This content is also available in:
![]() Español
Español ![]() Čeština
Čeština ![]() Magyar
Magyar ![]() Polski
Polski ![]() Türkçe
Türkçe
- Squamous cell changes
- Bronchial cell changes
- Bronchial reserve cell hyperplasia
- Repair
- Tipe II pneumocytes hyperplasia
Squamous cells
Squamous cells from the upper respiratory tract often contaminate specimens from the lower tract. Inflammatory conditions of the mouth may exfoliate atypical squamous cells which should not be misdiagnosed as squamous cell carcinoma. Cancer involving head and neck structures could also lead to false-positive diagnoses.
Bronchial cell changes
Bronchial cell changes occur in response to noxious stimuli such as severe inflammations, radiotherapy, chemotherapy. Ciliated columnar cells may have enlarged nuclei with coarse chromatin and large nucleoli. Multinucleation is common. Large papillary groups of bronchial cells (Creola bodies) may be seen in chronic airway diseases such as asthma. Goblet cells may also proliferate and large sheets or papillary clusters of goblet cells may exfoliate; goblet cell hyperplasia can mimic a bronchioloalveolar carcinoma.
Bronchial cell hyperplasia must not be misdiagnosed as adenocarcinoma. Benign bronchial cells are ciliated and a spectrum of epithelial changes ranging from benign to markedly atypical is usually observed, rather than two distinct cell populations.
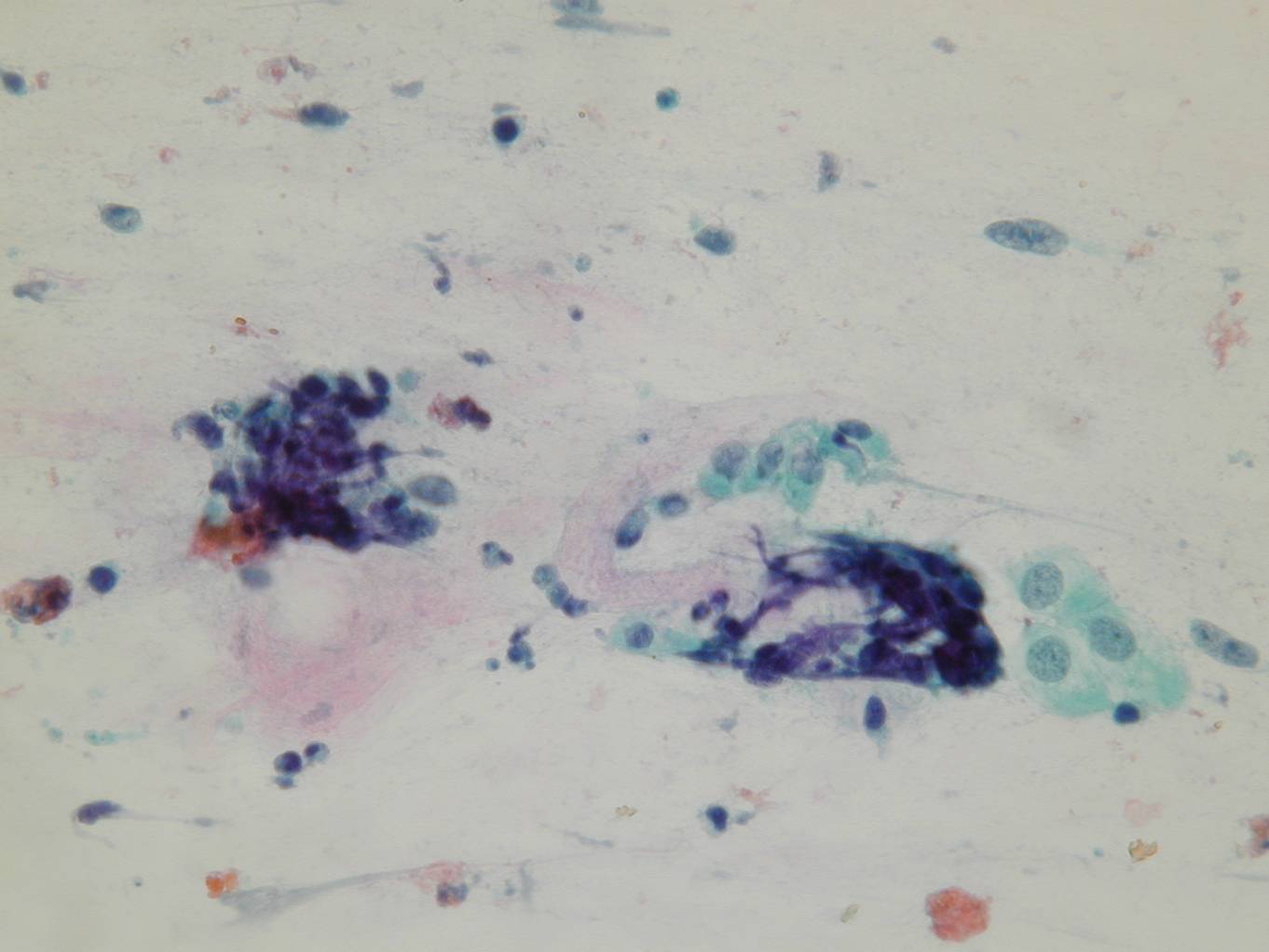
Bronchial reserve cell hyperplasia
Bronchial reserve cells proliferate when the surface epithelium is shed during lung injury. In cytologic smears, hyperplastic reserve cells are observed as small, hyperchromatic cells, with smudged chromatin and scant cytoplasm; they are tightly packed and show nuclear molding.
They are distinguished from small cell carcinoma by their greater cohesiveness, their very small size and lack of mitoses and necrosis.
Repair
Repair atypia may be observed after re-epithelialization of an ulcer caused by insults such as trauma, radiation, infections.
Flat, cohesive sheets of cells with abundant cytoplasm and large, often hypochromatic nuclei, with conspicuous nucleoli, are usually observed.
Tipe II pneumocytes hyperplasia
Because type II pneumocytes function as alveolar reserve cells, they proliferate after lung injury, such as pneumonia, sepsis, pulmonary embolus with infarction, chemotherapeutic drugs, radiation therapy, interstitial lung disease.
In cytologic smears they appear as single cells or clusters of cells with large nuclei, coarse chromatin and prominent nucleoli, with scant to abundant cytoplasm. These cells may resemble an adenocarcinoma when floridly hyperplastic, as in diffuse alveolar damage; it is therefore helpful the clinical history of respiratory distress. Type II pneumocytes are not present in BAL specimens more than 1 month after the onset of acute lung injury.