This content is also available in:
![]() Español
Español
Pulmonary neuroendocrine tumors, which include also small cell carcinoma, have been classified by the World Health Organization into the following types: carcinoid tumor, atypical carcinoid tumor, large cell neuroendocrine carcinoma, and small cell carcinoma.
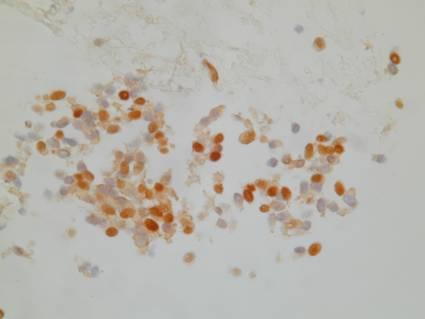
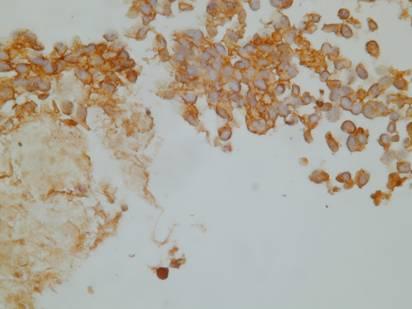
Ultrastructurally, all contain cytoplasmic dense-core granules. They variably stain positive with several immunohistochemical markers: chromogranin A (most specific), synaptophysin, neuron-specific enolase, Leu-7 (CD57). Other peptides may be present, such as ACTH, insulin, calcitonin, gastrin, VIP.
