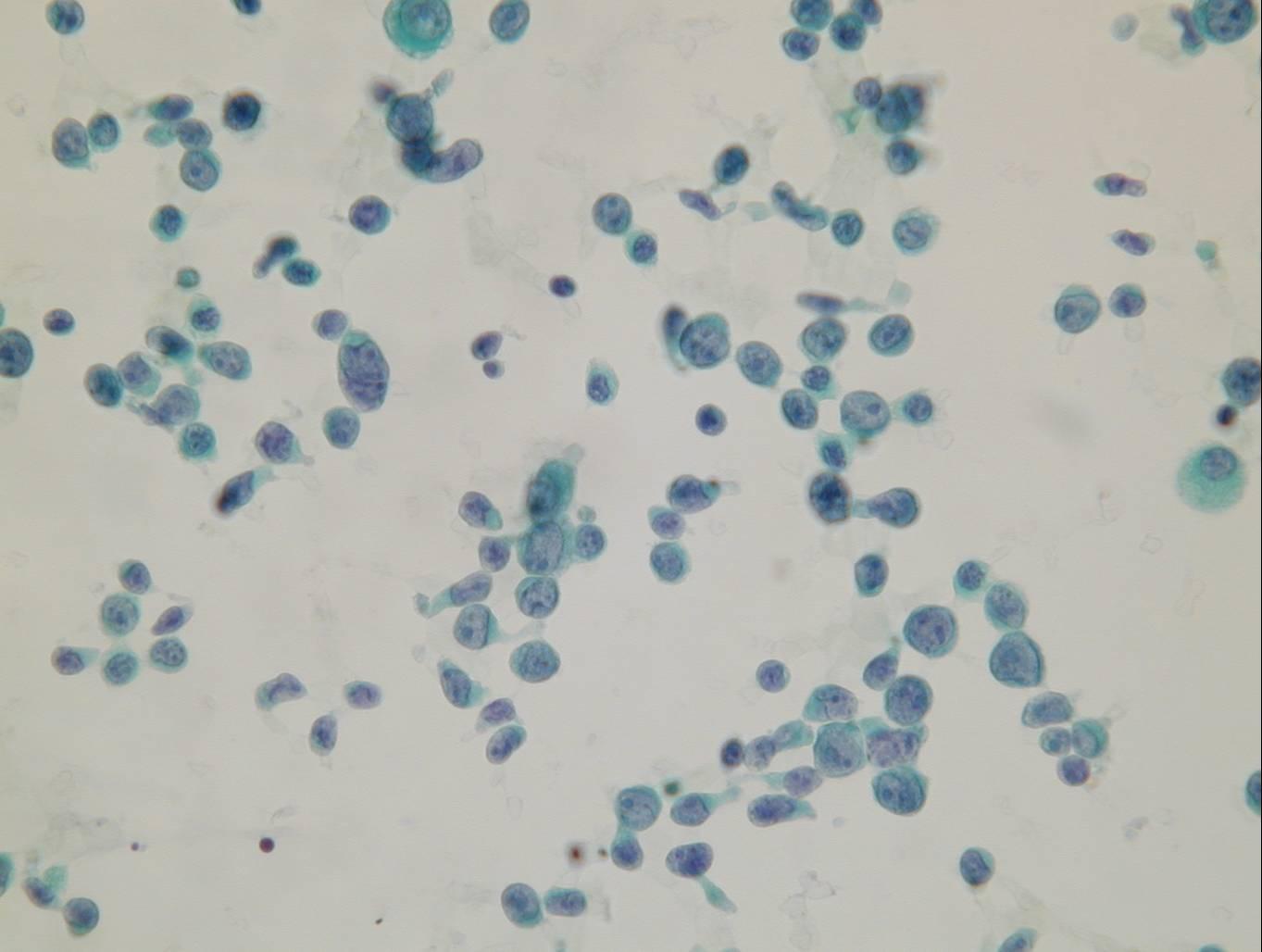
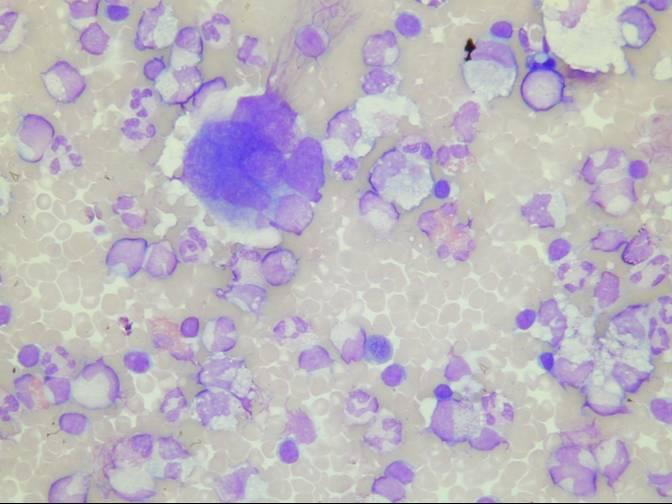
Non-Hodgkin lymphoma
- Monotonous picture
- Dispersed tumour cells
- Few mesothelial cells and macrophages
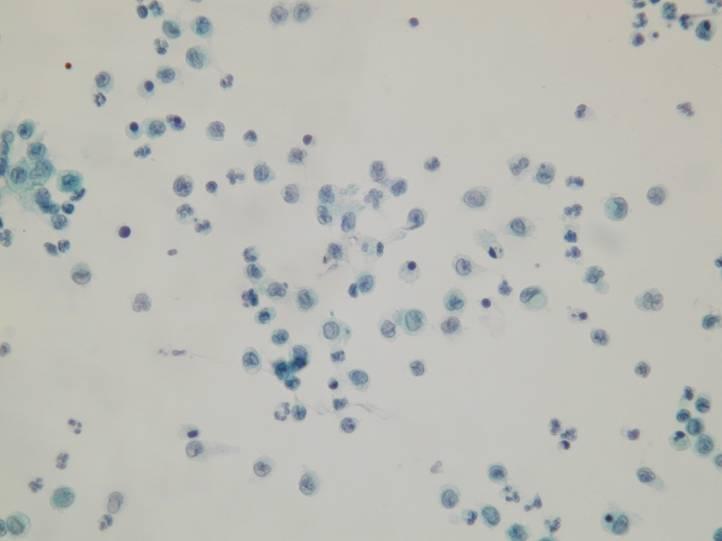
A malignant effusion may appear in the course of disease in many patients with non-Hodgkin lymphoma. Cytologic preparations are highly cellular and composed of dispersed lymphoid cells. Mesothelial cells may be absent.
