This content is also available in:
![]() English
English ![]() Italiano
Italiano ![]() Español
Español ![]() Čeština
Čeština ![]() Polski
Polski
Az elõszürés hibái és a minõségbiztosítás szükségessége
A Pap teszt világszerte hatékony korai stádiumban a méhnyakrák felismeréséhez, amikor a kezelés a leghatásosabb.
A legújabb tanulmányok kimutatták, hogy a kenet vizsgálat számos életet ment meg.
A teszt hatásossága függ ugyanakkor a cervicalis mintavétel gondosságától, a kenet készítésétõl és korrekt kikenésétõl, valamint a laboratórium pontos, korrekt kenet vizsgálatától és értékelésétõl.
Ez a modul elmagyarázza, hogyan érhetõ el és tartható fenn a citológiai laboratórium teljesítménye magas követelmény szinten.
A minõségbiztosítás elengedhetetlen a cervicalis citológia hibáinak minimalizálásában
Három fõ hiba:
1. Hibák a kenetvételkor
2. Hibák a laboratóriumi feldolgozás során
3. Hibák az interpretálásban
Preinvaziv vagy korai invaziv rák esetén 10%-ot is elérhet azon kenetek aránya, melyek nem tartalmaznak kóros sejteket. Ennek három lehetséges oka (magyarázata) ismert:
-
A kenetvétel hibái Fixálás és festés során elõforduló hibák értékelés hibái 1 átmeneti zona sejtjei nincsenek jelen 1 Sejt morfológia elmosott 1 Dekoncentrált, figyelmetlen elõszurés 2 A kóros sejtek aq spatulán maradtak, nem kerültek át a tárgylemezre 2 Mag/plazma arány elmosott 2 “Hozzászokás”: tudatalatti folyamat, melynek során az agyunk ismétlõdõ jelenségeket nem vesz figyelembe 3 A CIN lézió vagy kicsiny, vagy oly magasan van az endocervixben, hogy a spatula nem éri el 3 Mag membrán és struktura nehezen megitélhetõ 3 Félbehagyott elõszurési folyamat ( pl. telefonhivás miatt) 4 Halvány magfestõdés a mag/cytoplazma kontraszt elmosott 4 Nem került az egész kenet átvizsgálásra 5 Téves jelzés a tárgylemezen ( adminisztrációs hiba ) 5 Fáradtság ( tul sok kenet vizsgálata egy ülésben ) 6 Rossz optikájú mikroszkóp, szegényes ergonomia a laborban 7 Adminisztrációs hiba az adatok rögzítése során
Pitfalls of Diagnosis
False negative reports are issued when the cytologist fails to detect abnormal cells which are present in the smear .There have been several studies to determine the characteristics of false negative smears. These have shown that the risk of a false negative smear report being issued is very high if the smear contain relatively few ( < 50 ) abnormal cells. Unfortunately studies have also shown that the majority of false negative smear reports are issued in cases where the smears contain a very large number of abnormal cells indeed. In fact , in retrospective studies of women who have presented with invasive cancer it has been found that up to three or more consecutive false negative reports have been issued over a period of several years before invasive cancer was diagnosed . False negative reports are particularly harmful because they result in failure to diagnose or treat the patient’s cancer.
False Positive reports are issued when the negative smears are reported to contain abnormal cells . In these cases the patient may undergo unnecessary surgical procedure and may be alarmed unnecessarily.