The large cell neuroendocrine carcinoma is composed of large cells with the nuclear features and the organoid growth pattern of a neuroendocrine neoplasm (and immunohistochemical and ultrastructural studies confirm its neuroendocrine nature), whereas the large cell carcinoma with neuroendocrine differentiation is indistinguished by light microscopy from a large cell undifferentiated carcinoma, but it shows immunohistochemical and ultrastructural features of neuroendocrine differentiation. The prognosis for patients with these tumors is poor.
Carcinoid tumor (typical carcinoid tumor)
These neuroendocrine tumors have a low metastatic rate and the prognosis is usually very good. They are usually centrally-located, often with a prominent endobronchial component; they are often covered by an intact respiratory epithelium and, as a result, sputum cytology is often negative.
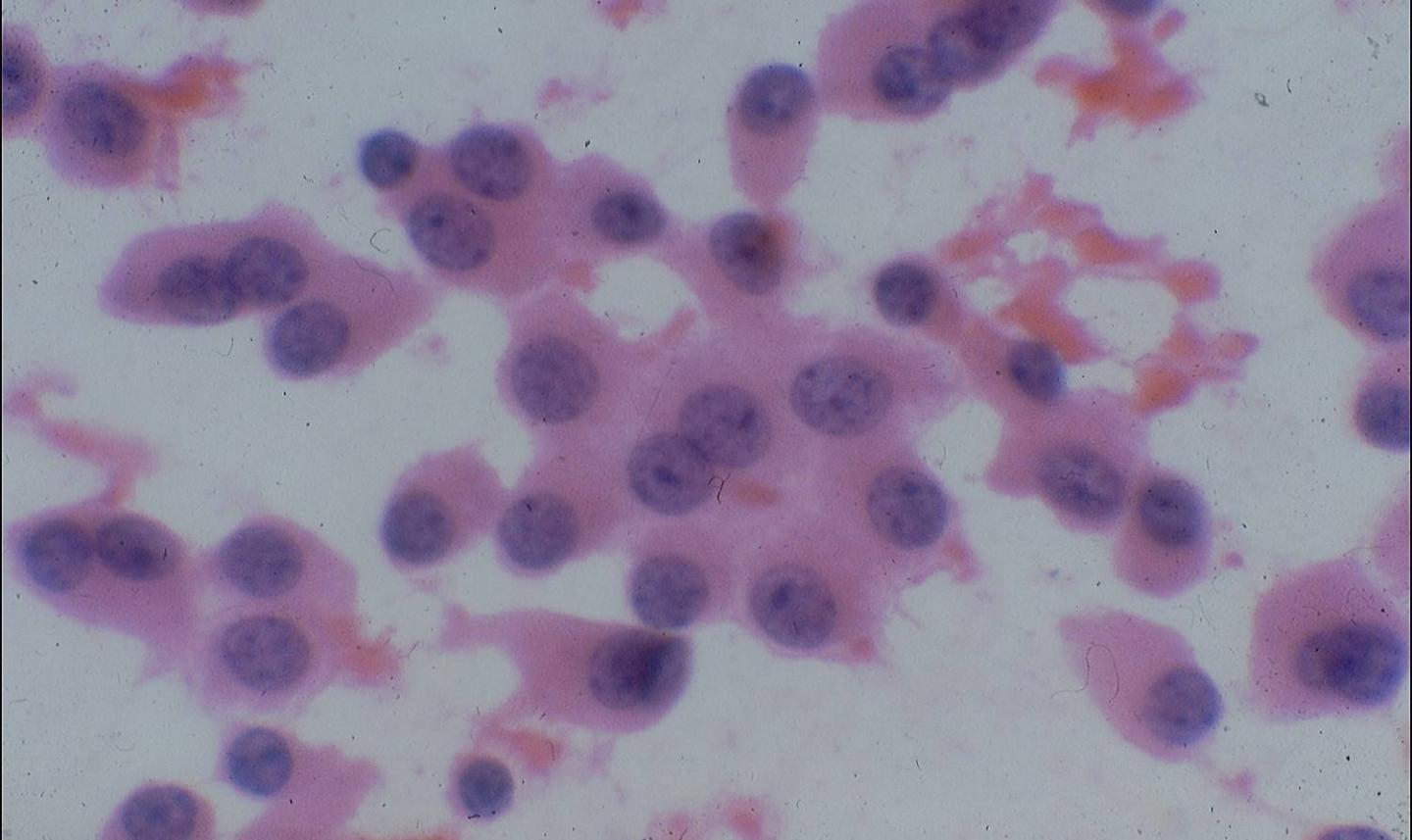
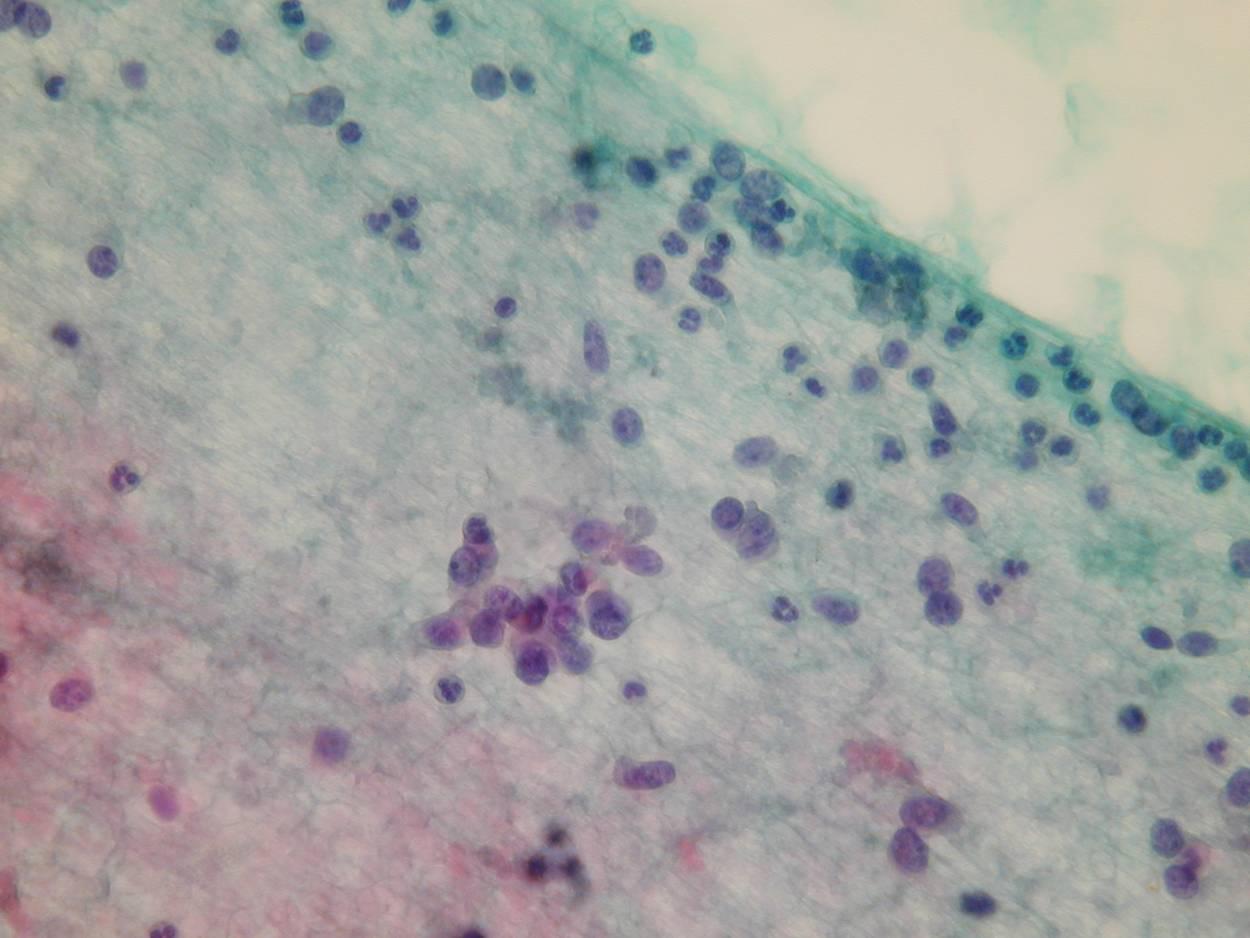
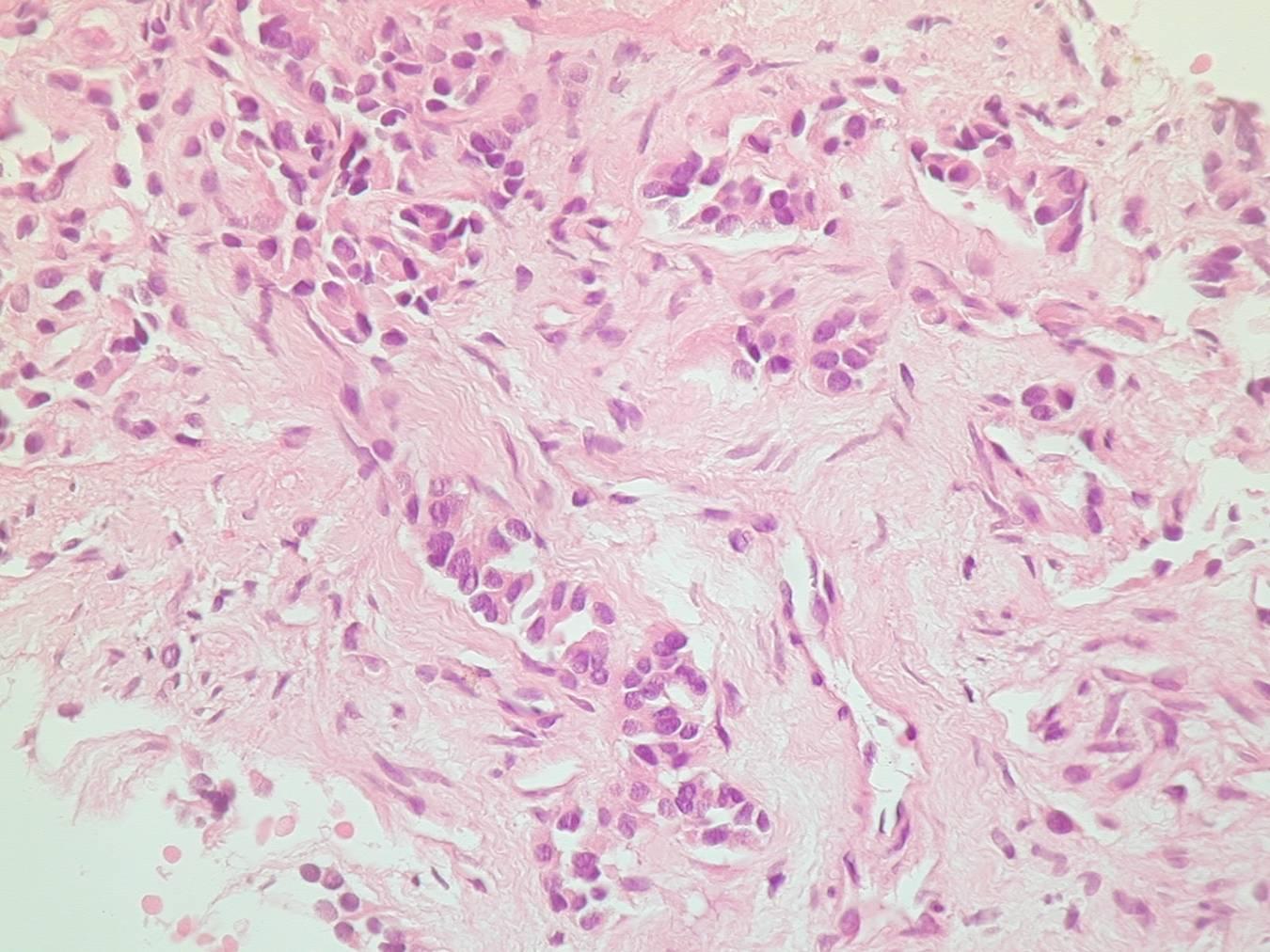
Cytologic diagnostic features
Loosely cohesive groups and single cells
Acinar or rosette-like structures
Round, columnar or plasmacytoid cells
Uniform, moderately granular nuclei, ‘salt and pepper’ chromatin pattern
Ample eosinophilic cytoplasm
Branching capillaries
Mitoses uncommon
Differential diagnosis
Benign bronchial epithelial cells
Adenocarcinoma
Small cell carcinoma
Atypical carcinoid
Lymphoma
Mesenchimal tumor (spindle cell carcinoid)
Because of their bland, monomorphous appearance, the cells of some carcinoid tumors could be mistaken for benign bronchial cells, but they are less cohesive, have more coarse chromatin and lack cilia. Because of the presence of rosettes in some carcinoid tumors, they could be mistaken for adenocarcinoma, which, however, usually show greater pleomorphism. Lymphoid cells are distinguished from carcinoid tumors because they have less cytoplasm and do not form clusters.
Carcinoid tumors are distinguished from atypical carcinoid and small cell carcinoma by the absence of mitoses and necrosis.
Atypical carcinoid tumor
Atypical carcinoid tumor (well-differentiated neuroendocrine carcinoma) is more aggressive than typical carcinoid tumor.