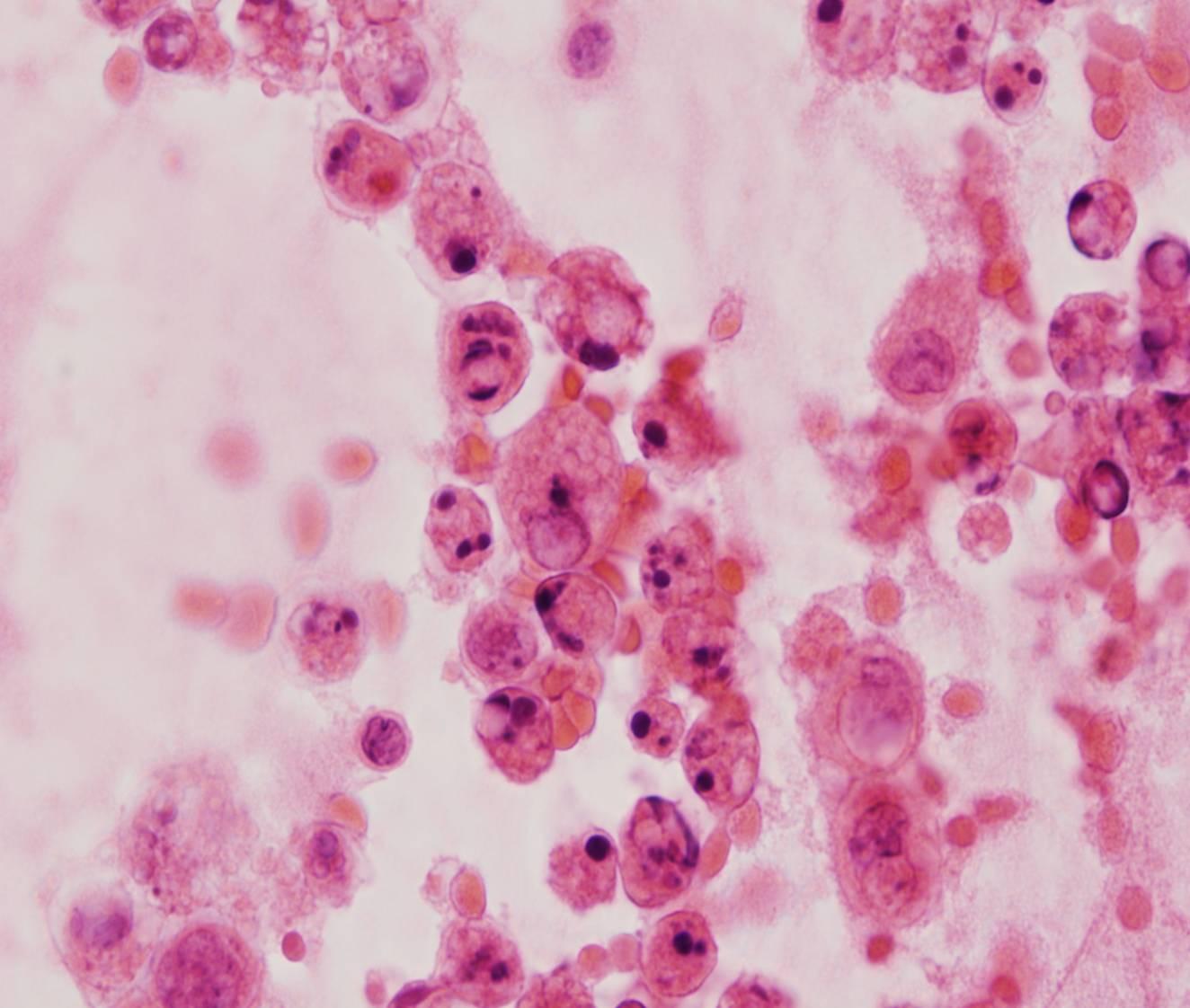
Several histologic types of non-Hodgkin lymphoma may involve the serosal cavities. The cells of large B-cell lymphomas have abundant, pale and vacuolated cytoplasm, and round or irregular nuclei with coarse chromatin. The cells of small cell lymphomas are only slightly larger than lymphocytes. Also follicular lymphomas, lymphoblastic lymphoma and Burkitt lymphoma can involve the serosal cavities. Karyorrhexis is a conspicuous feature of many lymphomas.
