This content is also available in:
![]() Español
Español ![]() Čeština
Čeština ![]() Magyar
Magyar ![]() Polski
Polski
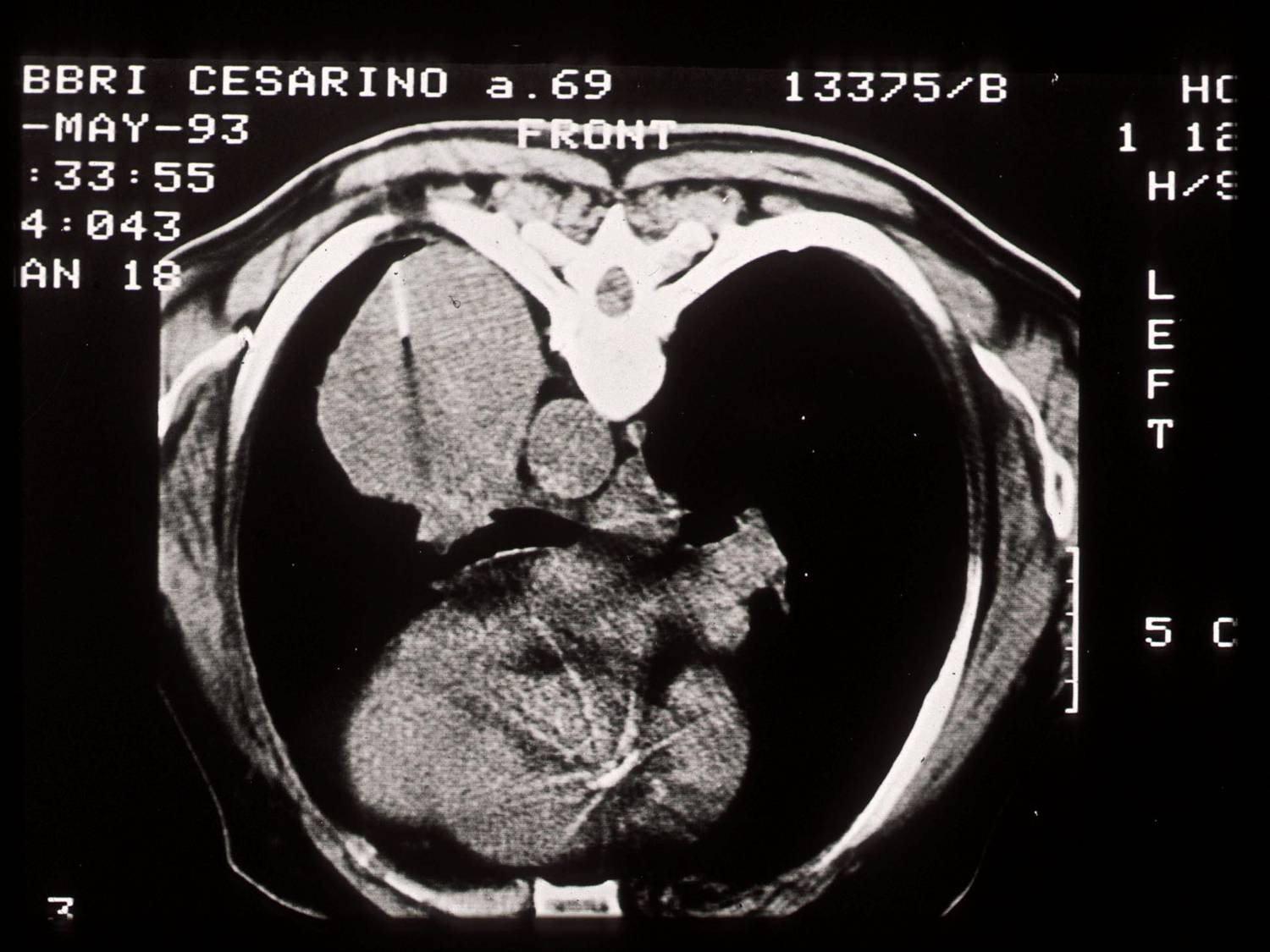
The indication for transthoracic FNA is the presence of a pulmonary mass. This method allows to spare many patients a more invasive surgical procedure. Indications to FNA also include subclassification of obvious malignant neoplasms and persistent lung infections. The most common complication is pneumothorax, requiring a drainage tube in 10% of the patients.
FNA is performed using CT or US guidance or fluoroscopy. Needle gauge ranges from 18 to 22 and many type of needle devices are available. One of the most used is the 22G Chiba needle; it requires repuncture if more than one pass is needed. Another choice is the coaxial needle, with a large-bore outer needle serving as the guide for a small-bore inner needle; once the outer needle is positioned, more than one aspiration can be performed by the inner needle.