Cytologic diagnostic features
Cells similar to typical carcinoid
Disorganized growth pattern
Necrosis
Pleomorphism
Mitosis
Prominent nucleoli
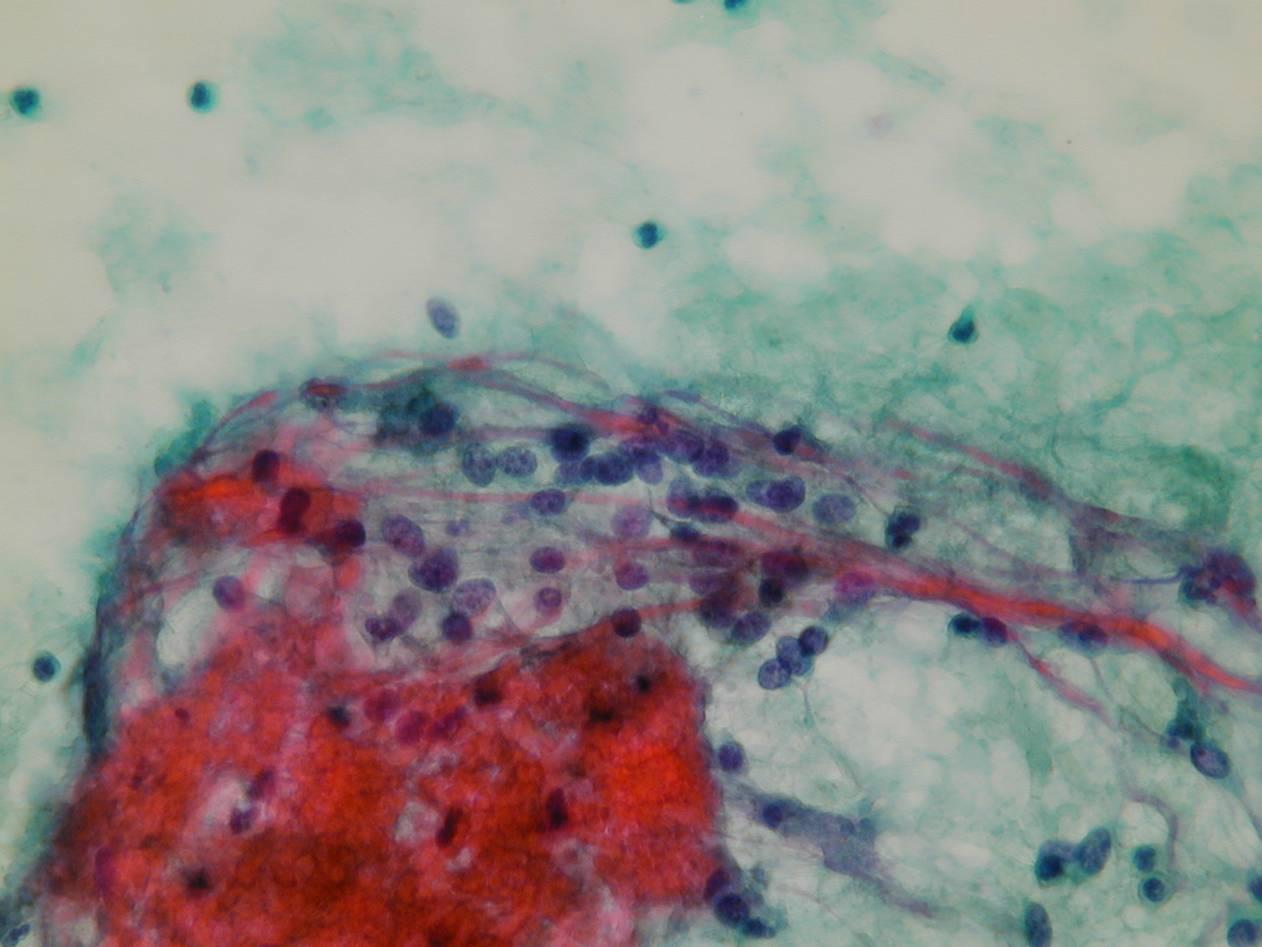