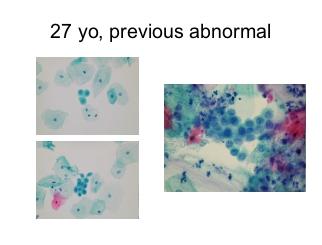
A number of conditions have been recognised which may give rise to problems of interpretation leading to a false positive diagnosis. These so called pitfalls in diagnosis are listed and several are illustrated below
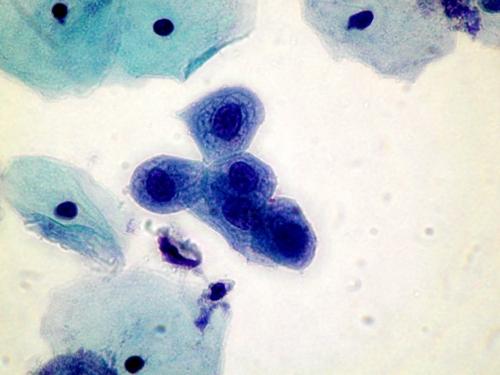
Pitfalls in diagnosis
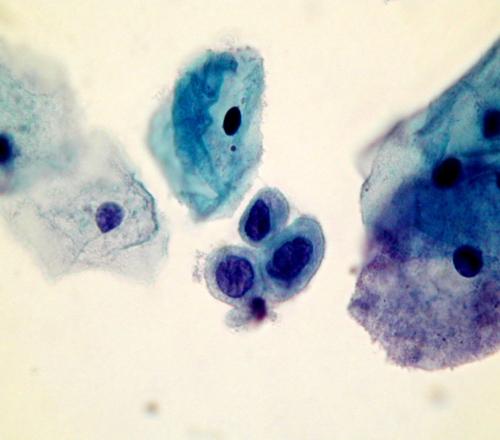
- Small cell dyskariosis
- Follicular lymphocytic cervicitis
- CIN3 minibiopsies ( microbiopsies ) or CIN involving crypts
- Discrete small keratinised cells
- Endometriosis , tubo endometrioid metaplasia
- Lower segment endometrium
- Immature metaplastic cells
- Histiocytes
- radiation changes
squamous cells is marked but the nuclear structure is bland and the cytoplasm abundant. It is important to take note of the clinical history when interpreting a smear.
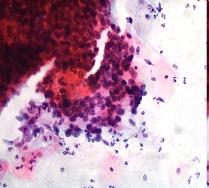
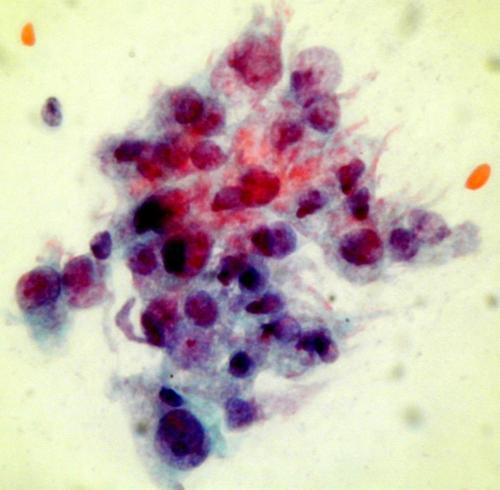
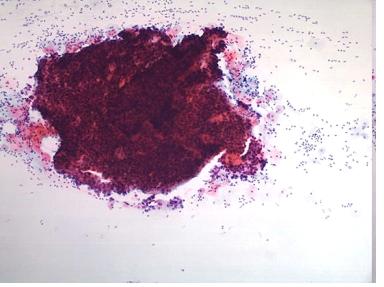
A dense cluster of poorly differentiated malignant squamous cells from a case of invasive squamous carcinoma . High power microscopy of the edge of the cluster reveals the crowded overlapping hyperchromatic nuclei which vary in shape and size and have abnormal chromatin content.
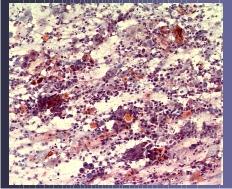
NOTE: Up to 45% of smears from women with advanced invasive cancer may not contain abnormal cells . This is because the lesions are often necrotic and ulcerating and the smear is comprised entirely of blood , polymorphs and necrotic debris (the so called malignant diathesis) Cytotechnologists can minimise this problem by systematically evaluating the smears for their adequacy and advising smear takers of the quality of their smears.