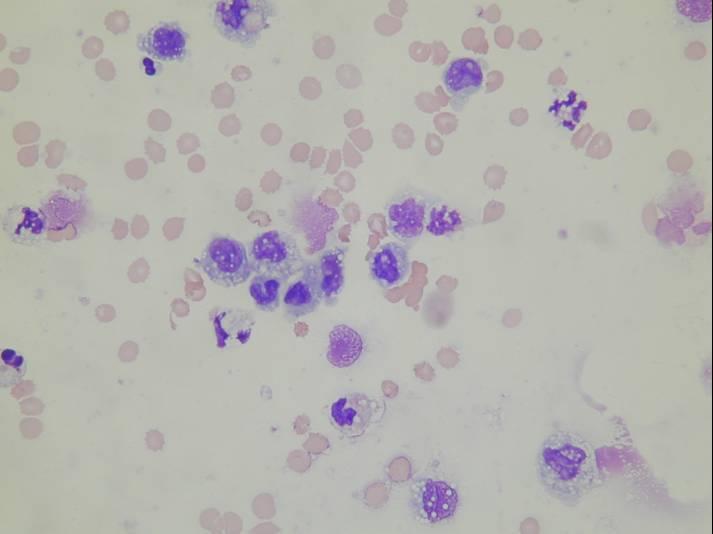
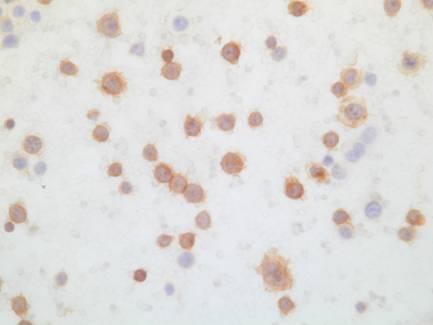
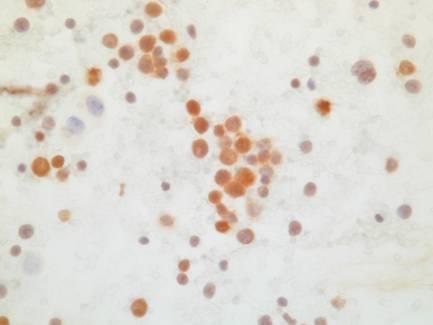
The differential diagnosis of small cell lymphomas includes benign effusions such as those due to tuberculosis, in which the fluid is composed predominantly of mature lymphocytes. The cells of small cell lymphomas may be impossible to distinguish from mature lymphocytes with Papanicolaou