Carcinoid:
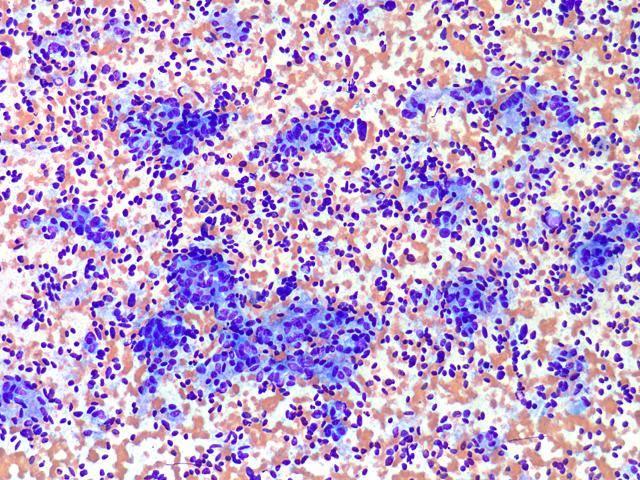
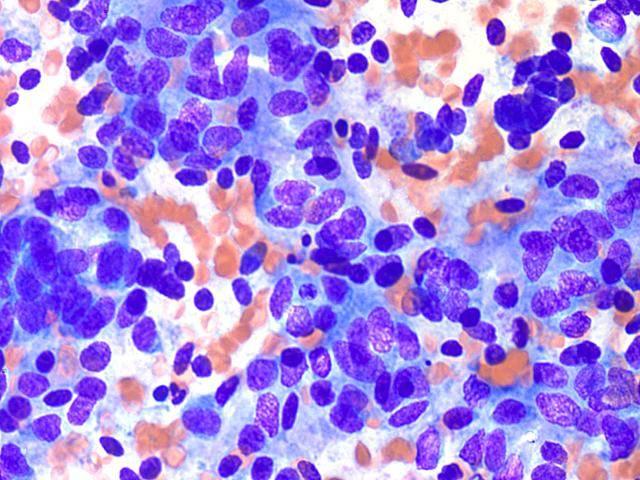
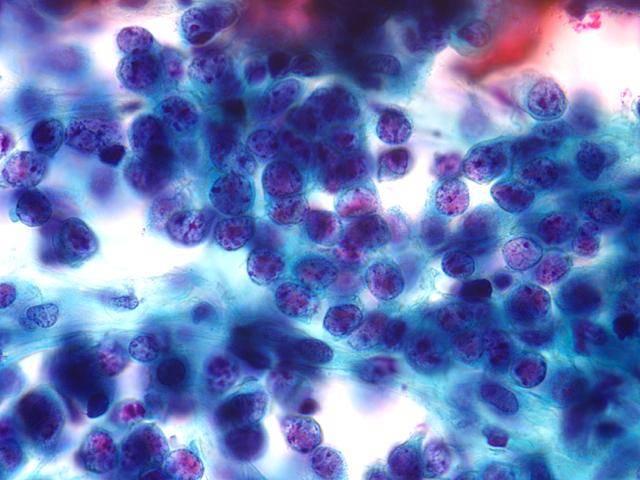
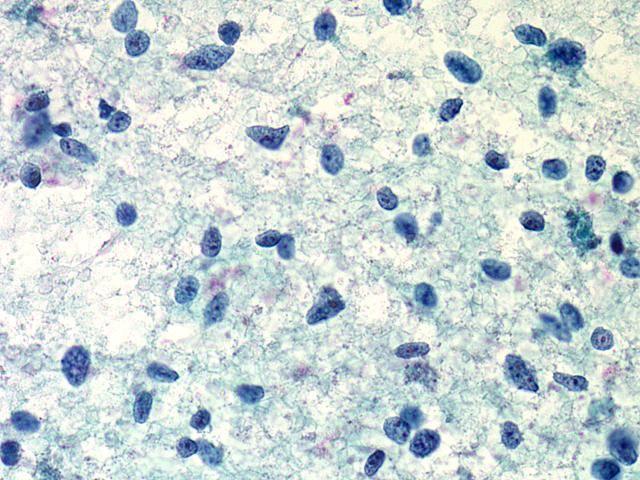
FNA carcinoid: