Benign conditions
Benign conditions Acute thyroiditis Subacute granulomatous (De Quervain`s) thyroiditis Chronic lymphocytic (Hashimoto`s) thyroiditis Riedel`s disease Multinodular goiter Radiation changes
Acute thyroiditis
Acute thyroiditis, a very rare condition due to bacterial infections, is usually diagnosed clinically, without the need for FNA. Aspirates are composed predominantly of neutrophils and inflammatory debris, and thyroid epithelial cells are scanty and degenerated.
Subacute granulomatous (De Quervain`s) thyroiditis
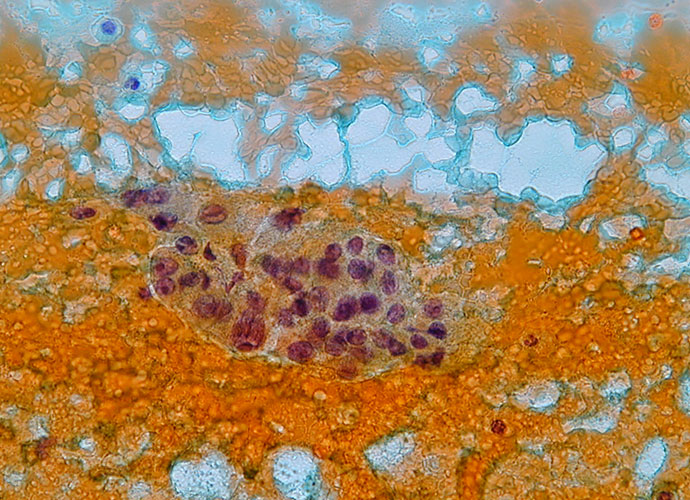
It is a rare self-limited disease, usually lasting several months, characterized by a painful enlargement of the gland. It is a granulomatous inflammatory condition which leads finally to fibrosis of the gland. Cytologic diagnostic features granulomas giant cells lymphocytes and neutrophils The cytologic specimens contain nodular aggregate of hystiocytes, lymphocytes and neutrophils. Epithelioid cells and […]
Chronic lymphocytic (Hashimoto`s) thyroiditis
This is an autoimmune disease in which the parenchima is virtually replaced by a lymphoid infiltrate with germinal centers, sometimes with a prominent fibrosis in longstanding disease. Several autoantibodies are identified in affected patients, such as antibodies against thyroid microsomal antigens and against TSH receptors. The gland is usually enlarged, painless, with or without nodularity. […]
Adequacy of the specimen
Specimens may be unsatisfactory due to obscuring blood, overly thick smears, air-drying of alcohol-fixed smears or an inadequate number of follicular cells. Specimens containing at least five groups of follicular cells, each composed of at least ten cells, are considered satisfactory for evaluation. With experience, the average unsatisfactory rate is about 5% to 10%. It […]
Fine needle aspiration (FNA)
Diagnostic tests in thyroid nodules Clinical history and examination are the first step to approach the investigation of the thyroid nodule; however they are not sufficiently accurate by themselves. Ultrasound examination, which can discriminate between a solid and a cystic nodule, does not reliably predict malignancy. Radionuclide imaging is not useful to identify malignant lesions: […]
Thyroid
On completion of this section the cytotechnologist should know: the anatomy and histology of the normal thyroid the role of the thyroid hormones and the control of their production the incidence of thyroid nodules and the diseases which can present as thyroid nodules the diagnostic tests in thyroid nodules the indications of thyroid fine needle […]
Anatomy and Physiology
Anatomy The thyroid is an endocrine organ situated in the neck. Its position, close to the thyroid cartilage gave the organ its name as thyroid is derived from the Greek word thyros, meaning shield it was originally considered to protect the larynx. Embryologically the thyroid develops at the base of the tongue from the […]
Thyroid nodules
Thyroid nodules Palpable thyroid nodules affect 4-7% of the adult population with female predominance, although it has been predicted that between 40-70% of adults may have clinically undetected nodules only identifiable by ultrasound or autopsy. The vast majority of these nodules are benign, with only 5-10% proving malignant. Clearly therefore surgical excision of all palpable […]
Classification of thyroid neoplasms
WHO classification of thyroid tumours (1988) I. Epithelial tumours Benign Follicular adenoma and variants Others including hyalinizing trabecular adenoma Malignant Follicular carcinoma including minimally invasive, widely invasive and poorly differentiated subtypes Papillary carcinoma and variants including papillary microcarcinoma, follicular variant and diffuse sclerosing variant Medullary carcinoma and variants including mixed medullary-follicular carcinoma Undifferentiated (anaplastic) carcinoma […]