Hepatocellular carcinoma (HCC)
Hepatocellular carcinoma (HCC) accounts for 90% of all primary cancers of the liver. It is more common in Africa and Asia than in United States and Europe, where most cases are seen in the setting of cirrhosis. Most patients are over 50 years old.
The tumor can present as a solitary nodule, as multiple nodules or as a diffuse liver enlargement. There is a wide range of differentiation, from well-differentiated tumors resembling normal liver, to poorly differentiated ones with marked nuclear pleomorphism and tumor giant cells. Elevated serum levels of alpha-fetoprotein are present in many cases.
Detection of HCC at an early stage improves possibility of treatment. HCC > 5 cm have poor prognosis. There are no histologically agreed criteria on the diagnosis of tumors < 1.5 cm.
The earliest identifiable HCC
Macroregenerative nodules are parenchymal nodules > 1cm in the setting of cirrhosis and contain portal tracts. Progression to neoplasia is associated with loss of reticulin structure, capillarised microvasculature, thickening of trabeculae, microacinar structures, increased mitotic activity and nuclear pleomorphism
Liver cell dysplasia
- Large cell dysplasia: individual hepatocytes larger than the surrounding ones but with a preserved
- N/C ratio
- Small cell dysplasia: only slightly larger than surrounding hepatocytes, but with high N/C ratio, increased cell density, thickened cell plates, rarefaction of reticulin
Small cell dysplasia probably represents preneoplastic change, however HCC becomes progressively less differentiated and its morphological relationship with dysplasia less obvious.
Cytologic criteria for malignancy
