This content is also available in:
![]() English
English ![]() Italiano
Italiano ![]() Español
Español ![]() Čeština
Čeština ![]() Magyar
Magyar
B??d w skryningu i potrzeba zapewnienia jako?ci
- Badanie cytologiczne szyjki macicy jest powszechnie stosowane dla wykrywania raka szyjki w najwcze?niejszych stadiach rozwoju, gdy leczenie jest najbardziej efektywne.
- Ostatnie badania wykaza?y, ?e badanie to mo?e uratowa? wiele istnie? ludzkich.
- Aby badanie to by?o skuteczne, wymaz z szyjki macicy musi by? pobrany starannie, rozmaz prawid?owo wykonany i opracowany technicznie a preparat analizowany i oceniony w pracowni z wysokim stopniem dok?adno?ci.
- Modu? ten wyja?nia, w jaki sposób osi?gn?? i utrzyma? wysoki standard funkcjonowania pracowni cytologicznej.
Zapewnienie jakosci jest nieodzowne dla zmniejszenia ryzyka bledów w cytologii szyjki macicy.
Istnieja 3 glówne typy bledów:
- B??dy zwi?zane z pobieraniem materia?u.
- B??dy zwi?zane z procesem laboratoryjnym.
- B??dy zwi?zane z interpetacj?.
Do 10% rozmazów pochodzacych od kobiet ze zmianami przedrakowymi lub wczesnym rakiem inwazyjnym szyjki macicy moze nie zawierac nieprawidlowych komórek. Istnieja trzy mozliwe wyjasnienia tej sytuacji:
- B??dy w pobieraniu i wykonywaniu rozmazu:
- Obszar strefy transformacji nie zosta? wystarczaj?co obj?ty w trakcie pobierania materia?u
- Nieprawid?owe komórki nie zosta?y przeniesione ze szpatu?ki na szkie?ko
- Zmiana CIN mo?e by? ma?a i/lub wysoko zlokalizowana w kanale szyjki macicy, poza zasi?giem szpatu?ki
- B??y w utrwalaniu i opracowaniu technicznym rozmazu:
- Morfologia komórek nie jest wystarczaj?co zachowana
- Stosunek j?drowo/cytoplazmatyczny zaburzony
- Obrysy j?dra i struktura chromatyny s?abo zachowana
- Blade wybarwienie j?dra i brak kontrastu j?dro/cytoplazma
- B??d w oznaczaniu preparatu
- B??dy w interpretacji rozmazu
- Spadek koncentracji w czasie skryningu
- Przyzwyczajenie – Pod?wiadomy proces, w którym mózg ignoruje powtarzaj?cy si? sygna?.
- Rozpraszanie uwagi w trakcie skryningu (rozmowa telefoniczna)
- Niedostateczny skryning ca?ego preparatu
- Zm?czenie (skrining zbyt du?ej liczby preparatów)
- Niewystarczaj?ce wyposa?enie optyczne mikroskopu lub
- B??d w trakcie pisania wyników
Pitfalls of Diagnosis
False negative reports are issued when the cytologist fails to detect abnormal cells which are present in the smear .There have been several studies to determine the characteristics of false negative smears. These have shown that the risk of a false negative smear report being issued is very high if the smear contain relatively few ( < 50 ) abnormal cells. Unfortunately studies have also shown that the majority of false negative smear reports are issued in cases where the smears contain a very large number of abnormal cells indeed. In fact , in retrospective studies of women who have presented with invasive cancer it has been found that up to three or more consecutive false negative reports have been issued over a period of several years before invasive cancer was diagnosed . False negative reports are particularly harmful because they result in failure to diagnose or treat the patient’s cancer.
False Positive reports are issued when the negative smears are reported to contain abnormal cells . In these cases the patient may undergo unnecessary surgical procedure and may be alarmed unnecessarily.