stains, whereas in Romanowsky-stained preparations they have a prominent coarse chromatin clumping. In lymphocyte-rich effusions which are cytologically equivocal for malignancy, kappa and lambda light chain expression can be examined by immunocytochemistry or flow cytometry, in order to document light chain restriction. Lymphomas are rarely confused with other malignancies because other tumours tend to form cell clusters in effusion. If there is any doubt about the lymphoid nature of malignant cells, an immunocytochemical panel of antibodies can be performed.
However, Flow Cytometry on a fresh sample appears to be the best method to confirm the morphological findings and subclassify the tumour
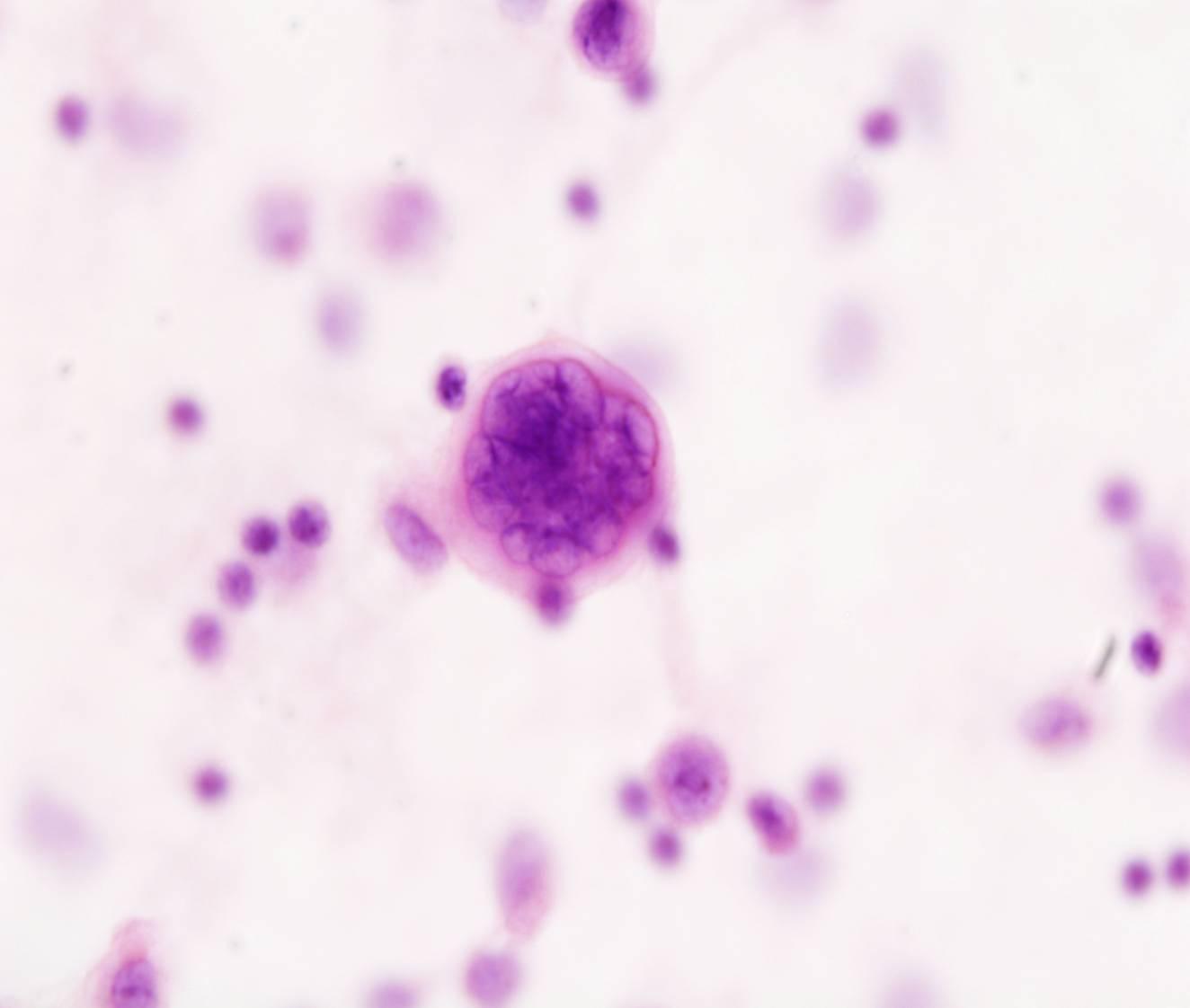
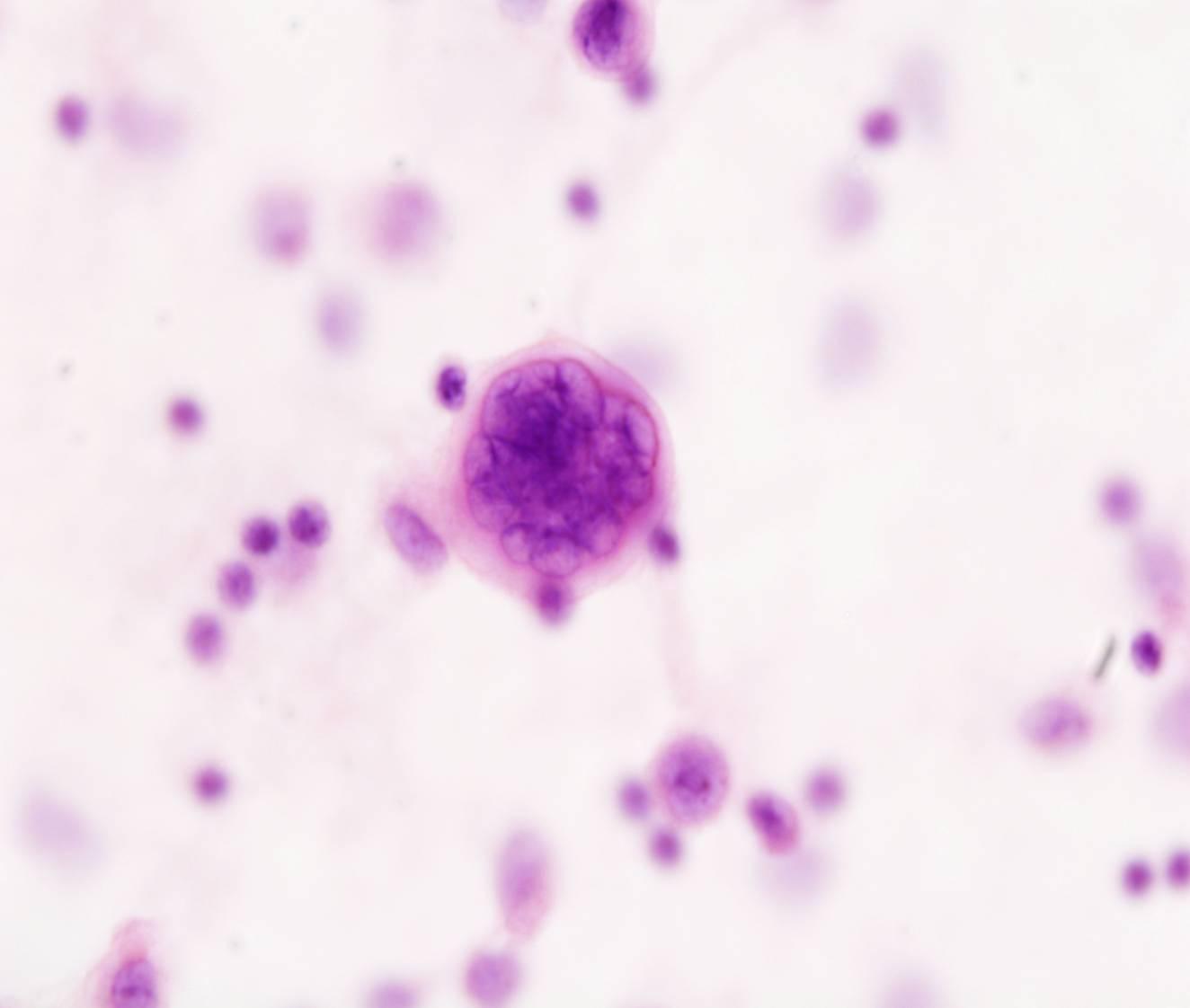
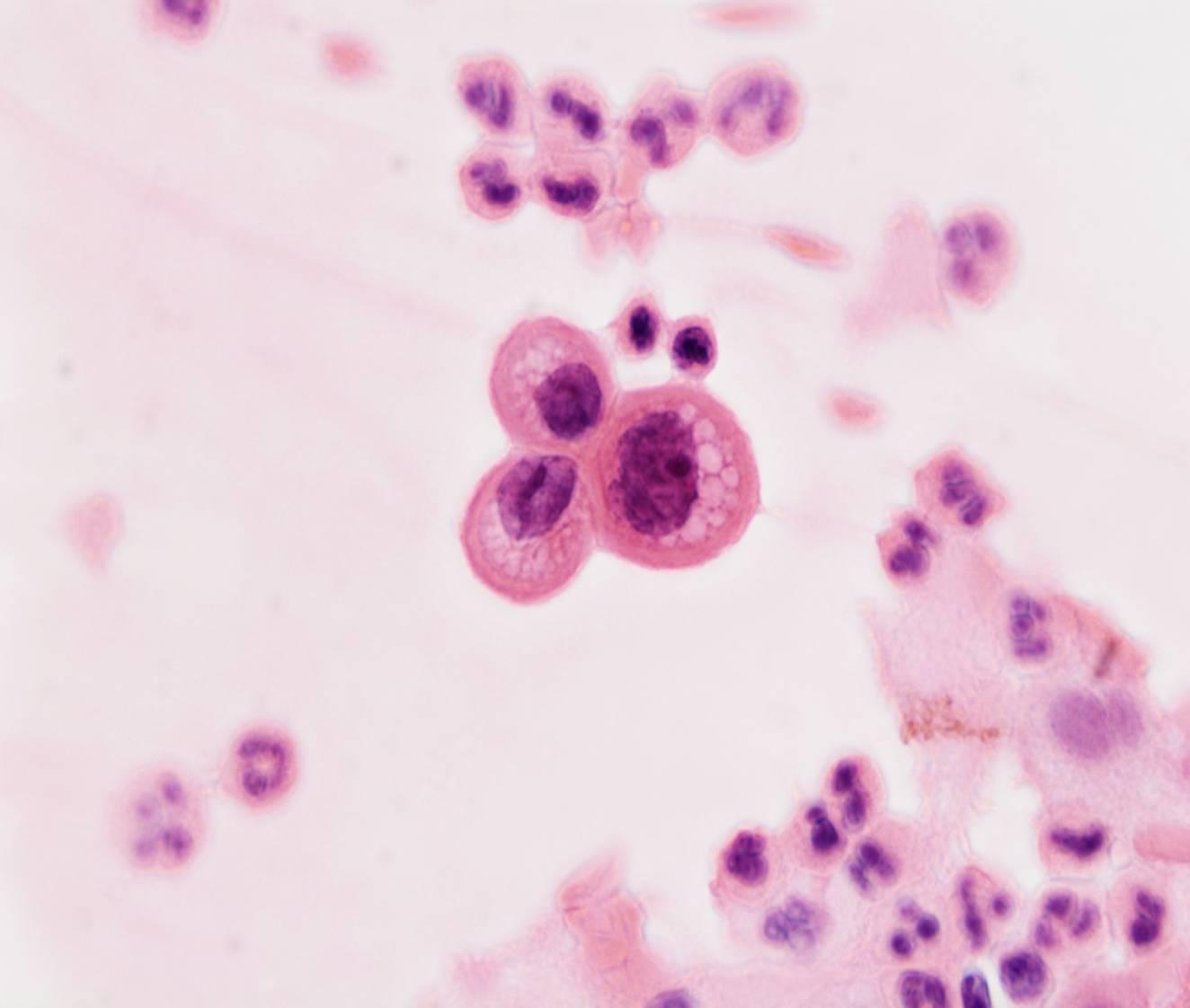