- Architecture: irregular cell arrangements, thick trabeculae, pseudoglandular pattern, naked nuclei,
- no or few ductal cells, dirty background
- Nuclei: high N/C ratio, multinucleation, irregular membranes, coarse chromatin, very large nucleoli
- Cytoplasm: evidence of bile production, granular cytoplasm, vacuolation
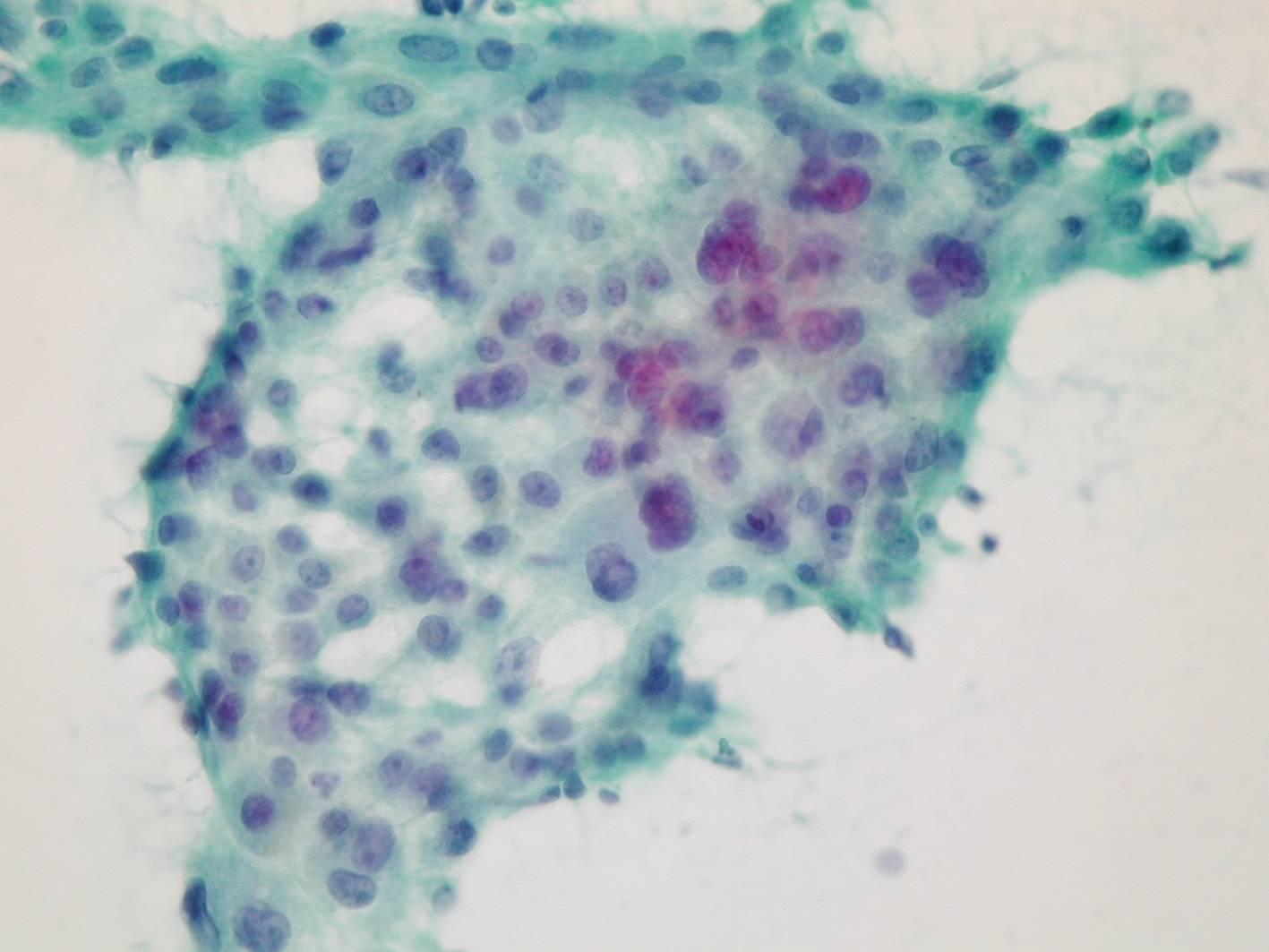
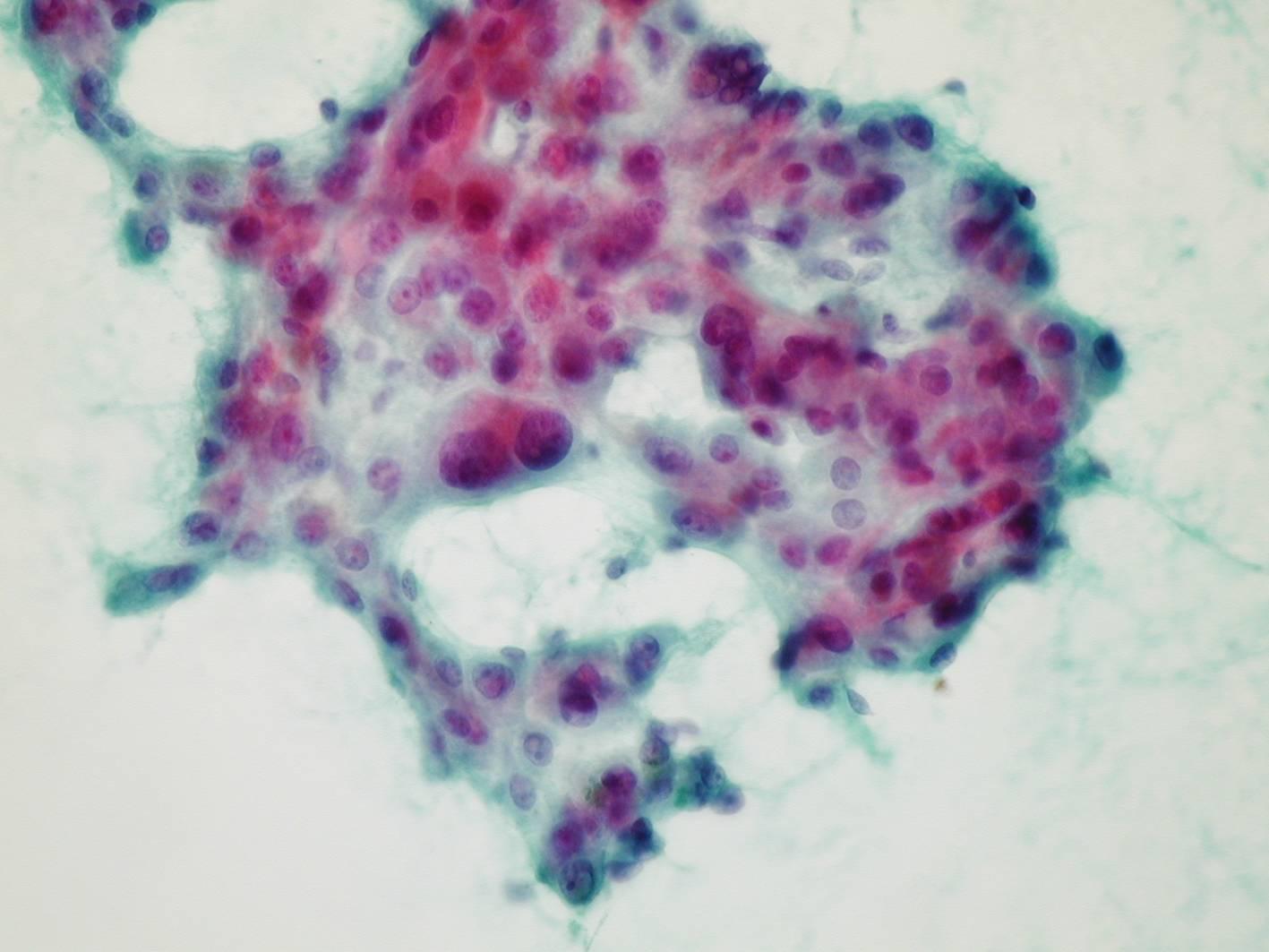
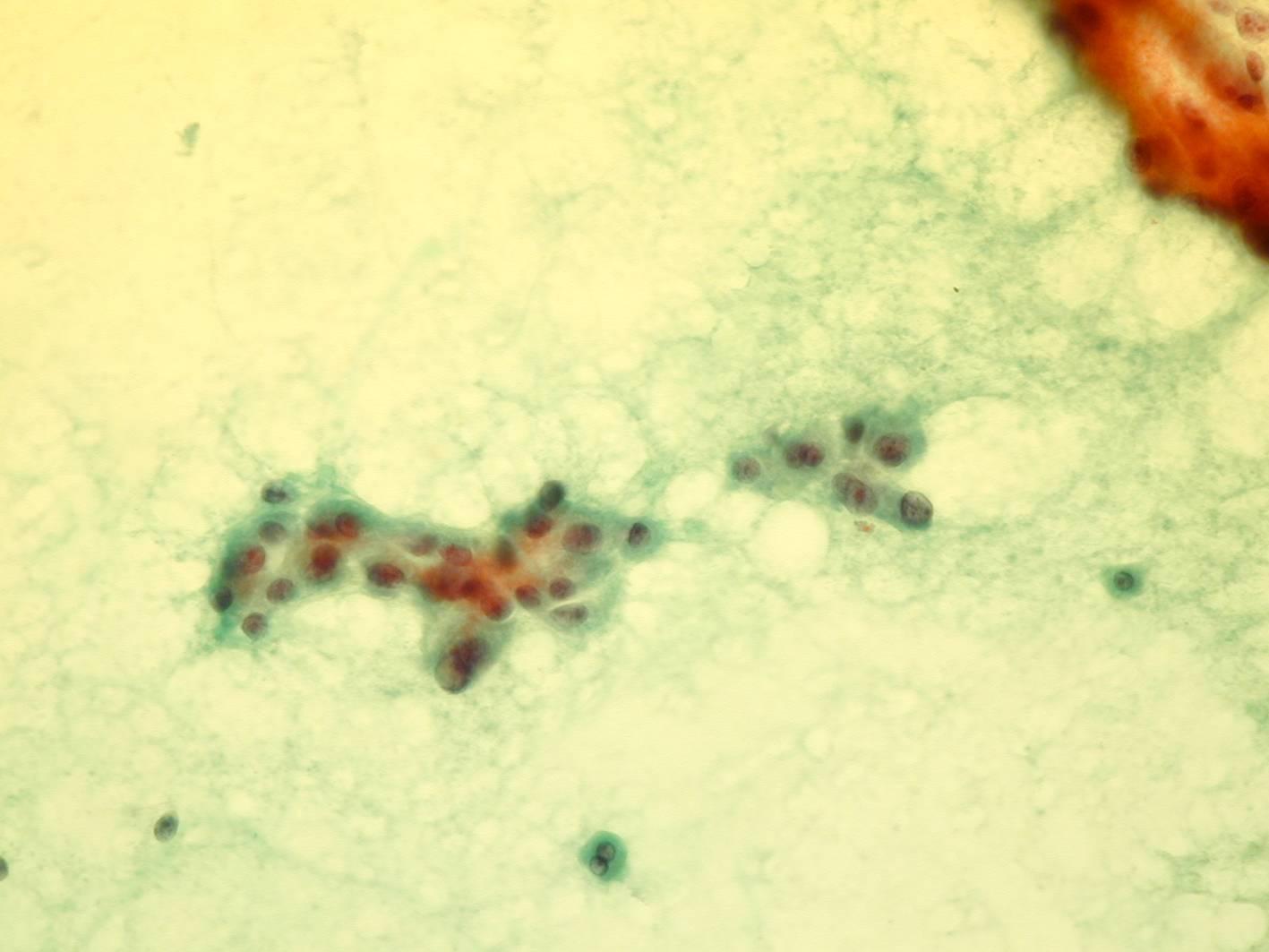
Cytologic diagnostic features (well-differentiated HCC)
- Spindle-shaped endothelial cells surrounding thickened cords of neoplastic hepatocytes
- Increased N/C ratio
- Granular cytoplasm with bile or hyaline globules (red with Papanicolaou and blue with Romanowsky stains)
- Large round nuclei, prominent nucleoli
- Intranuclear pseudoinclusions
- Large naked nuclei
Differential diagnosis (well-differentiated HCC)
- Regenerating nodules in cirrhosis
