This content is also available in:
![]() English
English ![]() Español
Español
L’errore nello screening e la necessità di un controllo di qualità
- Lo striscio con il metodo di Papanicolaou viene eseguito in tutto il mondo al fine di individuare I carcinoma cervicali nelle fasi iniziali quando il trattamento risulta più efficace.
- Recenti studi hanno mostrato come gli strisci cervicali possono salvare molte vite.
- Al fine di ottenere un test efficace la cervice deve essere campionata con cura, lo striscio preparato e processato con cura e il vetro analizzato e refertati nel laboratorio con una grande accuratezza.
- Questo modulo spiega come raggiungere e mantenere alti livelli di efficienza in un laboratorio citologico.
La garanzia di qualità è essenziale per ridurre il rischio di errori nella citologia cervicale
Ci sono tre tipi di errori:
- Errori nel effettuare lo striscio.
- Errori nella processazione nel laboratorio.
- Errori nella interpretazione.
Fino al 10% degli strisci di donne con cancro cervicale pre-invasivo o nelle prime fasi può non contenere cellule atipiche.
Ci sono tre possibili spiegazioni per questa ragione:
- Errors of smear taking:
- The area of the transformation zone was not adequately sampled
- The abnormal cells were not transferred from spatula to slide
- The CIN lesion may be small and/or high in the endocervical canal beyond the reach of the spatula
- Errors of fixation and processing:
- Cell morphology not clearly displayed
- Nuclear/ cytoplasmic ratios distorted
- Nuclear outline and chromatin structure poorly displayed
- Pale nuclear staining and loss of nuclear/ cytoplasmic contrast
- Clerical error in mislabeling of slide
- Errors in the interpretation of the smear:
- Loss of concentration when screening
- Habituation- A subconscious process by which the brain ignores a repeated signal
- Distraction from screening (a telephone call)
- Failure to screen the whole slide
- Fatigue (screening too many slides at a sitting)
- Unsatisfactory microscope optics or laboratory ergonomics
- Clerical error in recording results
Referto con un falso negativo o con un falso positivo
Un referto con un falso negativo viene fatto quando il citologo non riesce a individuare cellule atipiche nello striscio.
Un referto con un falso positivo viene fatto quando uno striscio negativo viene refertato come contenete cellule atipiche
False negative reports are particularly harmful because for the patient because they result in failure to diagnose or treat the patient’s cancer.
NOTA:
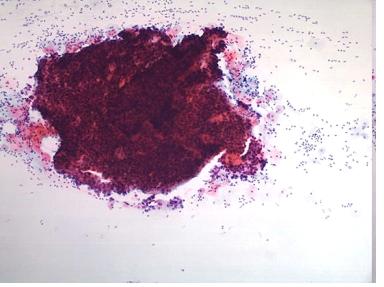
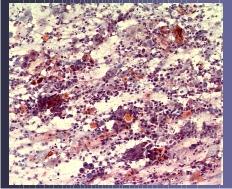
Fino al 45% di strisci di donne con carcinoma invasivo avanzato possono non contenere cellule atipiche. Questo perché le lesioni sono necrotiche e ulcerate, e lo striscio contiene interamente sangue, polimorfonucleati, detriti necrotici (chiamate anche diatesi maligne). I citotecnici possono ridurre questi problemi valutando sistematicamente gli strisci per la loro adeguatezza e segnalando a chi effettua gli strisci la qualità degli strisci stessi.
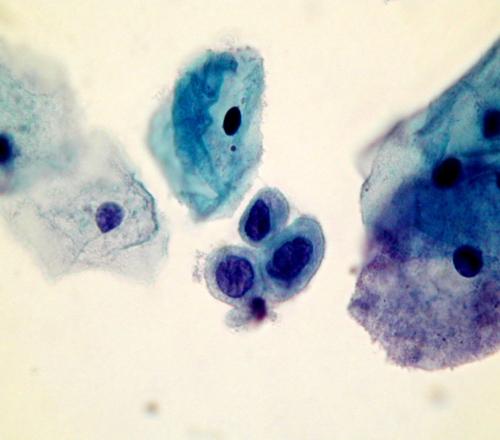
Pitfalls in diagnosis
- Small cell dyskariosis
- Follicular lymphocytic cervicitis
- CIN3 minibiopsies ( microbiopsies ) or CIN involving crypts
- Discrete small keratinised cells
- Endometriosis , tubo endometrioid metaplasia
- Lower segment endometrium
- Immature metaplastic cells
- Histiocytes
- radiation changes
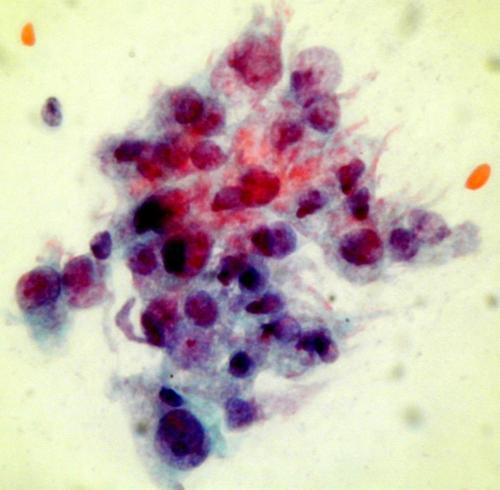
squamous cells is marked but the nuclear structure is bland and the cytoplasm abundant. It is important to take note of the clinical history when interpreting a smear.
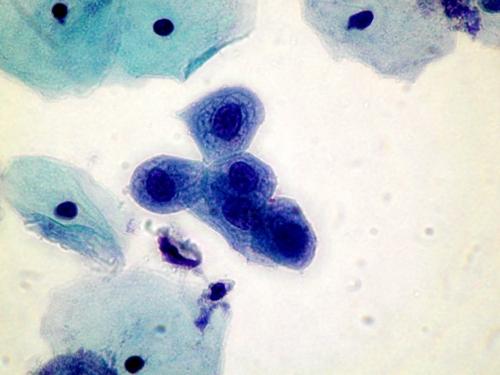
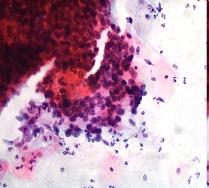
A dense cluster of poorly differentiated malignant squamous cells from a case of invasive squamous carcinoma . High power microscopy of the edge of the cluster reveals the crowded overlapping hyperchromatic nuclei which vary in shape and size and have abnormal chromatin content.