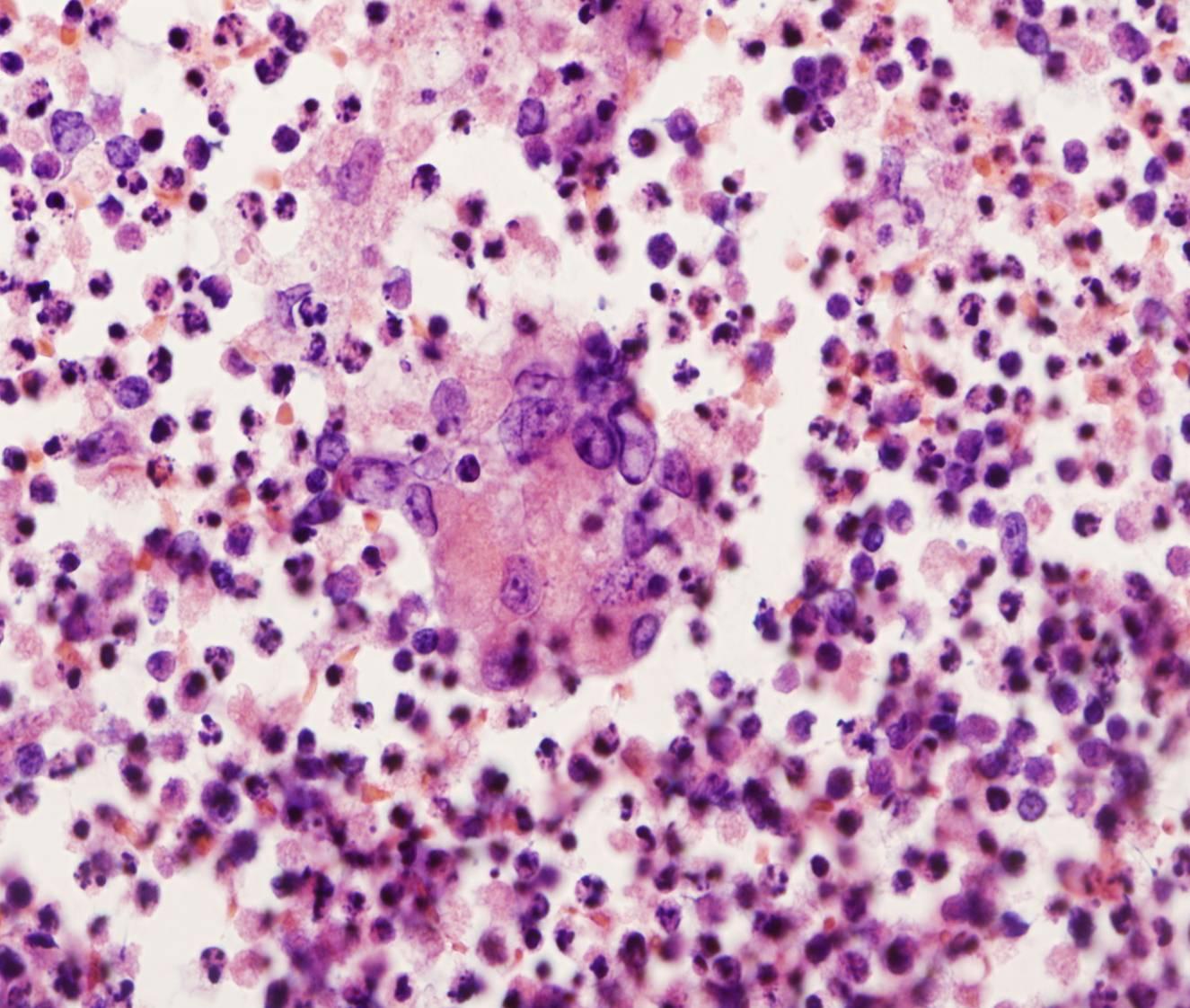
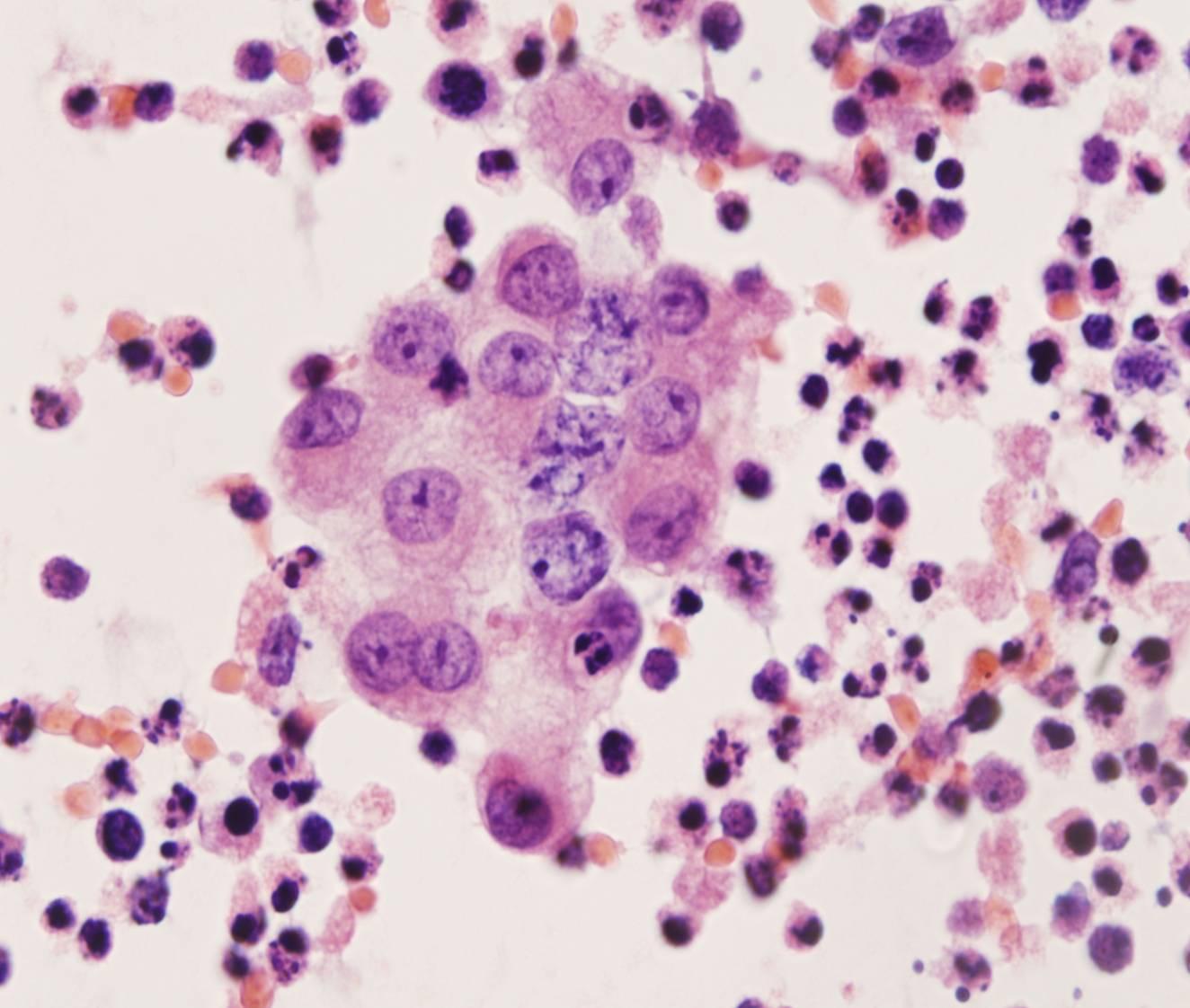
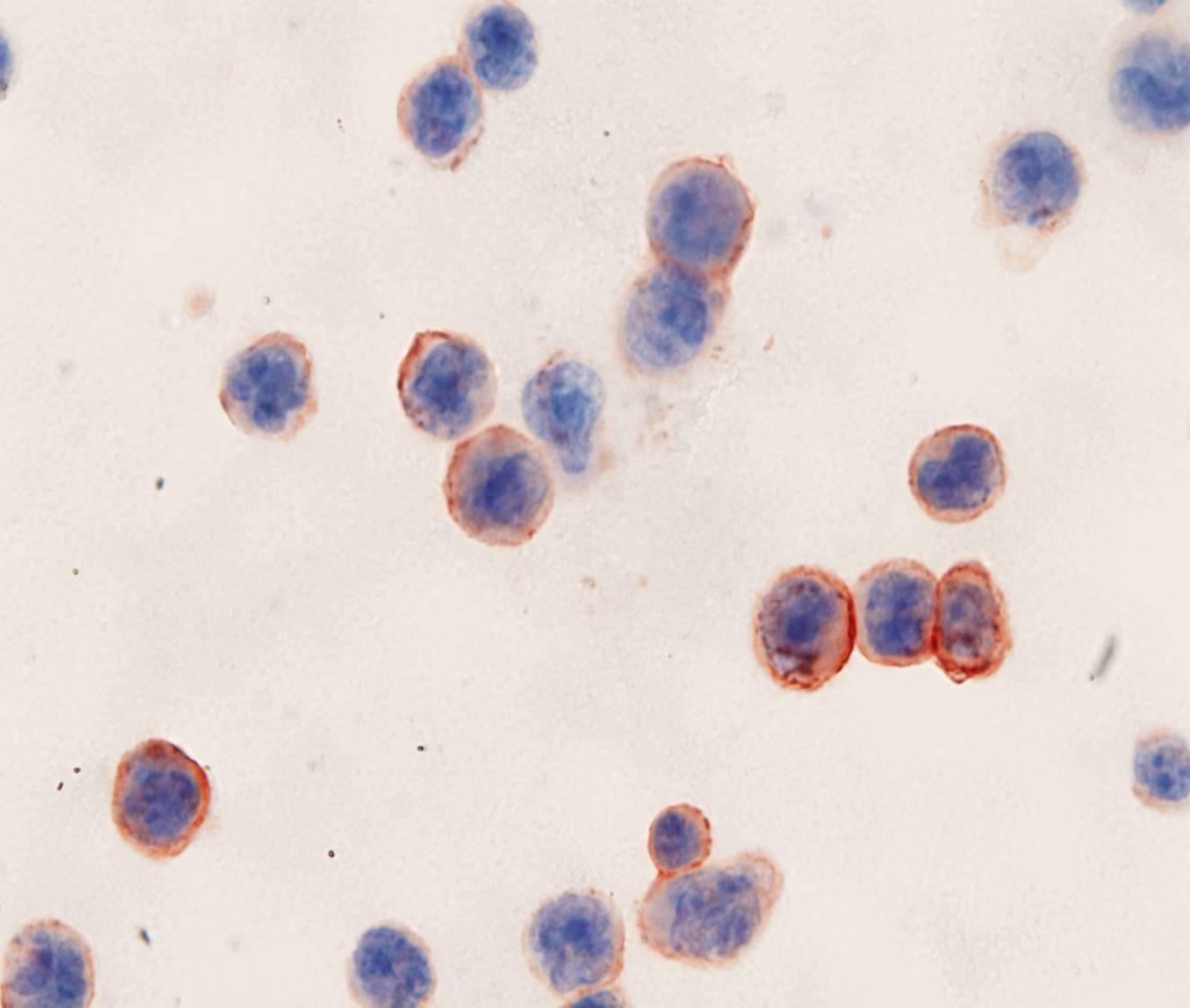
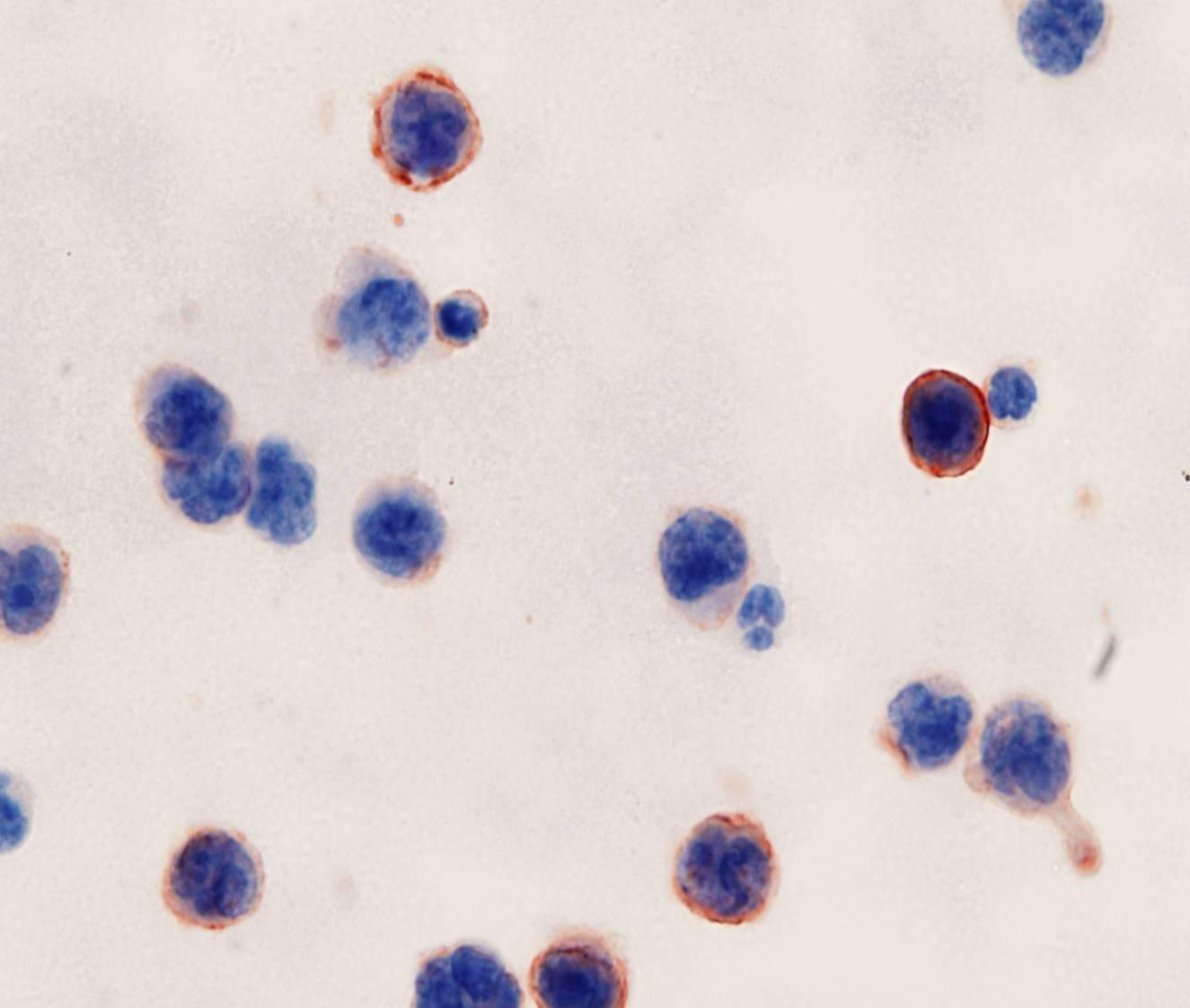
Malignant effusions are uncommon in Hodgkin lymphoma. The cytologic hallmark is the Reed-Sternberg cell, a large multinucleated cell with huge inclusion-like nucleoli. Mononuclear variants are also present, together with a mixed population of inflammatory cells including lymphocytes, plasma cells, histiocytes, eosinophils and neutrophils.
Immunostains on Cell block for CD30, CD15, PAX5 and ALK1 along with EBER ISH are useful diagnostic tools.
Other hematopoietic malignancies may involve the serosal cavities, such as acute lymphoblastic and myeloblastic leukaemias and chronic leukaemias. Flow cytometry is the method of choice to subclassify the neoplastic population

Metastatic sarcoma
Virtually all sarcomas can metastasize to the serosal surfaces, although they do much less frequently than carcinomas and lymphomas. In cytologic preparations, sarcoma cells are large or small, often spindle-shaped, and may appear as isolated cells or tissue fragments. Immunostains for CD31, CD34, S100, PGP9.5, CD56 Desmin and SMA can help to suggest the histotype.