A number of conditions have been recognised which may give rise to problems of interpretation leading to a false positive diagnosis. These so called pitfalls in diagnosis are listed and several are illustrated below
Pitfalls in diagnosis
- Small cell dyskariosis
- Follicular lymphocytic cervicitis
- CIN3 minibiopsies ( microbiopsies ) or CIN involving crypts
- Discrete small keratinised cells
- Endometriosis , tubo endometrioid metaplasia
- Lower segment endometrium
- Immature metaplastic cells
- Histiocytes
- radiation changes
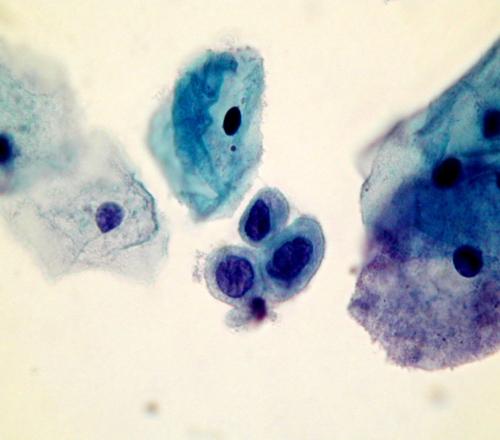
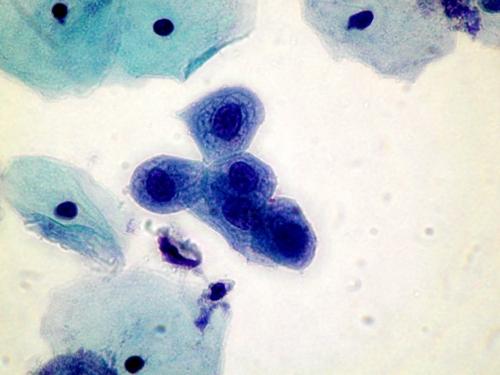
squamous cells is marked but the nuclear structure is bland and the cytoplasm abundant. It is important to take note of the clinical history when interpreting a smear.
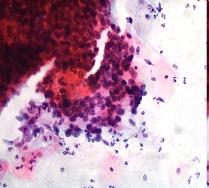
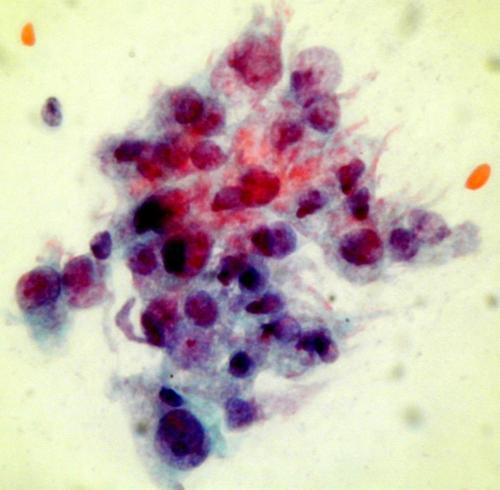
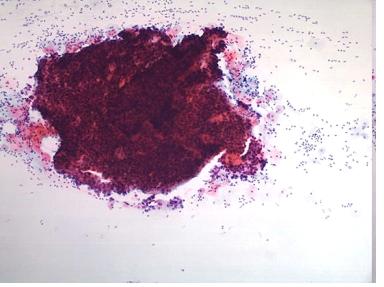
A dense cluster of poorly differentiated malignant squamous cells from a case of invasive squamous carcinoma . High power microscopy of the edge of the cluster reveals the crowded overlapping hyperchromatic nuclei which vary in shape and size and have abnormal chromatin content.
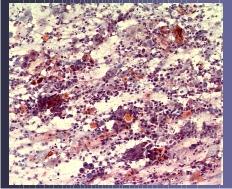
UWAGA
Do 45% rozmazów pochodzacych od kobiet z zaawansowanym rakiem moze nie zawierac komórek rakowych. Zdarza sie tak dlatego, ze zmiany sa czesto martwiczo zmienione i owrzodziale, a wówczas rozmaz zawiera wylacznie krew neutrofile i masy martwicze (tzw. diathesis maligna). Cytotechnicy moga zminimalizowac ten problem przez systematyczna ocene rozmazu pod katem jego adekwatnosci i informowanie osoby pobierajacej wymaz o jakosci rozmazu.