- Hepatic adenoma
- Focal nodular hyperplasia
Atypical naked nuclei, increased N/C ratio, cellular monomorphism, mitoses and loss of bile ducts are typical of HCC; endothelium is particularly specific for HCC. CD34 reactivity can be useful to differentiate HCC from cirrhosis. Immunoreactivity for mutant p53 expression increases with increasing grades of HCC.
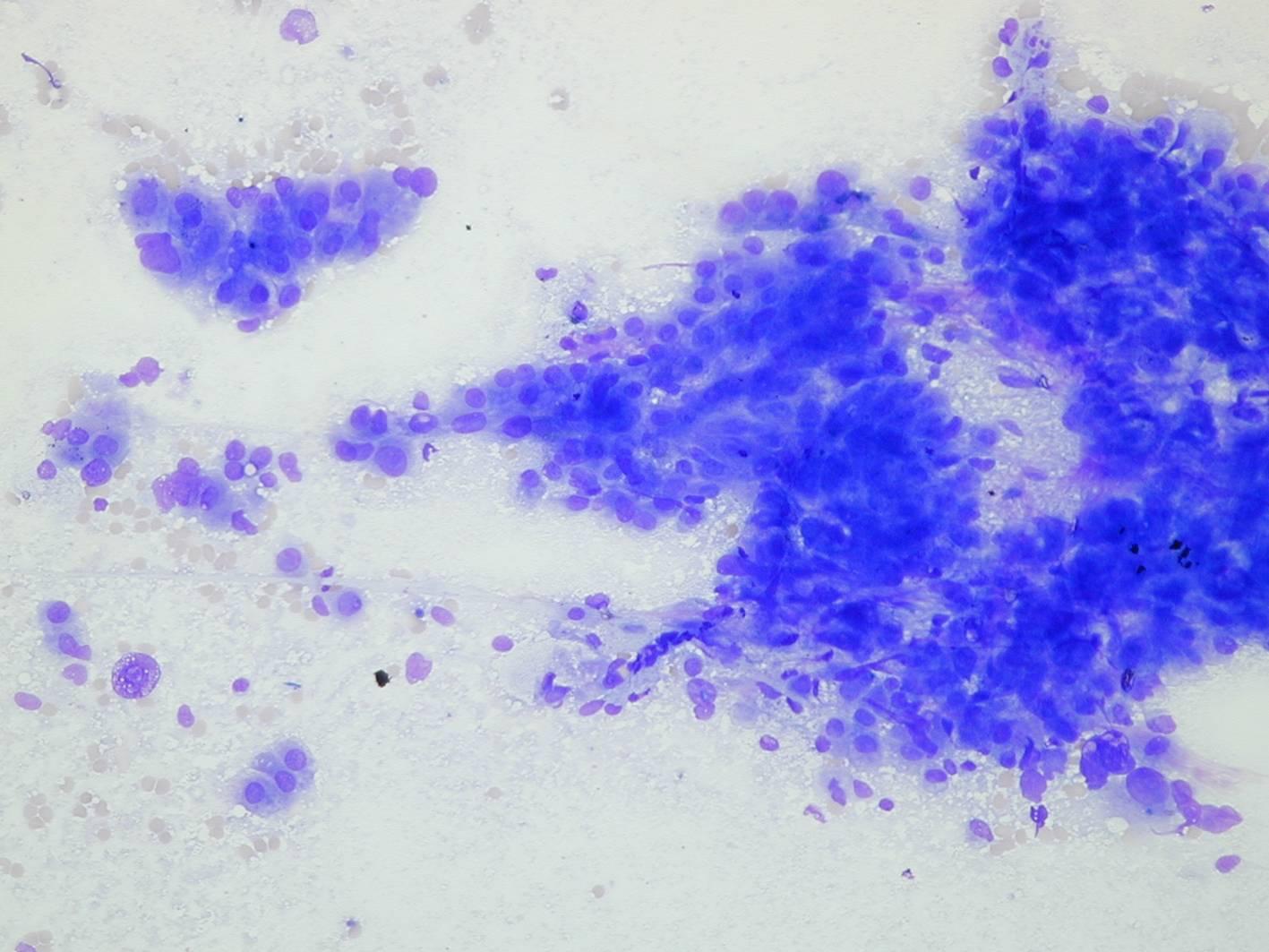
Cytologic diagnostic features (moderately and poorly differentiated HCC)
- Highly cellular smears
- Single cells, cords, nests, tubules, or sheets
- Moderate to marked pleomorphism
- Atypical mitoses
- Spindle-shaped cells
- Tumor giant cells
- Clear cytoplasm in 10% of HCC (clear cell carcinoma)
Differential diagnosis (moderately and poorly differentiated HCC)
- Cholangiocarcinoma
- Metastatic carcinoma
These tumors can be difficult to distinguish by cytologic features alone. In addition, there are rare cases of combined HCC and cholangiocarcinoma. Histochemical and immunohistochemical studies may be necessary to distinguish some HCCs from metastatic tumors. Intracytoplasmic mucin is very uncommon in HCC, but present in many adenocarcinomas and in cholangiocarcinoma.

Fibrolamellar HCC
The fibrolamellar variant of HCC is usually seen in young patients who do not have cirrhosis. The prognosis is good. Dense bands of fibrosis surround large tumor cells with abundant eosinophilic cytoplasm.
Cytologic diagnostic features
- Large cells with abundant cytoplasm
- Large nuclei, very prominent nucleoli
- Mostly single cells or loose clusters
- Hyaline intracytoplasmic globules
- Bands of fibrosis
The tumor cells are much larger than normal hepatocytes, but the N/C ratio is lower than in the usual variant of HCC.