A cytopathologist should attend the procedure to assess the adequacy of the material on-site.
Adverse indications
- patient refusing
- bleeding disorder
- controlateral pneumonectomy
- severe respiratory failure
- vascular malformations
- echinococcosis
Complications
- pneumothorax (mostly related to lenght of the procedure)
- haemorrage
- intrapulmonary hematomas
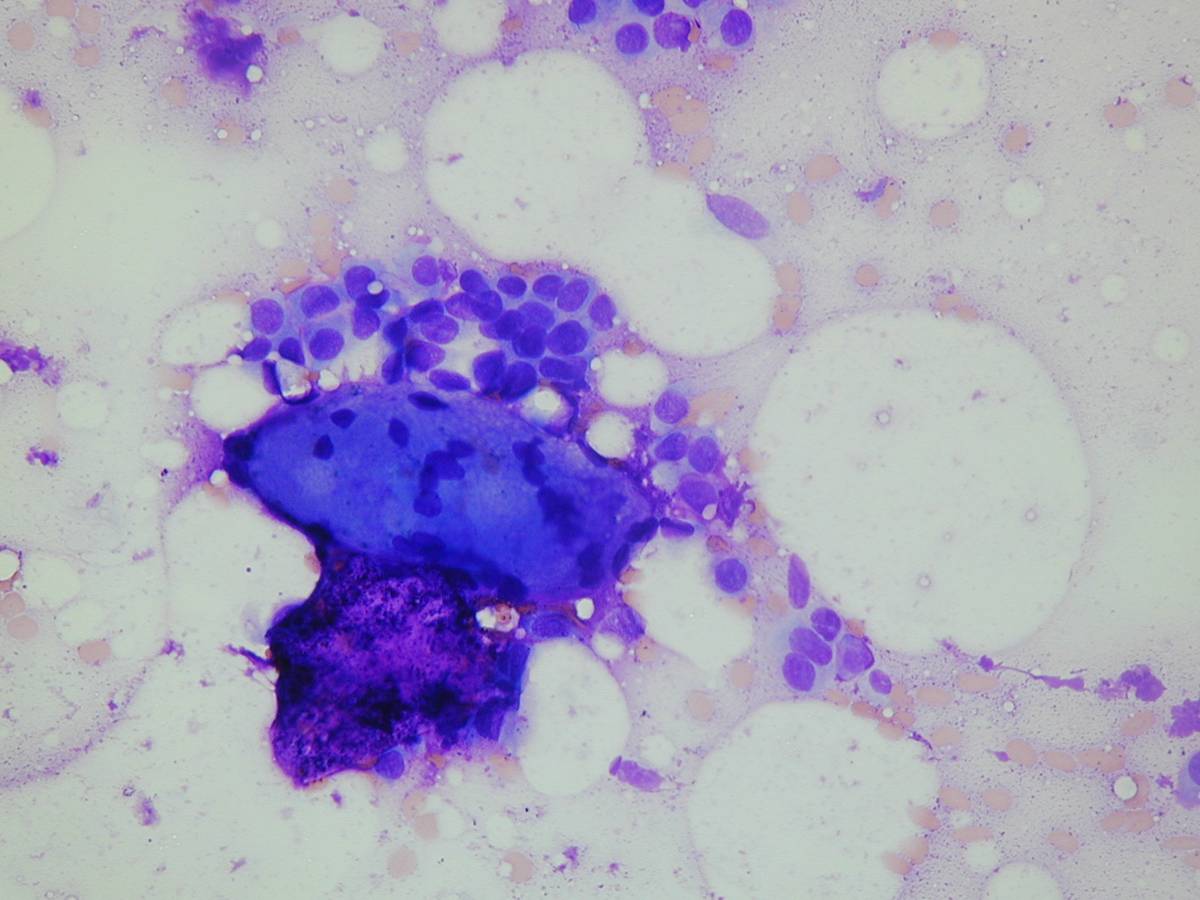
After direct smears are prepared, the needle is rinsed in a balance electrolyte solution, Saccomanno`s fixative, 50% ethanol or commercial preservative solution. This cellular suspension may be processed for microbiologic analysis, cytospins, thin-layer preparations, filters, cell blocks, cytogenetic analysis or elecron microscopy. Formalin-fixed cell blocks are very useful for histochemical and immunohistochemical stains.
Potential contaminants of transthoracic FNA are cutaneous squamous cells, mesothelial cells, skeletal muscle, fibroconnective tissue, hepatocytes (in case of a diaphragmatic transgression).
Transthoracic FNA is a reliable way to diagnose many lung neoplasms and is often able to distinguish between small cell and non-small cell lung carcinoma. A repeat aspiration or tissue biopsy are recommended when a specific diagnosis cannot be made with certainty.